J Clin Aesthet Dermatol. 2026;19(3):42–46.
by Vixey Silva, DO; Lisa Fronek, DO; Travis Blalock, MD; and Emily Coughlin, MPH, CPH
Dr. Silva is with the Department of Dermatology, HCA Healthcare/USF Morsani College of Medicine: Largo Medical Center Program, Largo, Florida. Dr. Fronek is with Scripps Clinic Torrey Pines Bighorn Mohs Surgery and Dermatology, San Diego, California. Dr. Blalock is with the Department of Dermatology at the Emory University School of Medicine, Atlanta, Georgia. Ms. Coughlin is with the Department of Medical Education at the University of South Florida, Tampa, Florida.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no relevant conflicts of interest.
ABSTRACT: Objective: This paper seeks to characterize Mohs surgeons’ postoperative wound care practices for secondary intention healing (SIH) and identify trends in the use of topical agents and perceived clinical outcomes. Methods: A survey was distributed to American College of Mohs Surgery (ACMS) members to assess demographics, practice settings, wound care preferences, and self-reported outcomes related to SIH. Fisher’s exact and χ2 tests were used to evaluate associations between surgeon characteristics and wound care practices. Results: Petroleum emollients were used by 96.4% of respondents. Topical antibiotics, most commonly mupirocin and gentamicin, were routinely recommended by 36.1% and were associated with higher reported infection rates (P=0.034). Antiseptic solutions, particularly dilute acetic acid, were more often used by early-career surgeons (P=0.016). Only 10.8% of respondents used topical timolol. Conventional nonadherent dressings were preferred by 91.6% of respondents. Most surgeons reported complete healing within 4 to 8 weeks (72.3%), 95.2% of surgeons indicated infection rates of 5% or less, and 95.2% reported good to excellent cosmetic outcomes. Limitations: Low response rate and self-reported data limited generalizability. Wound location data were not stratified. Conclusion: Postoperative care practices for SIH vary considerably among Mohs surgeons. Despite supporting literature, the use of advanced dressings, antiseptics, and topical timolol remains limited. These findings highlight opportunities for further research and standardization of SIH wound care. Keywords: Mohs micrographic surgery, secondary intention healing, postoperative wound care, topical antibiotics, antiseptics, hydrocolloid dressings, timolol, surgical site infection
Introduction
Mohs micrographic surgery (MMS) is the preferred treatment for high-risk keratinocyte carcinomas, with recurrence rates of 4.4% for primary basal cell carcinomas and 3.1% for primary squamous cell carcinomas.1,2 Postremoval repair options include primary closure, grafts, flaps, and secondary intention healing (SIH). SIH, where wounds heal by granulation, often yields comparable or superior results to traditional reconstructive techniques, particularly on concave surfaces.3 As SIH is used in approximately 25% of postdermatologic surgical defects, optimizing postoperative wound care is crucial for improving outcomes.3,4
A moist environment is essential for rapid healing, promoting keratinocyte migration and collagen synthesis while reducing necrosis and scarring.5,6 Petroleum jelly is the most recommended emollient by dermatologic surgeons, with a lower risk of contact dermatitis compared to alternatives like Aquaphor (Beiersdorf Inc.).5 Impermeable occlusive dressings also promote a favorable healing environment. Hydrocolloid dressings (HCD) have shown benefits in reducing infection rates while improving patient satisfaction and comfort compared to conventional nonadherent dressings (CND).7,8
Guidelines advise against routine use of topical antibiotics postoperatively due to risks of bacterial resistance and contact dermatitis.5,6 Studies show that topical petrolatum yields similar infection rates compared to bacitracin and mupirocin in clean postoperative wounds, with lower risk of allergic contact dermatitis.9,10 Despite this evidence, a 2013 survey of American College of Mohs Surgery (ACMS) members found that surgeons still recommend topical antibiotics.5
Topical antiseptics may reduce surgical site infections (SSI) and promote wound healing in SIH, though data on postoperative use in MMS are limited. Low-concentration povidone iodine in a petroleum base enhanced wound healing in rats by reducing inflammation, irritation, and bleeding, while hydrogen peroxide can promote granulation tissue growth and decrease healing time.11-13 Diluted acetic acid has shown effectiveness in healing MMS wounds with hypergranulation tissue and decolonizing burn wounds from Pseudomonas.14,15 Chlorhexidine may also benefit SIH; daily bathing reduced hospital-acquired infections and preoperative application decreased SSI rates in lower extremity procedures.16,17
Topical timolol promotes wound healing through multiple mechanisms, including keratinocyte migration stimulation and inflammation reduction.18,19 Studies have demonstrated that it can halve repair time in dermatologic wounds and significantly reduce healing time in chronix lower leg wounds.18,19
Despite these advancements, data on common practices and outcomes for Mohs surgical defects healing by SIH remain limited. This study aims to characterize current wound care practices among Mohs surgeons to identify areas for standardization.
Methods
A 16-question survey was developed by the authors to assess postoperative MMS wound care practices and outcomes for SIH among ACMS members. The survey was approved by the HCA Healthcare Institutional Review Board and by the ACMS Executive Committee. It was distributed to all ACMS members via email in August 2024, with a 6-week data collection period. Participation in the study was voluntary and anonymous.
The survey assessed demographics, practice settings, wound care practices, and clinical outcomes related to SIH after MMS. Survey items were primarily closed-ended questions (yes/no, multiple choice, and “select all that apply” formats), with limited optional free-text responses for “other” selections, including practice location, practice setting, years of experience, preferred topical agents, dressing types, and perceptions of healing time, infection rates, and cosmetic outcomes. Healing was defined as complete re-epithelialization based on surgeon judgment, while infection was determined by symptoms such as erythema or drainage or by culture-proven bacterial infection requiring antibiotic treatment. No standardized definitions or body site stratification were applied.
Survey responses were summarized using frequencies and proportions. Fisher’s exact and χ2 tests (for expected cell counts <5) were used to compare provider characteristics and outcomes of interest. A significance level of 0.05 was applied. Analysis was performed using SPSS version 29.
Results
The survey received 83 responses of a potential 1,500 (5.5% response rate). Respondents practiced in various settings: 7.2% in rural areas, 55.4% in suburban environments, and 37.3% in urban locations (Table 1). Practice settings included single-specialty groups (51.8%), academic (20.5%), single private (16.9%), and multispecialty groups (10.8%). The distribution of years of practice among respondents was diverse and nearly evenly spread: 25.3% had been in practice for 0 to 5 years, 18.1% for 6 to 10 years, 26.5% for 11 to 20 years, and 30.1% for more than 20 years.
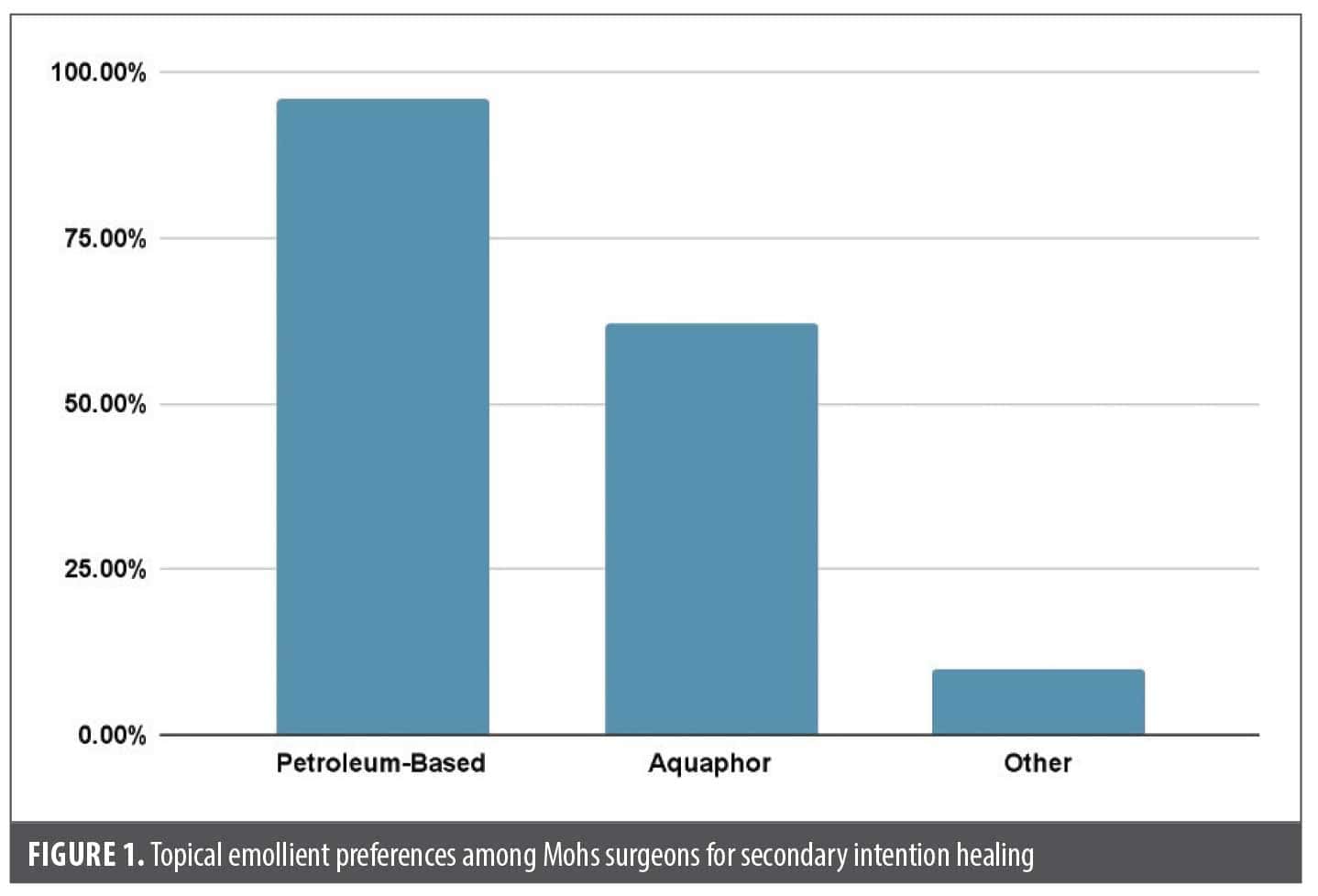
Emollients. All respondents reported using topical emollients, with 96.4% using petroleum jelly and 62.7% using Aquaphor (Figure 1). Ten percent selected “other,” specifying alternatives such as CeraVe Healing Ointment (CeraVe LLC) and silicone-based ointments.
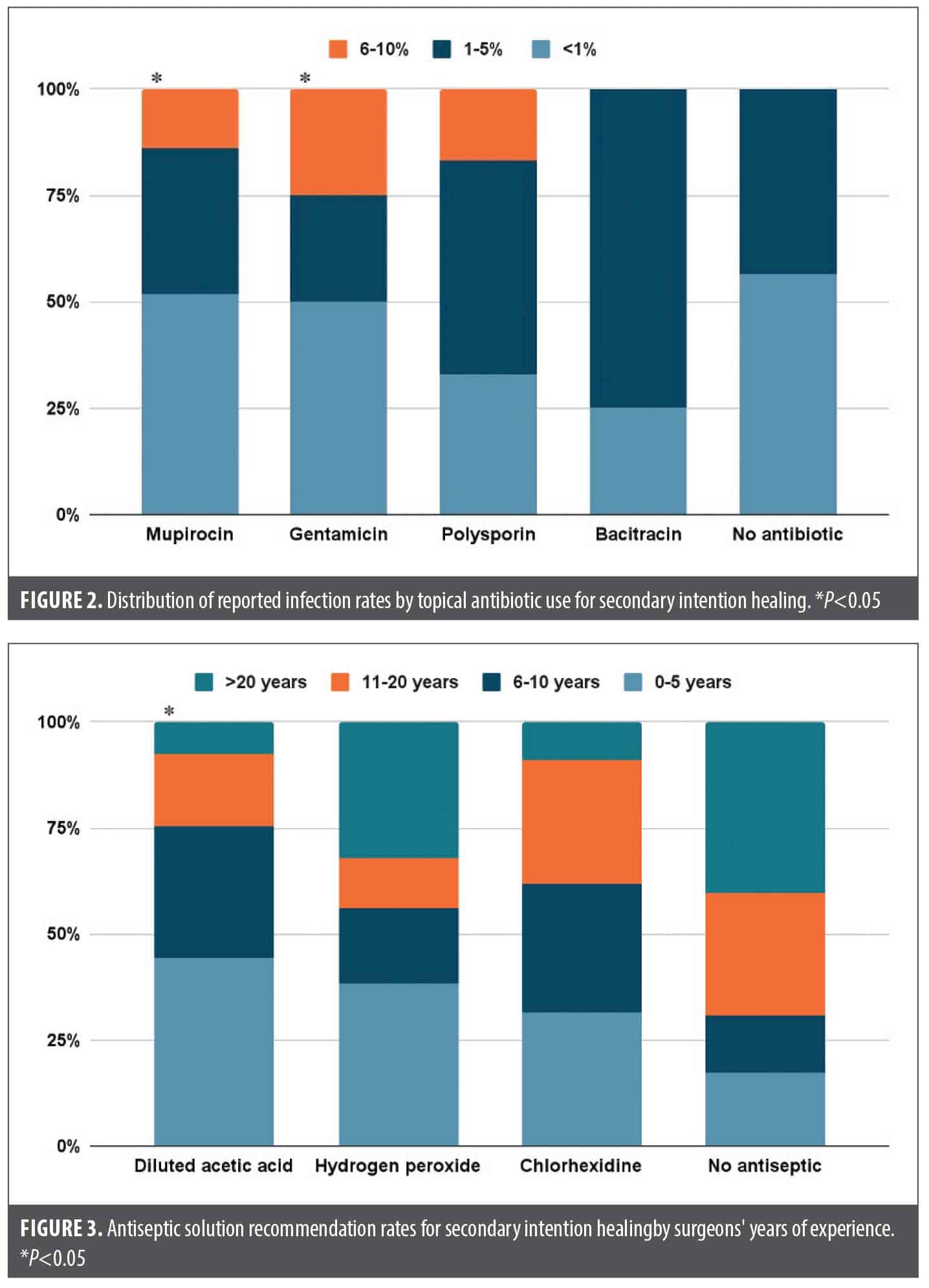
Topical antibiotics. Most respondents (63.9%) did not routinely recommend topical antibiotics for SIH. Among the 36.1% who do recommend antibiotics, mupirocin was most commonly used (34.9%), followed by gentamicin (14.5%), polysporin (7.2%), and bacitracin (4.8%). Eight percent of respondents reported using other topical antibiotics, including silver sulfadiazine and erythromycin. Recommending topical antibiotics was associated with higher reported rates of infection (P=0.034), particularly for mupirocin and gentamicin (Figure 2).
Antiseptic solutions. Most respondents (62.7%) did not recommend using antiseptic solutions, while 37.3% did. Among those who recommended antiseptics, dilute acetic acid was most common (25.3%), followed by chlorhexidine (10.8%) and hydrogen peroxide (9.6%). Other antiseptic solutions (4.8%) reported by respondents included standard soap and hypochlorous acid. Notably, recommendation of antiseptic solutions was lower in respondents with increased years of experience (P=0.016), with only 12.9% of surgeons with over 20 years of experience recommending them vs 38.7% of those with 0 to 5 years of experience (Figure 3).
Other pharmacologic agents. Only 10.8% of respondents recommended use of topical timolol in SIH wound care; of these, 77.8% practice in suburban locations, 55.6% in single specialty group practices, and greater than 50% have been practicing for 0 to 5 years. However, there were no statistically significant associations. Additionally, 6.02% of respondents reported using other pharmacologic agents including cyanoacrylate, VERIS (SweetBio), PuraChol (Medline Industries, Inc.), gentian violet, and oral antibiotics.
Surgical dressing. Most respondents (91.6%) used CND for SIH, while 4.8% preferred HCD. The remaining 4.8% used a combination of both types. Additionally, most respondents (95.2%) advised patients to remove their initial postoperative bandage within 1 to 2 days of surgery. Only a small fraction (4.8%) recommended that patients keep their original bandage on for longer than 2 days.
Outcomes. On average, 72.3% of respondents reported complete healing within 4 to 8 weeks for all wounds undergoing SIH, regardless of location, while 15.7% reported healing in less than 4 weeks and 12% in 9 to 12 weeks. Regarding postoperative infections, 53% of respondents reported rates of less than 1%, 42.2% reported rates of 1% to 5%, and 4.8% reported rates of 6% to 10%. For cosmetic outcomes, 62.7% of respondents reported good results, 32.5% reported excellent results, and 4.8% reported poor results.
Discussion
All respondents reported using topical emollients, with 96.4% preferring petroleum jelly ointments. This preference is likely due to a lower risk of adverse reactions compared to Aquaphor, which has been shown to cause redness in up to 52% of treated wounds.6 This is thought to be due to lanolin, a potential allergen in Aquaphor.5,7 Given the widespread use and established safety profile of petroleum jelly, it continues to serve as the topical emollient of choice for SIH to maintain an optimal healing environment while minimizing the risk of contact dermatitis.
Although the American Academy of Dermatology advises against routine topical antibiotic use, a third of surveyed Mohs surgeons continue to prescribe them. Mupirocin and gentamicin, the most commonly selected antibiotics, were associated with higher reported infection rates (P=0.034). This association may stem from contact dermatitis being misperceived as an infection or from prophylactic use in high-risk patients (eg, those with existing infections, advanced age, obesity, smoking, diabetes, immunosuppression, or ischemia secondary to vascular disease or irradiation).20 In line with these findings, other studies have reported 1.47-fold higher adjusted odds of infection with prophylactic antibiotics.21 These findings, combined with the known risks of bacterial resistance and contact dermatitis, suggest that routine use of topical antibiotics for SIH wounds may be unnecessary and potentially harmful.
Mohs surgeons with 0 to 5 years of surgical experience were more likely to recommend antiseptic solutions in wound care practices compared to surgeons with greater than 20 years of experience (38.7% vs 12.9%). This trend in recommending antiseptic solutions, particularly acetic acid, is noteworthy. Recent studies support the efficacy of acetic acid in wound care, demonstrating its superiority over saline in eliminating Pseudomonas aeruginosa and its antibiofilm activity against common pathogens at low concentrations of 0.5% to 1%.22,23 Therefore, implementation of dilute acetic acid may be a valuable antiseptic technique in SIH wounds, particularly those involving the ear that have a higher risk of P. aeruginosa, or for wounds exhibiting hypergranulation tissue or biofilm concerns.
Despite emerging evidence of its benefits, such as a significant reduction in healing time in chronic lower extremity wounds, only 10.8% of respondents reported using topical timolol in SIH, most of whom were early-career surgeons. The lower adoption rate suggests barriers, including unfamiliarity with off-label use, questionable insurance coverage, safety concerns, and insufficient large-scale trials. Nevertheless, given the potential benefits of topical timolol gel, 0.5%, or solution for wounds on the lower extremities or those exhibiting delayed healing, the low rate of use indicates an area for further exploration.18,19 The reported use of timolol suggests that surgeons are exploring alternative approaches to enhance wound healing.
The predominant use of CND (91.6% of respondents) for SIH wounds contrasts with current literature on postoperative wound care. Recent studies suggest benefits of advanced dressings, particularly HCD, with a meta-analysis finding 72% more ulcers healed with HCD compared to CND.7 HCD have shown faster healing times, superior patient comfort, and convenience after MMS, with 96.8% of patients preferring them.7,8 This discrepancy between practice and literature may be due to familiarity with conventional dressings, cost considerations, or lack of awareness of recent evidence. Further research is needed to better understand the barriers to adopting HCD and to evaluate their impact on outcomes in SIH wound management.
The reported outcomes for SIH in this survey highlight the efficacy of this approach following MMS. Complete healing within 4 to 8 weeks was reported by 72%, similar to a 2017 study by Chetter et al24 who found that the median duration of SIH at the time of their survey was 28.0 days. The rapid healing observed in 15.7% of cases (<4 weeks) suggests that SIH can be remarkably efficient in certain scenarios, potentially rivaling primary closure in select cases.
Perceived infection rates in this study were low, with 53% of surgeons reporting rates less than 1% and 42.2% reporting 1% to 5%. These figures are comparable to primary closure, though the literature shows some variability. A 2020 study found a 6.8% infection rate for SIH wounds vs 3.2% for sutured wounds,25 while a study showed no significant difference in infection rates between SIH and intermediate linear closure.26
This survey reported a 95.2% rate of good to excellent cosmetic outcomes, challenging the perception that SIH results in suboptimal aesthetics. The excellent cosmetic outcomes reported here suggest that SIH can produce highly satisfactory results as reported by Mohs surgeons, particularly in concave surfaces of the face. This high satisfaction rate may potentially reduce the need for complex reconstructions and their associated risks and costs.
Although this study highlights trends in SIH wound care practices and potential associations with outcomes, its low response rate (5.5%) and reliance on self-reported data limit generalizability. The findings should be interpreted as exploratory, with the potential to inform future research rather than guide definitive clinical practice. The inclusion of surgeons from varied practice settings and experience levels adds some breadth, but the lack of standardized outcome definitions and body site stratification further limits interpretation. Future research should prioritize larger prospective studies, randomized controlled trials of specific interventions (eg, topical timolol, antiseptics), and patient-centered outcomes such as quality of life.
Conclusion
Notable variation exists in postoperative care practices for SIH following MMS, despite general alignment with established wound healing principles. Topical antibiotics were associated with higher reported infection rates, while newer approaches—such as antiseptic solutions and topical timolol—remain underutilized. Conventional dressings continue to dominate despite growing evidence supporting HCD. These findings underscore the need for continued research and education to develop evidence-based, standardized guidelines for SIH wound management.
References
- Kim JYS, Kozlow JH, Mittal B, Moyer J, Olencki T, Rodgers P; Work Group; Invited Reviewers. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540–559.
- Kim JYS, Kozlow JH, Mittal B, Moyer J, Olenecki T, Rodgers P; Work Group; Invited Reviewers. Guidelines of care for the management of cutaneous squamous cell carcinoma. J Am Acad Dermatol. 2018;78(3):560–578.
- Zitelli JA. Secondary intention healing: an alternative to surgical repair. Clin Dermatol. 1984;2(3):92–106.
- Norman G, Dumville JC, Mohapatra DP, et al. Antibiotics and antiseptics for surgical wounds healing by secondary intention. Cochrane Database Syst Rev. 2016;3(3):CD011712.
- Nijhawan RI, Smith LA, Mariwalla K. Mohs surgeons’ use of topical emollients in postoperative wound care. Dermatol Surg. 2013;39(8):1260–1263.
- Morales-Burgos A, Loosemore MP, Goldberg LH. Postoperative wound care after dermatologic procedures: a comparison of 2 commonly used petrolatum-based ointments. J Drugs Dermatol. 2013;12(2):163–164.
- Singh A, Halder S, Menon GR, et al. Meta-analysis of randomized controlled trials on hydrocolloid occlusive dressing versus conventional gauze dressing in the healing of chronic wounds. Asian J Surg. 2004;27(4):326–332.
- Holmes SP, Rivera S, Hooper PB, Slaven JE, Que SKT. Hydrocolloid dressing versus conventional wound care after dermatologic surgery. JAAD Int. 2021;6:37–42.
- Smack DP, Harrington AC, Dunn C, et al. Infection and allergy incidence in ambulatory surgery patients using white petrolatum vs bacitracin ointment. A randomized controlled trial. JAMA. 1996;276(12):972–977.
- Dixon AJ, Dixon MP, Dixon JB. Randomized clinical trial of the effect of applying ointment to surgical wounds before occlusive dressing. Br J Surg. 2006;93(8):937–943.
- Mitani O, Nishikawa A, Kurokawa I, Gabazza EC, Ikeda M, Mizutani H. Enhanced wound healing by topical application of ointment containing a low concentration of povidone-iodine. J Wound Care. 2016;25(9):521–529.
- Rai S, Gupta TP, Shaki O, Kale A. Hydrogen peroxide: its use in an extensive acute wound to promote wound granulation and infection control – is it better than normal saline? Int J Low Extrem Wounds. 2021:22(3):563–577.
- Sauvageau AP, Moyer J, Harms KL. Topical hydrogen peroxide promotes secondary intention healing. Dermatol Surg. 2023;49(1):108–110.
- Prodanivic E, Fosko S. Use of vinegar (acetic acid) to promote wound healing complicated by hypergranulation tissue. J Am Acad Dermatol. 2009;60(3 suppl 1):AB203.
- Nour S, Reid G, Sathanantham K, Mackie I. Acetic acid dressings used to treat Pseudomonas colonised burn wounds: a UK national survey. Burns. 2022;48(6):1364–1367.
- Pallotto C, Fiorio M, De Angelis V, et al. Daily bathing with 4% chlorhexidine gluconate in intensive care settings: a randomized controlled trial. Clin Microbiol Infect. 2019;25(6):705–710.
- Dempsey MP, Riopelle AM, West M, Kumar A, Schanbacher CF. The effect of preoperative chlorhexidine gluconate cleanse on lower extremity surgical site infections: a retrospective cohort study. Dermatol Surg. 2024;50(7):627–629.
- Rai AK, Janani K, Rai R. Efficacy of topical timolol versus saline in chronic venous ulcers: a randomized controlled trial. J Cutan Aesthet Surg. 2020;13(1):18–23.
- Manci R, Nazir ZH, Dusza SW, Chen CJ. Topical timolol enhances surgical wound healing in the lower portion of the leg in older patients with comorbidities: a retrospective review. J Am Acad Dermatol. 2022;87(3):661–663.
- Cheadle WG. Risk factors for surgical site infection. Surg Infect (Larchmt). 2006;7(Suppl 1):S7–11.
- Levin EC, Chow C, Makhzoumi Z, Jin C, Shiboski SC, Arron ST. Association of postoperative antibiotics with surgical site infection in Mohs micrographic surgery. Dermatol Surg. 2019;45(1):52–57.
- Madhusudhan VL. Efficacy of 1% acetic acid in the treatment of chronic wounds infected with Pseudomonas aeruginosa: prospective randomised controlled clinical trial. Int Wound J. 2016;13(6):1129–1136.
- Siddiqi A, Abdo ZE, Springer BD, Chen AF. Pursuit of the ideal antiseptic irrigation solution in the management of periprosthetic joint infections. J Bone Jt Infect. 2021;6(6):189–198.
- Chetter IC, Oswald AV, Fletcher M, Dumville JC, Cullum NA. A survey of patients with surgical wounds healing by secondary intention; an assessment of prevalence, aetiology, duration and management. J Tissue Viability. 2017;26(2):103–107.
- Schimmel J, Belcher M, Vieira C, Lawrence N, Decker A. Incidence of surgical site infections in second intention healing after dermatologic surgery. Dermatol Surg. 2020;46(12):1492–1497.
- Schlager JG, Hartmann D, Ruiz San Jose V, Patzer K, French LE, Kendziora B. Procedure-related risk factors for surgical site infection in dermatologic surgery. Dermatol Surg. 2022;48(10):1046–1050.