 J Clin Aesthet Dermatol. 2021;14(8):14–21.
J Clin Aesthet Dermatol. 2021;14(8):14–21.
by James Q. Del Rosso, DO; Guy Webster, MD; Jonathan S. Weiss, MD; Neal D. Bhatia, MD; Linda Stein Gold, MD; and Leon Kircik, MD
Dr. Del Rosso is with JDR Dermatology Research and Thomas Dermatology in Las Vegas, Nevada, and Clinical Research at Advanced Dermatology and Cosmetic Surgery in Maitland, Florida.. Dr. Webster is with Sidney Kimmel Medical College of Thomas Jefferson University in Philadelphia, Pennsylvania. Dr. Weiss is with Georgia Dermatology Partners in Snellville, Georgia. Dr. Bhatia is with Therapeutics Clinical Research in San Diego, California. Dr. Stein Gold is with the Henry Ford Health System in Detroit, Michigan. Dr. Kircik is with Icahn School of Medicine at Mount Sinai in New York, New York.
FUNDING: p-value communications provided medical writing, editing, and publication assistance and was funded by VYNE Therapeutics, Inc.
DISCLOSURES: Dr. Del Rosso has served as a consultant (C), research investigator (RI), and/or speaker (S) for Vyne Therapeutics (C, RI, S), Almirall (C,RI, S), Bausch Health (C, RI, S), BiopharmX (C, S), Galderma (C, RI, S), JEM Health (C), Leo Pharma (C, RI, S), Mayne Pharma (C, S), Novan (C), and Sun Pharma (C,RI,S). Dr. Webster has served as a consultant for VYNE Therapeutics. Dr. Weiss is a speaker for AbbVie, Almirall, Ortho Dermatologics, Regeneron, Sanofi Genzyme; a consultant for Aclaris Therapeutics Inc. and LEO Pharma; an advisor for Dr. Reddy, VYNE Therapeutics Inc., Galderma Laboratories, LP, UCB, Valeant Pharmaceuticals International; and an investigator for AbbVie, Aclaris Therapeutics Inc., Celgene Corporation, Endo International Plc, VYNE Therapeutics Inc., Galderma, LEO Pharma, Moberg Pharma North America LLC, Novartis, Promius Pharma, LLC, and Valeant Pharmaceuticals International. Dr. Bhatia is an investigator and consultant for VYNE Therapeutics. Dr. Stein Gold is an advisor and investigator for VYNE Therapeutics Inc., Galderma, LEO Pharma, Novartis, and Valeant and is an investigator for Janssen, AbbVie, and Solgel. Dr. Kircik is an investigator and consultant for VYNE Therapeutics Inc.
ABSTRACT: Rosacea is one of the most common inflammatory skin diseases in the United States, with a complex pathophysiology. One of the major components of the pathophysiology of rosacea is an abnormal immune detection and response to stimuli. Tetracyclines and their derivatives, including minocycline and doxycycline, have anti-inflammatory properties independent of their antibacterial activity that correlate with certain aspects of the pathophysiology, and these drugs are often used by dermatologists to treat rosacea. Biological actions of tetracyclines correlating with rosacea include anti-inflammatory and antioxidative activities, inhibitory effects on angiogenesis, and proteolysis. The objective of this review is to re-establish the current understanding of tetracyclines and their mechanism of action as they relate to the pathophysiology and treatment of rosacea for clinicians. This includes reviewing the inflammatory aspects of rosacea that correlate with the known nonantibiotic properties of tetracyclines and providing the most up-to-date clinical evidence supporting the use of tetracyclines to treat rosacea. Given the evolving and multifactorial nature of pathophysiology, this review offers clinicians a unified picture that includes research on the links between rosacea pathophysiology and clinical presentation, the nonantibiotic properties of tetracyclines that relate to pathophysiologic pathways in rosacea, and the potential for clinical application of tetracyclines in rosacea therapy.
Keywords: Tetracycline, minocycline, doxycycline, nonantibiotic, rosacea, anti-inflammatory, pathophysiology
Rosacea is one of the most common inflammatory skin diseases, occurring in approximately 16 million people in the United States.1–3 Although it has been reported to occur most commonly in Caucasians, rosacea also affects other populations, including Asian, Black, and Latino individuals.1,4,5 Rosacea is associated with chronic and recurrent inflammation and affects mainly the central facial skin.1,2,6,7 It is a phenotypically heterogeneous disease, characterized by persistent erythema, recurrent flushing (i.e., vasodilation), telangiectasia, and papules and pustules, and it may also trigger ocular findings and phymatous changes.1,2,6,8,9
One of the major clinical challenges with treating rosacea may be that its pathophysiology is complex and multifactorial; therefore, our understanding of the disorder is still developing.6,10 Environmental triggers and genetics are contributory factors, with neurovascular dysregulation and abnormal immune detection and response noted to be the two predominant pathophysiologic components.6,7,11–17 Due to the multifaceted nature of rosacea’s pathophysiology, the clinical presentation is diverse.1,6,7,10 The various phenotypes can overlap, with research suggesting that several manifestations can share the same underlying inflammatory continuum.8,17–20 Tetracyclines and their derivatives, including minocycline and doxycycline, have anti-inflammatory properties that correlate with certain aspects of the pathophysiology of rosacea and are commonly used to treat rosacea.15,21–23
This review focuses on the nonantibiotic properties of tetracyclines and their mechanisms of action (MOA) as they relate to immune dysregulation, with the objective of re-establishing the current understanding of tetracyclines and their MOA in the treatment of rosacea. This will include a discussion highlighting the inflammatory aspects of rosacea that correlate with the activity and known nonantibiotic properties of tetracyclines.
Predisposing Factors, Potential Triggers in Rosacea Pathophysiology, and Immune Dysregulation
Prior to discussing the MOA of tetracyclines, the factors and triggers that may predispose patients to rosacea need to be reviewed. This will enable a more complete understanding of the clinical manifestations of rosacea and the correlation with MOAs of tetracycline derivatives.
Genetics can predispose individuals to the development of rosacea. A study in twins showed higher clinical scores between identical twins versus fraternal twins with rosacea, and a genome-wide association study identified single-nucleotide polymorphisms and the association of three human leukocyte antigen (HLA) alleles in individuals with rosacea compared to controls.12,13 The HLA allele associations have links to other autoimmune diseases and are consistent with the inflammatory nature of the disease.13,24 Although more research is needed, patients with rosacea also have increased expression of a variety of genes with a role in both innate and adaptive immune systems; results are also consistent with laboratory research findings studying dysregulation of the innate immune system in rosacea.7,24
Several additional internal and external factors or triggers contribute to rosacea pathophysiology by stimulating an aberrant innate immune system response.7,24 A variety of these can initiate or exacerbate rosacea, including ultraviolet (UV) radiation (UVR), ambient heat, stress, Demodex mite proliferation, and possibly certain bacterial proteins.2,6,10,25,26 UVR is a recognized trigger for flushing of rosacea and can worsen signs and symptoms; however, the exact mechanism responsible for increased sensitivity to UVR is unknown.7,27 UVR increases levels of reactive oxygen species (ROS) in the skin, which in turn has a proinflammatory effect.7 UV and other environmental stimuli can activate the pattern-recognition system, which includes the Toll-like receptor (TLR) family, with stimulation of cutaneous inflammation.7,28,29 Many patients with rosacea report that environmental and other factors precipitate rosacea flares. The most commonly reported trigger in a survey of 1,066 patients was sun exposure, followed in order of prevalence by stress, heat, wind, heavy exercise, alcohol consumption, and food and beverages.11 The role of microbial sources as external triggers for rosacea remains unclear, with current reports suggesting they are either not mandatory for the development of rosacea or that no direct link has been established.10,15,17,19,25,27–29 Proliferation of Demodex mites, such as Demodex folliculorum, is more prevalent in the skin of patients with rosacea compared to controls, and can provoke a flare by stimulating a dysregulated immune response in selected patients with rosacea, including those with papulopustular rosacea (PPR) and erythematotelangiectatic rosacea (ETR).14,25,26,30
Immune Dysregulation and Rosacea Pathophysiology as They Relate to the Mechanism of Action of Tetracyclines
It is important to review the pathophysiology relevant to the MOA of tetracyclines, especially their nonantibiotic properties. Some of the major sets of nonantibiotic properties are multiple anti-inflammatory effects, such as inhibition of neutrophil chemotaxis and respiratory bursts and inhibition of the matrix metalloproteases (MMPs) that can augment the cathelicidin cascade, one of the dysregulated immune pathways in rosacea.7,21–23,31,32
A hyperresponsive innate immune system has been reported in rosacea-prone skin.6,14,15,28,29,33 Strong experimental support from multiple studies suggests that dysregulation of the innate immune system could unify current clinical observations in rosacea.28 This support includes research reporting increased numbers of innate cells, such as mast cells and macrophages, observed in all major phenotypes of rosacea, with enhanced neutrophil infiltration noted especially in PPR.17,33 In addition, within the inflammatory infiltrate of all rosacea, subtypes of T-cells are activated and proliferate; specifically, T helper cells.33 As a result, the skin has increased susceptibility to triggers, which can provoke an exaggerated immune response.14,24,28,33 Activation of the innate immune system, including neutrophils and mast cells, can then lead to increased production or release of mediators that aggravate the inflammatory cascades, including ROS, antimicrobial peptides, and/or proteases (Figure 1).6,16,29,34,35

Patients with rosacea display higher levels of multiple inflammatory mediators; high levels of ROS and elevated markers for oxidative stress are found in patients with more severe rosacea.7,23 A recent study reported that global measurements for oxidative stress were significantly elevated in patients with rosacea.40 It is therefore clinically relevant that neutrophils play an important role in ROS-mediated inflammatory responses, as tetracycline derivatives can inhibit both neutrophil migration and production of ROS (Figure 1).39
Kallikrein 5 (KLK5), a protease formerly known as stratum corneum tryptic enzyme, and LL-37, of the cathelicidin family, are key contributors to immune dysregulation in rosacea, and are often present at higher baseline levels in rosacea-prone and affected skin. 6,14,28,29,34,42 KLK5 is a serine protease that cleaves an inactive precursor (a cathelicidin precursor, human cathelicidin antimicrobial protein [hCAP18]) into the main active antimicrobial peptide, LL-37, a cathelicidin peptide.29,34,42 LL-37 is stored in neutrophils and in lamellar bodies in keratinocytes.42 Cathelicidins are part of the innate ability for skin to physiologically mount an effective defense against microbial invasion and infection.42 The presence of the human cathelicidin, LL-37, is critical for normal microbial defense and innate immunity within the skin.42,43 Higher baseline levels are found in the skin of patients with rosacea due to abnormal production and excess protease activity.6,28,34,43 The marked overexpression of both KLK5 (a serine protease that cleaves the pre-cathelicidin) and cathelicidin (LL-37) are magnified over what is normally seen physiologically in non-rosacea-prone skin.34 Additionally, in rosacea, there is also production of variant peptides through faulty cleavage of propeptides, which can contribute to the inflammation of the disease.6,15,28,34,44 Other cutaneous findings that correlate with rosacea pathophysiology include an increased expression of TLR2 on keratinocytes, which initiate a pathophysiologic response to environmental triggers.28,29 The enhanced expression of TLR2 leads to increased activity and levels of KLK5 in the epidermis.28,29 This enzyme must first be processed from its inactive proenzyme (pro-KLK5) form; one study supported a role for MMPs in the activation of KLK5.32 These activated KLK5 enzymes in turn increase levels of the active forms of the LL-37 peptide (Figure 1) and other variant peptides.6,15,28,34 Mast cells are also key mediators of the cathelicidin cascade; when LL-37 is injected into mast cell-deficient mice, they do not develop rosacea-like features.35 Moreover, when human mast cells degranulate, they stimulate MMP and KLK enzyme activity from human keratinocyte cells, resulting in enhanced expression of LL-37 and amplification of inflammation.35
High concentrations of LL-37 induce inflammation and vasodilation and increase vascularity in experimental models.15,28,34,35,38,41 In one such model, the peptide LL-37, abundant in the skin of patients with rosacea but not in that of healthy patients, was injected into mice.34 Forty-eight hours following injection, erythema, vascular dilation, and infiltration of neutrophils were reported in the skin of the murine model, characteristic of rosacea. The inflammatory reaction after injection was dose-dependent.34 Similarly, a more recent study addressed the question of why exposure to UVR promotes vascular inflammation in rosacea and the role that LL-37 might play in the process. Patients with rosacea have increased expression of adhesion molecules that are present in UVR-damaged keratinocytes that released double-stranded RNA (dsRNA).27 The expression was not enhanced in the absence of LL-37.27 Enhanced adhesion molecule expression required both dsRNA and LL-37. LL-37 and dsRNA promote leukocyte adhesion and transmigration across the endothelial layer, demonstrating functional relevance. The data from this study provide a framework for understanding the link between UVR damage to keratinocytes and an increase in adhesion molecule expression and sheds light on a previously unknown mechanism that correlates the expression of LL-37 with enhanced sensitivity to UVB radiation in rosacea.27
In summary, LL-37-induced effects include, but are not limited to, leukocyte chemotaxis and angiogenesis, which correlate with morphologic characteristics of facial erythema, telangiectasia, and papules and pustules.15,27,34,38 An increase in the inactive precursor of cathelicidin (hCAP18), combined with proteolytic processing, generates and leads to the accumulation of LL-37 and variant peptides.7,28,34 From a clinical perspective, this enhanced response by the innate immune system, initiated by a trigger with early activation of TLR2, translates to dysregulation of immune detection and response, which leads to several clinical manifestations of rosacea (Figure 1).7,14,29,34
Finally, patients with rosacea have higher levels of certain MMPs.17,23,35,45,46 Involved in extracellular matrix remodeling, MMPs are upregulated in association with UVR damage and inflammation.23,47,48 This is medically relevant, because rosacea is associated with dermal destruction, and patients report sun exposure precipitating rosacea.11,23 Moreover, as previously discussed, MMPs play a role in promoting the cathelicidin cascade by activating the pro-KLK5 enzyme, which ultimately results in the accumulation of higher levels of LL-37 (Figure 1).32,35 MMP levels are reported to be increased not only in cutaneous rosacea but also in ocular rosacea.23,35,45,46 MMP levels have been shown to be higher in the tear fluid of patients with ocular rosacea compared to that of healthy controls.23,45,46,49 The MMP levels in ocular rosacea decreased following doxycycline treatment, which coincided with clinical improvements in the majority of patients.23,45,49
Correlation of Nonantibiotic Mechanisms of Action of Tetracyclines and Rosacea Pathophysiology
Tetracyclines, including minocycline and doxycycline, are antibiotic agents when present in adequate concentrations that are also effective in the treatment of inflammatory skin conditions, such as acne vulgaris (AV) and rosacea.15,31,50,51 Minocycline and doxycycline are second-generation, semisynthetic tetracyclines, effective in treating AV due to their antibacterial and anti-inflammatory properties.15,21,50,52–55 The primary MOA of tetracyclines against bacteria derives from their ability to bind to the bacterial 30S ribosomal subunit and inhibit protein synthesis.21
Multiple studies have focused on the nonantibiotic properties of tetracycline derivatives and their efficacy across multiple disease states unrelated to their antibiotic effects.21,23,32,49,56–61 Many of these disease states are noninfectious in origin, including rheumatoid arthritis, osteoporosis, and dermatologic conditions, including rosacea and bullous pemphigoid.21,23,32,51,57–59,61 The biologic activities of tetracyclines that are not antibiotic-related include anti-inflammatory and antioxidative properties, and inhibitory effects on angiogenesis, granuloma formation, and proteolysis (Table 1).21–23
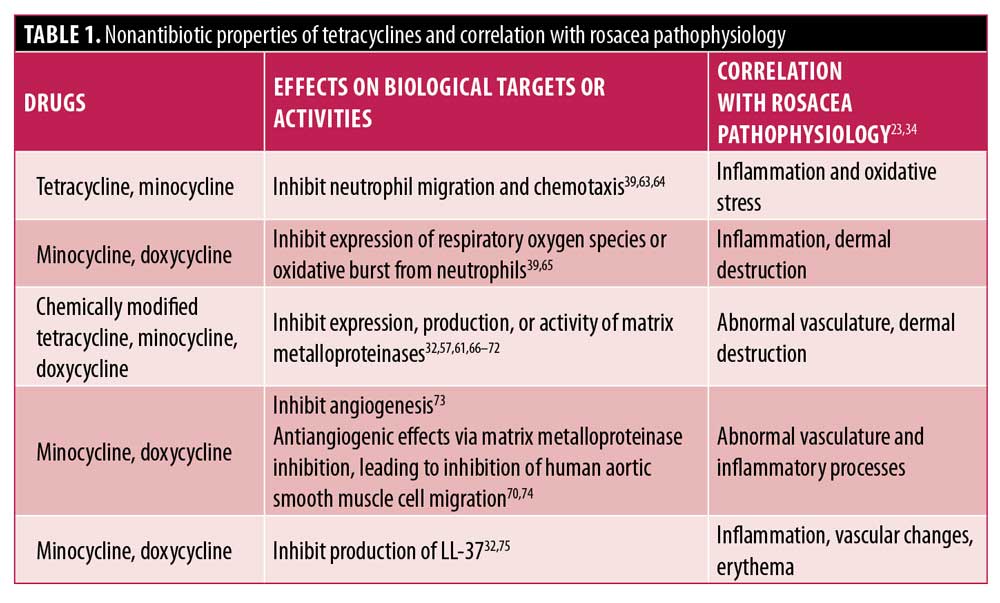
Of the multiple anti-inflammatory properties tetracyclines exhibit, some correlate with the therapeutic activity in rosacea, such as the reduction of cathelicidin expression, inhibition of several MMPs, and inhibition of neutrophil chemotaxis.23,31,45,49,51,61 Therefore, the proposed MOA of tetracyclines in the treatment of rosacea includes three major components: regulation of inflammation via the cathelicidin (LL-37) cascade,15,32,34,62 inhibition of some of the MMPs involved in dermal matrix modulation and angiogenesis,23 and inhibition of neutrophil chemotaxis involved in inflammation and production of ROS (Table 1 and Figure 1).15,21,23,31
Neutrophils. White blood cell recruitment is an early event in inflammation, and neutrophil recruitment is often pivotal in several inflammatory disorders.39,51 Tetracyclines have previously been shown to inhibit neutrophil chemotaxis and migration in vitro (Table 1).63,64 A more recent MOA that correlates with the therapeutic action in rosacea occurred in a human neutrophil model treated with minocycline or doxycycline.39 In this model, minocycline significantly inhibited human neutrophil transendothelial migration, with a maximal effect observed at 100uM (n=5; p<0.001).39 Significant inhibition of oxidative bursts was also observed from 1uM of minocycline treatment (p<0.05), with the maximal effect reported at 300uM (p<0.0001).39 Similarly, doxycycline significantly reduced oxidative bursts from 10uM, with a maximal effect reported at 300uM (p<0.0001). This MOA is clinically relevant, considering that neutrophils are richly present in the skin of patients with PPR and appear to play a role in both cutaneous inflammation and in the oxidative stress associated with rosacea, with patients with rosacea displaying increased levels of ROS and global markers for oxidative stress.7,23,33,39,40
MMPs and LL-37. Tetracyclines and their derivatives have been shown to directly inhibit MMPs in a variety of animal and human cells; inhibition of extracellular activity occurs at least in part through tetracycline binding to zinc and calcium ions.76 The first experiments reporting nonantibiotic activity associated with tetracyclines showed that MMP enzyme activity was reduced in both experimental models and in humans after minocycline treatment.68 More recently, minocycline has been shown to inhibit the activity, expression, and production of MMPs in multiple experimental models and cell types, including in human cells.57,70–72,77
Doxycycline has also been reported to inhibit the expression and production of MMPs in a variety of cell types, including human skin keratinocytes and in human skin.32,66,78,79 An MOA was reported that correlates with therapeutic action in rosacea and occurred in a human keratinocyte model treated with doxycycline. In this model, direct inhibition of MMP activity led to the indirect inhibition of processing and activation of the serine protease KLK5 (Figure 1). This inhibition ultimately resulted in a reduced production of LL-37.32 Similarly, tetracyclines can indirectly inhibit serine proteases, with preliminary data showing that minocycline decreases skin protease activity during treatment.34 Minocycline has also been reported to reduce LL-37 in human cells.75 The study evaluated the effect of minocycline on signaling and LL-37 production in bone marrow-derived mesenchymal stromal/stem cells (MSCs), which have demonstrated prohealing properties, including anti-inflammatory cytokine expression profiles. LL-37 production was significantly decreased in MSCs treated with 100ug/mL of minocycline for 24 hours (p<0.001 vs. MSC control).75
The indirect inhibition of serine proteases that occurs after MMP inhibition is clinically relevant because of the potential role this MOA may play in epidermal barrier homeostasis (Figure 1).7,36 Patients with rosacea report increased skin sensitivity, suggestive of abnormal barrier function, and their skin has increased transepidermal water loss and decreased epidermal hydration.7,37 A study evaluating the role of serine protease signaling in epidermal permeability barrier homeostasis reported that the use of topical serine protease inhibitors accelerated the recovery of the permeability barrier.36 Moreover, patients with PPR who had reduced epidermal hydration and were treated for six weeks with minocycline demonstrated reduced erythema and increased hydration.37 Based on this evidence, it has been proposed that increased serine protease levels in rosacea contribute to the loss of barrier function and that treatment may help restore the function and integrity of the skin barrier (Figure 1).7
The inhibition of MMP activity and the production of LL-37 are also clinically relevant, as inhibition of cathelicidin production by this mechanism would be expected to interfere with several inflammatory cascades responsible for specific clinical manifestations associated with cutaneous rosacea (Figure 1). For example, patients with ocular rosacea display reduced MMP levels that correlate with clinical improvement after treatment with doxycycline and as evidenced by doxycycline normalization of the tear film break-up time.45,49,80 Moreover, patients with PPR treated with doxycycline display reduced biomarker levels of MMP and cathelicidin, and these reduced levels correlated with clinical improvement.61
Clinical Evidence Supports the Use of Tetracyclines, Including Minocycline and Doxycycline, to Treat Rosacea
Regardless of their exact MOA, oral tetracyclines have been used to treat inflammatory lesions of rosacea for several decades, and their use has been associated with clinical improvements in disease manifestations compared to placebo.15,24 Tetracycline derivatives, such as doxycycline and minocycline, have also been used as management options for several other types of rosacea, including granulomatous rosacea and ocular rosacea.1,81
Oral doxycycline. Currently, the only oral tetracycline approved by the United States Food and Drug Administration (FDA) for the treatment of inflammatory lesions of rosacea is subantibiotic-dose doxycycline.15,82–84 Clinical studies leading to FDA approval were conducted using an anti-inflammatory dose of doxycycline that allows for immediate release of 30mg and delayed release of 10mg.82,84 Two Phase III randomized, placebo-controlled, 16-week studies evaluated use of a doxycycline 40-mg modified release capsule once daily for patients with moderate-to-severe papulopustular rosacea.82 In both studies, a significant reduction in the number of baseline inflammatory lesions compared with placebo at Week 16 was observed.
Oral minocycline. Oral minocycline has also shown therapeutic efficacy in rosacea.81,85,86 Published data on the use of low-dose oral minocycline for the treatment of rosacea are limited, with only one known randomized controlled trial utilizing a low-dose extended-release (ER) tablet formulation.15,85 Although not currently approved by the FDA for papulopustular rosacea, an ER minocycline was formulated to avoid the vestibular side effects that are often observed with use of immediate-release (IR) minocycline formulations.85,87 There are no data at this time showing that either IR or ER minocycline formulations provide subantibiotic dosing.85 The efficacy and safety of low-dose oral minocycline (45mg ER) monotherapy and combination therapy with 15% azelaic acid in treating patients with rosacea was evaluated in a randomized, double-blind trial with a 12-week treatment period and four-week follow-up.85 Treatment of patients with either 45mg of ER minocycline, either alone or in combination with topical 15% azelaic acid gel, resulted in significant reductions in inflammatory lesion counts, as well as in Investigator Global Assessment (IGA) and Clinician Erythema Assessment scores over the 16-week study period, with the largest reductions in both arms observed in the interval between baseline and Week 4 (p or lower than 0.0002, all outcomes).85
Oral minocycline versus oral doxycycline. More recently, a head-to-head, noninferiority, randomized, assessor-blinded trial assessed the efficacy and safety of once-daily oral minocycline 100 mg and oral doxycycline 40mg once daily over 16 weeks of treatment in patients with PPR, with a 12-week follow-up period.86 The study showed that, over the 16-week treatment period, 100mg of minocycline was noninferior to 40mg of doxycycline in terms of efficacy, and that minocycline and doxycycline exhibited comparable safety profiles.86 Although outcomes were comparable at Week 28, patient-reported outcomes, as assessed by Patient Global Assessment and Rosacea-specific Quality-of-life scores, were significantly different in favor of minocycline (p=0.043 and p=0.005, respectively).86 Furthermore, at the 12-week follow-up, significantly fewer patients with rosacea had a relapse in the minocycline treatment group (7% vs. 48%; p<0.001).86 Importantly, oral minocycline might be associated with specific adverse reactions not typically observed with oral doxycycline, including vertigo, hyperpigmentation, drug hypersensitivity syndrome, and less commonly, autoimmune reactions (e.g., hepatitis, lupus-like syndrome).15,21,87 Oral doxycycline is more commonly associated with gastrointestinal side effects and dose-related phototoxicity, although these adverse effects (AEs) are markedly reduced with a subantibiotic-dose doxycycline (40mg) modified-release capsule taken once daily.15,82,87
Some patients treated with oral tetracyclines might experience AEs.15,88 Overall, oral doxycycline has been reported to be associated with fewer AEs compared to oral minocycline.87 The incidence of AEs was low with either drug relative to the number of prescriptions dispensed; however, fewer AEs were reported with doxycycline.87
Topical minocycline 1.5%. Minocycline foam 1.5% is a novel topical formulation of micronized minocycline, developed and recently approved to treat inflammatory lesions of rosacea.89–91 The foam vehicle is composed primarily of natural plant oils selected for their ability to protect minocycline from degradation and which have been shown to have beneficial effects on the skin barrier.89 Pharmacokinetic, ex-vivo studies demonstrated that high concentrations of minocycline are delivered to the epidermis and dermis with negligible systemic exposure.89 As a result, minocycline foam 1.5% avoids the potential for AEs associated with oral minocycline use.89,92 The high cutaneous concentrations of minocycline achieved with topical foam formulation (330ug/mL in the epidermis and 15ug/mL in the dermis) might circumvent antibiotic resistance based on an evaluation of mutant protection concentrations of minocycline.55,89
One Phase II and two pivotal Phase III trials led to the FDA approval of topical minocycline foam 1.5% for the treatment of papulopustular rosacea.90,91,93 The two Phase III trials were identical 12-week, randomized, multicenter, vehicle-controlled Phase III studies with minocycline foam 1.5% conducted in patients with moderate-to-severe PPR, Study 11 (FX2016-11) and Study 12 (FX2016-12).91 Both studies showed a significant reduction in the number of inflammatory lesions relative to vehicle at Week 12 (Study 11: -17.57 vs. -15.65; p=0.0031 and Study 12: -18.54 vs. -14.88; p<0.0001). The absolute reduction in inflammatory lesions compared to vehicle was significant as early as Week 4 (Study 11: -11.19 vs. -8.79; p=0.0004 and Study 12: -12.90 vs. -8.74; p<0.001) and continued throughout Week 12. No serious treatment-emergent AEs (TEAEs) were reported in either study, and only one discontinuation was considered related to treatment across both studies (pruritus). Of the 1,008 patients who received at least one dose of minocycline foam 1.5%, more than 95 percent reported no or only mild issues with skin tolerability.91 After the 12-week study period, once-daily application of minocycline 1.5% foam was deemed effective, safe, and well tolerated for the treatment of moderate-to-severe PPR.91
An open-label extension study evaluated minocycline foam 1.5% for a total of up to 52 weeks of treatment.92 The severity and frequency of local tolerability reactions reported at Week 52 were comparable to those at Week 12.90,92 None of the major systemic AEs associated with oral minocycline, such as vertigo, cutaneous hyperpigmentation, or autoimmune side effects, were observed with minocycline foam 1.5% in this extension study, with no serious treatment-emergent AEs.92 During the additional 40 weeks of treatment, long-term efficacy data showed that minocycline foam 1.5% treatment was associated with a progressive decrease in the number of inflammatory lesions as well as an improvement in overall IGA treatment success.92
Additional research considerations. In a carefully designed laboratory model, tetracyclines have been shown to inhibit granuloma formation via modulation of protein kinase C.94 This may potentially correlate with therapeutic benefit for granulomatous rosacea, although more data are needed.
Conclusion
Rosacea is one of the most common inflammatory skin diseases in the United States, with a complex pathophysiology. Although immune detection and response to stimuli are normal responses in healthy human skin, this part of the immune pathway is dysfunctional in cutaneous rosacea and the inflammatory response ultimately causes damage. This dysregulation includes activation of the innate immune system, which might then lead to increased production or release of mediators that aggravate the inflammatory cascade. Some of the nonantibiotic properties of tetracyclines correlate with therapeutic activity in rosacea, such as the suppression or reduction of some of these mediators, including cathelicidin expression, inhibition of some MMPs, and the inhibition of neutrophil chemotaxis. Our understanding of all the aspects of the MOA of tetracyclines in rosacea is still evolving. Regardless of their exact MOA, tetracyclines, such as doxycycline and minocycline, improve the clinical outcomes in patients with PPR.
Acknowledgments
Manuscript preparation assistance was provided by Scient Healthcare Communications, supported by VYNE Therapeutics.
References
- Del Rosso JQ, Tanghetti E, Webster G, Stein Gold L, Thiboutot D, Gallo RL. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). J Clin Aesthet Dermatol. 2019;12(6):17–24.
- Thiboutot D, Anderson R, Cook-Bolden F, et al. Standard management options for rosacea: the 2019 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2020;82(6):1501–1510.
- Li WQ, Cho E, Khalili H, Wu S, Chan AT, Qureshi AA. Rosacea, use of tetracycline, and risk of incident inflammatory bowel disease in women. Clin Gastroenterol Hepatol. 2016;14(2):220–225.e221–223.
- Al-Dabagh A, Davis SA, McMichael AJ, Feldman SR. Rosacea in skin of color: not a rare diagnosis. Dermatol Online J. 2014;20(10):13030/qt13031mv13039r13030ss.
- Tan J, Schofer H, Araviiskaia E, et al. Prevalence of rosacea in the general population of Germany and Russia—the RISE study. J Eur Acad Dermatol Venereol. 2016;30(3):428–434.
- Ahn CS, Huang WW. Rosacea pathogenesis. Dermatol Clin. 2018;36(2):81–86.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: part I. Introduction, categorization, histology, pathogenesis, and risk factors. J Am Acad Dermatol. 2015;72(5):749–758; quiz 759–760.
- Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: the 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78(1):148–155.
- van Zuuren EJ, Fedorowicz Z, Tan J, et al. Interventions for rosacea based on the phenotype approach: an updated systematic review including GRADE assessments. Br J Dermatol. 2019;181(1):65–79.
- Buddenkotte J, Steinhoff M. Recent advances in understanding and managing rosacea. F1000Res. 2018;7:F100 Faculty Rev-1885.
- National Rosacea Society. Rosacea triggers survey. Available at: www.rosacea.org/patients/rosacea-triggers/rosacea-triggers-survey. Accessed January 19, 2021.
- Aldrich N, Gerstenblith M, Fu P, et al. Genetic vs environmental factors that correlate with rosacea: a cohort-based survey of twins. JAMA Dermatol. 2015;151(11):1213–1219.
- Chang ALS, Raber I, Xu J, et al. Assessment of the genetic basis of rosacea by genome-wide association study. J Invest Dermatol. 2015;135(6):1548–1555.
- Del Rosso JQ, Gallo RL, Kircik L, et al. Why is rosacea considered to be an inflammatory disorder? The primary role, clinical relevance, and therapeutic correlations of abnormal innate immune response in rosacea-prone skin. J Drugs Dermatol. 2012;11(6):694–700.
- Del Rosso JQ, Thiboutot D, Gallo R, et al. Consensus recommendations from the American Acne & Rosacea Society on the management of rosacea, part 3: a status report on systemic therapies. Cutis. 2014;93(1):18–28.
- Steinhoff M, Buddenkotte J, Aubert J, et al. Clinical, cellular, and molecular aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):2–11.
- Schwab VD, Sulk M, Seeliger S, et al. Neurovascular and neuroimmune aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011;15(1):53–62.
- Seeliger S, Buddenkotte J, Schmidt-Choudhury A, et al. Pituitary adenylate cyclase activating polypeptide: an important vascular regulator in human skin in vivo. Am J Pathol. 2010;177(5):2563–2575.
- Sulk M, Seeliger S, Aubert J, et al. Distribution and expression of non-neuronal transient receptor potential (TRPV) ion channels in rosacea. J Invest Dermatol. 2012;132(4): 1253–1262.
- Wladis EJ, Iglesias BV, Adam AP, Gosselin EJ. Molecular biologic assessment of cutaneous specimens of ocular rosacea. Ophthalmic Plast Reconstr Surg. 2012;28(4):246–250.
- Garrido-Mesa N, Zarzuelo A, Gálvez J. Minocycline: far beyond an antibiotic. Br J Pharmacol. 2013;169(2):337–352.
- Garrido-Mesa N, Zarzuelo A, Gálvez J. What is behind the non-antibiotic properties of minocycline? Pharmacol Res. 2013;67(1): 18–30.
- Monk E, Shalita A, Siegel DM. Clinical applications of non-antimicrobial tetracyclines in dermatology. Pharmacol Res. 2011;63(2):130–145.
- Rainer BM, Kang S, Chien AL. Rosacea: epidemiology, pathogenesis, and treatment. Dermatoendocrinol. 2017;9(1):e1361574.
- Ellis SR, Nguyen M, Vaughn AR, et al. The skin and gut microbiome and its role in common dermatologic conditions. Microorganisms. 2019;7(11):550.
- McMahon F, Banville N, Bergin DA, et al. Activation of neutrophils via IP3 pathway following exposure to Demodex-associated bacterial proteins. Inflammation. 2016;39(1):425–433.
- Kulkarni NN, Takahashi T, Sanford JA, et al. Innate immune dysfunction in rosacea promotes photosensitivity and vascular adhesion molecule expression. J Invest Dermatol. 2020;140(3):645–655.e646.
- Yamasaki K, Gallo RL. Rosacea as a disease of cathelicidins and skin innate immunity. J Investig Dermatol Symp Proc. 2011;15(1): 12–15.
- Yamasaki K, Kanada K, Macleod DT, et al. TLR2 expression is increased in rosacea and stimulates enhanced serine protease production by keratinocytes. J Invest Dermatol. 2011;131(3):688–697.
- Chang YS, Huang YC. Role of Demodex mite infestation in rosacea: a systematic review and meta-analysis. J Am Acad Dermatol. 2017;77(3):441–447.e446.
- Sapadin AN, Fleischmajer R. Tetracyclines: nonantibiotic properties and their clinical implications. J Am Acad Dermatol. 2006;54(2):258–265.
- Kanada KN, Nakatsuji T, Gallo RL. Doxycycline indirectly inhibits proteolytic activation of tryptic kallikrein-related peptidases and activation of cathelicidin. J Invest Dermatol. 2012;132(5):1435–1442.
- Buhl T, Sulk M, Nowak P, et al. Molecular and morphological characterization of inflammatory Iinfiltrate in rosacea reveals activation of Th1/Th17 pathways. J Invest Dermatol. 2015;135(9):2198–2208.
- Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007;13(8):975–980.
- Muto Y, Wang Z, Vanderberghe M, et al. Mast cells are key mediators of cathelicidin-initiated skin inflammation in rosacea. J Invest Dermatol. 2014;134(11):2728–2736.
- Hachem JP, Houben E, Crumrine D, et al. Serine protease signaling of epidermal permeability barrier homeostasis. J Invest Dermatol. 2006;126(9):2074–2086.
- Raghallaigh SN, Powell FC. Epidermal hydration levels in patients with rosacea improve after minocycline therapy. Br J Dermatol. 2014;171(2):259–266.
- Koczulla R, von Degenfeld G, Kupatt C, et al. An angiogenic role for the human peptide antibiotic LL-37/hCAP-18. J Clin Invest. 2003;111(11):1665–1672.
- Parenti A, Indorato B, Paccosi S. Minocycline affects human neutrophil respiratory burst and transendothelial migration. Inflamm Res. 2017;66(2):107–109.
- Erdogan HK, Bulur I, Kocaturk E, et al. Advanced oxidation protein products and serum total oxidant/antioxidant status levels in rosacea. Postepy Dermatol Alergol. 2018;35(3):304–308.
- Braff MH, Hawkins MA, Di Nardo A, et al. Structure-function relationships among human cathelicidin peptides: dissociation of antimicrobial properties from host immunostimulatory activities. J Immunol. 2005;174(7):4271–4278.
- Yamasaki K, Schauber J, Coda A, et al. Kallikrein-mediated proteolysis regulates the antimicrobial effects of cathelicidins in skin. FASEB J. 2006;20(12):2068–2080.
- Reinholz M, Ruzicka T, Schauber J. Cathelicidin LL-37: an antimicrobial peptide with a role in inflammatory skin disease. Ann Dermatol. 2012;24(2):126–135.
- Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci. 2009;55(2):77–81.
- Maatta M, Kari O, Tervahartiala T, et al. Tear fluid levels of MMP-8 are elevated in ocular rosacea—treatment effect of oral doxycycline. Graefes Arch Clin Exp Ophthalmol. 2006;244(8):957–962.
- Afonso AA, Sobrin L, Monroy DC, et al. Tear fluid gelatinase B activity correlates with IL-1alpha concentration and fluorescein clearance in ocular rosacea. Invest Ophthalmol Vis Sci. 1999;40(11):2506–2512.
- Jung SK, Lee KW, Kim HY, et al. Myricetin suppresses UVB-induced wrinkle formation and MMP-9 expression by inhibiting Raf. Biochem Pharmacol. 2010;79(10):1455–1461.
- Cui N, Hu M, Khalil RA. Biochemical and biological attributes of matrix metalloproteinases. Prog Mol Biol Transl Sci. 2017;147:1–73.
- Lam-Franco L, Perfecto-Avalos Y, Patiño-Ramírez BE, Rodríguez García A. IL-1alpha and MMP-9 tear levels of patients with active ocular rosacea before and after treatment with systemic azithromycin or doxycycline. Ophthalmic Res. 2018;60(2):109–114.
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5): 945–973.e933.
- Webster G, Del Rosso JQ. Anti-inflammatory activity of tetracyclines. Dermatol Clin. 2007;25(2):133-135, v.
- Garner SE, Eady A, Bennett C, Newton JN, Thomas K, Popescu CM. Minocycline for acne vulgaris: efficacy and safety. Cochrane Database Syst Rev. 2012(8):CD002086.
- Ochsendorf F. Minocycline in acne vulgaris: benefits and risks. Am J Clin Dermatol. 2010;11(5):327-341.
- Raoof TJ, Hooper D, Moore A, et al. Efficacy and safety of a novel topical minocycline foam for the treatment of moderate to severe acne vulgaris: a phase 3 study. J Am Acad Dermatol. 2020;82(4):832–837.
- Sutcliffe J, McLaughlin R, Webster G, et al. Susceptibility of Cutibacterium acnes to topical minocycline foam. Anaerobe. 2020;62:102169.
- Furlong-Silva J, Cross SD, Marriott AE, et al. Tetracyclines improve experimental lymphatic filariasis pathology by disrupting interleukin-4 receptor-mediated lymphangiogenesis. J Clin Invest. 2021;131(5):140853.
- Kim Y, Kim J, Lee H, et al. Tetracycline analogs inhibit osteoclast differentiation by suppressing MMP-9-mediated histone H3 cleavage. Int J Mol Sci. 2019;20(16):4038.
- Nakagawa T, Kakizoe Y, Iwata Y, et al. Doxycycline attenuates cisplatin-induced acute kidney injury through pleiotropic effects. Am J Physiol Renal Physiol. 2018;315(5):
F1347–F1357. - Vellimana AK, Zhou ML, Singh I, et al. Minocycline protects against delayed cerebral ischemia after subarachnoid hemorrhage via matrix metalloproteinase-9 inhibition. Ann Clin Transl Neurol. 2017;4(12):865–876.
- Webster GF, Toso SM, Hegemann L. Inhibition of a model of in vitro granuloma formation by tetracyclines and ciprofloxacin. Involvement of protein kinase C. Arch Dermatol. 1994;130(6):748–752.
- Di Nardo A, Holmes AD, Muto Y, et al. Improved clinical outcome and biomarkers in adults with papulopustular rosacea treated with doxycycline modified-release capsules in a randomized trial. J Am Acad Dermatol. 2016;74(6):1086–1092.
- Bevins CL, Liu FT. Rosacea: skin innate immunity gone awry? Nat Med. 2007;13(8):904–906.
- Esterly NB, Furey NL, Flanagan LE. The effect of antimicrobial agents on leukocyte chemotaxis. J Invest Dermatol. 1978;70(1):51–55.
- Esterly NB, Koransky JS, Furey NL, Trevisan M. Neutrophil chemotaxis in patients with acne receiving oral tetracycline therapy. Arch Dermatol. 1984;120(10):1308–1313.
- Takeshita S, Ono Y, Kozuma K, et al. Modulation of oxidative burst of neutrophils by doxycycline in patients with acute myocardial infarction. J Antimicrob Chemother. 2002;49(2):411–413.
- Hanemaaijer R, Visser H, Koolwijk P, et al. Inhibition of MMP synthesis by doxycycline and chemically modified tetracyclines (CMTs) in human endothelial cells. Adv Dent Res. 1998;12(2):114–118.
- Guimaraes DA, Rizzi E, Ceron CS, et al. Doxycycline dose-dependently inhibits MMP-2-mediated vascular changes in 2K1C hypertension. Basic Clin Pharmacol Toxicol. 2011;108(5):318–325.
- Golub LM, Lee HM, Lehrer G, et al. Minocycline reduces gingival collagenolytic activity during diabetes. Preliminary observations and a proposed new mechanism of action. J Periodontal Res. 1983;18(5):516–526.
- Brundula V, Rewcastle NB, Metz LM, Bernard CC, Yong VW. Targeting leukocyte MMPs and transmigration: minocycline as a potential therapy for multiple sclerosis. Brain. 2002;125(Pt 6):1297–1308.
- Yao JS, Chen Y, Zhai W, et al. Minocycline exerts multiple inhibitory effects on vascular endothelial growth factor-induced smooth muscle cell migration: the role of ERK1/2, PI3K, and matrix metalloproteinases. Circ Res. 2004;95(4):364–371.
- Machado LS, Kozak A, Ergul A, et al. Delayed minocycline inhibits ischemia-activated matrix metalloproteinases 2 and 9 after experimental stroke. BMC Neurosci. 2006;7:56.
- Ali S, Driscoll HE, Newton VL, Gardiner NJ. Matrix metalloproteinase-2 is downregulated in sciatic nerve by streptozotocin induced diabetes and/or treatment with minocycline: implications for nerve regeneration. Exp Neurol. 2014;261:654–665.
- Tamargo RJ, Bok RA, Brem H. Angiogenesis inhibition by minocycline. Cancer Res. 1991;51(2):672–675.
- Yao JS, Shen F, Young WL, Yang GY. Comparison of doxycycline and minocycline in the inhibition of VEGF-induced smooth muscle cell migration. Neurochem Int. 2007;50(3): 524–530.
- Guerra AD, Rose WE, Hematti P, Kao WJ. Minocycline modulates NFkappaB phosphorylation and enhances antimicrobial activity against Staphylococcus aureus in mesenchymal stromal/stem cells. Stem Cell Res Ther. 2017;8(1):171.
- Golub LM, Lee HM, Ryan ME, et al. Tetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanisms. Adv Dent Res. 1998;12(2):12–26.
- Masumori N, Tsukamoto T, Miyao N, et al. Inhibitory effect of minocycline on in vitro invasion and experimental metastasis of mouse renal adenocarcinoma. J Urol. 1994;151(5):1400–1404.
- Li DQ, Chen Z, Song XJ, Luo L, Pflugfelder SC. Stimulation of matrix metalloproteinases by hyperosmolarity via a JNK pathway in human corneal epithelial cells. Invest Ophthalmol Vis Sci. 2004;45(12):4302–4311.
- Uitto VJ, Firth JD, Nip L, Golub LM. Doxycycline and chemically modified tetracyclines inhibit gelatinase A (MMP-2) gene expression in human skin keratinocytes. Ann N Y Acad Sci. 1994;732:140–151.
- Quarterman MJ, Johnson DW, Abele DC, et al. Ocular rosacea. Signs, symptoms, and tear studies before and after treatment with doxycycline. Arch Dermatol. 1997;133(1): 49–54.
- Ta CN, Shine WE, McCulley JP, et al. Effects of minocycline on the ocular flora of patients with acne rosacea or seborrheic blepharitis. Cornea. 2003;22(6):545–548.
- Del Rosso JQ, Webster GF, Jackson M, et al. Two randomized phase III clinical trials evaluating anti-inflammatory dose doxycycline (40-mg doxycycline, USP capsules) administered once daily for treatment of rosacea. J Am Acad Dermatol. 2007;56(5):791–802.
- Fowler JF, Jr. Combined effect of anti-inflammatory dose doxycycline (40-mg doxycycline, usp monohydrate controlled-release capsules) and metronidazole topical gel 1% in the treatment of rosacea. J Drugs Dermatol. 2007;6(6):641–645.
- Oracea [prescribing information]. Fort Worth, TX: Galderma Laboratories, LP; December 2014.
- Jackson JM, Kircik LH, Lorenz DJ. Efficacy of extended-release 45 mg oral minocycline and extended-release 45 mg oral minocycline plus 15% azelaic acid in the treatment of acne rosacea. J Drugs Dermatol. 2013;12(3): 292–298.
- van der Linden MMD, van Ratingen AR, van Rappard DC, Nieuwenburg SA, Spuls PI. DOMINO, doxycycline 40 mg vs. minocycline 100 mg in the treatment of rosacea: a randomized, single-blinded, noninferiority trial, comparing efficacy and safety. Br J Dermatol. 2017;176(6):1465–1474.
- Smith K, Leyden JJ. Safety of doxycycline and minocycline: a systematic review. Clin Ther. 2005;27(9):1329–1342.
- Oge LK, Muncie HL, Phillips-Savoy AR. Rosacea: diagnosis and treatment. Am Fam Physician. 2015;92(3):187–196.
- Kircik L, Del Rosso JQ, Weiss JS, et al. Formulation and profile of FMX101 4% minocycline topical foam for the treatment of acne vulgaris. J Clin Aesthet Dermatol. 2020;13(4):14–21.
- ZILXI (minocycline) topical foam, 1.5% [prescribing information]. Bridgewater, NJ: Foamix Pharmaceuticals Inc.; May 2020.
- Gold LS, Del Rosso JQ, Kircik L, et al. Minocycline 1.5% foam for the topical treatment of moderate to severe papulopustular rosacea: results of 2 phase 3, randomized, clinical trials. J Am Acad Dermatol. 2020;82(5):1166–1173.
- Stein Gold L, Del Rosso JQ, Kircik L, et al. Open-label extension study evaluating long-term safety and efficacy of FMX103 1.5% minocycline topical foam for the treatment of moderate-to-severe papulopustular rosacea. J Clin Aesthet Dermatol. 2020;13(11):44–49.
- Mrowietz U, Kedem TH, Keynan R, et al. A phase II, randomized, double-blind clinical study evaluating the safety, tolerability, and efficacy of a topical minocycline foam, FMX103, for the treatment of facial papulopustular rosacea. Am J Clin Dermatol. 2018;19(3):427–436.
- Webster GF, Toso SM, Hegeman L: Inhibition of a model of granuloma formation by tetracyclines and ciprofloxacin: Involvement of protein kinase C. Arch Dermatol .1994;130:748–752.