J Clin Aesthet Dermatol. 2026;19(2):10–14.
by Miguel A. Aristizabal-Torres, MD; Misty M. Hobbs, MD; Thais Pincelli, MD; Olayemi Sokumbi, MD; and
Alison J. Bruce; MB, ChB
Drs. Aristizabal-Torres, Hobbs, Pincelli, Sokumbi, and Bruce are with the Department of Dermatology at Mayo Clinic Florida in Jacksonville, Florida. Dr. Sokumbi is additionally with the Department of Laboratory Medicine & Pathology at Mayo Clinic Florida in Jacksonville, Florida.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors have no conflicts of interest relevant to the contents of this article.
ABSTRACT: Miliary osteoma cutis is an underreported condition that typically presents with firm papules on the face, although involvement of other areas has been described. It commonly presents in middle-aged women with fair skin. Treatment options for this condition are limited. We describe two patients with miliary osteoma cutis, detailing the treatment strategies used, including the successful use of carbon dioxide laser-assisted extraction. Keywords: Osteoma cutis, miliary osteoma cutis, CO2 laser, facial papules
Introduction
In 1858, Wilckens1 first described heterotopic bone formation within the dermis as osteoma cutis. This concept was further refined by Virchow2 in 1864, when he characterized it as multiple miliary lesions affecting various anatomical areas. Multiple miliary osteoma cutis (MMOC) is a rare condition, often underreported or overlooked in the literature. It most commonly presents in middle-aged women with fair skin. Interestingly, it has also been incidentally detected during dental radiologic studies in 2.2% to 27% of diverse population subsets, although conditions with similar radiologic findings, such as calcinosis cutis, could have been included in these studies.3,4
MMOC is classified as primary in 15% to 20% of cases when no underlying cause is identified.5 Secondary MMOC accounts for 80% to 85% of cases and is associated with preexisting conditions, such as acne, connective tissue disease, hereditary disorders, and trauma.6 Unlike other hereditary conditions that present with dystrophic calcification, MMOC has not been associated with any specific genetic mutations.7 Clinically, it commonly presents with asymptomatic papules on the face in women, while men tend to present with lesions involving extrafacial areas such as the neck or trunk.6,8
Lesions of MMOC are typically asymptomatic, often resulting in misdiagnosis and delayed diagnosis. However, patients may express concerns due to the cosmetic implications of lesions. Treatment options for MMOC are limited. In this report, we discuss two cases of MMOC, including the use of a carbon dioxide (CO2) laser-assisted approach as part of the management strategy.
Case reports
Patient 1. A 42-year-old woman presented to the dermatology department with asymptomatic papules on her face for more than 7 years. She had not sought evaluation earlier, attributing these lesions to acne scarring. Her past medical history was notable for recurrent BRCA1-positive breast cancer, with metastasis to the lymph nodes, for which she underwent bilateral mastectomy, axillary lymph node dissection, and chemoradiotherapy. Additionally, she reported a history of severe acne involving the forehead, cheeks, and chin during adolescence and early adulthood, which was effectively treated with spironolactone. After resolution of her acne, she noticed a gradual development of facial papules, which eventually stabilized. Physical examination revealed numerous skin-colored 1 to 3 mm smooth, firm papules on the forehead and cheeks (Figure 1). Her Fitzpatrick skin phototype was determined to be Phototype II. Dermoscopic findings were nonspecific; however, upon close examination, subtle whitish material was visualized in the superficial papules. A 3-mm punch skin biopsy was obtained from her right buccal cheek, demonstrating dense eosinophilic deposits in the superficial-to-mid dermis consistent with mature bone and compatible with osteoma cutis (Figure 2). Laboratory evaluation for secondary causes of MMOC, including serum calcium, phosphorus, parathyroid hormone, vitamin D, alkaline phosphatase, lactate dehydrogenase, creatinine kinase, antinuclear antibody (ANA), extractable nuclear antigen (ENA), and anticentromere antibody, was negative for disorders of calcium metabolism or connective tissue disease.
Prior to biopsy, the patient was treated empirically with oral doxycycline 100 mg twice a day, topical metronidazole cream 0.75%, and azelaic acid gel 15% without improvement. Following biopsy, she completed a 4-month course of tazarotene 0.1% cream nightly with no response. Manual extraction attempts using a sterile #11 blade, following infiltration with 1% lidocaine with 1:100,000 epinephrine, yielded bony fragments. Electrodesiccation was also attempted but proved to be inferior to blade extraction. To reduce the risk of scarring, laser-assisted extraction was performed using a CO2 laser (Candela CO2RE) in continuous mode with a surgical handpiece, a spot size of 1 mm, and a fluence of 10 J. The laser treatment created precise entry points that allowed for manual extraction using an 18-gauge needle or a sterile #11 blade. Lesions were found to be firmly attached to the dermis and underlying subcutaneous tissue (Figure 3 and Figure 4). Several lesions were extracted successfully, with adequate patient tolerability and no evidence of noticeable scarring. The patient reported high satisfaction with the treatment strategy employed (Figure 5).
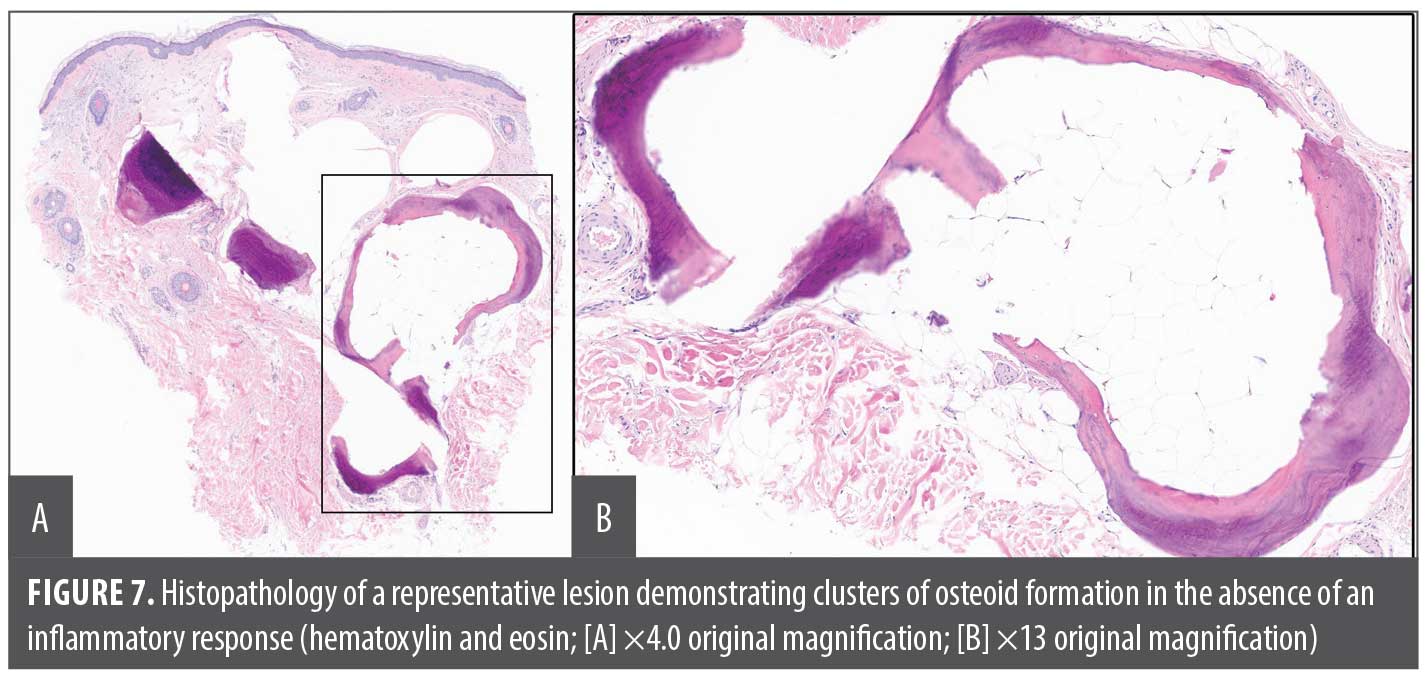
Patient 2. A 65-year-old woman presented to the cosmetic center of our dermatology department with concerns of facial papules that had increased in number for the past 3 years. Her medical history was notable for sarcoidosis, uveitis, and inflammatory arthritis, for which she was receiving treatment with prednisone, methotrexate, and adalimumab. Physical examination revealed scattered skin-colored, smooth, firm, discrete 1mm to 2mm papules involving the bilateral cheeks and chin (Figure 6). Her Fitzpatrick skin phototype was determined to be Phototype IV. Given the clinical morphology of the lesions and the patient’s medical history, cutaneous sarcoidosis was initially considered as the primary differential diagnosis. However, a skin biopsy obtained from the preauricular area revealed osteoma cutis (Figure 7). Laboratory evaluation, including serum calcium, phosphorus, parathyroid hormone, vitamin D, alkaline phosphatase, lactate dehydrogenase, creatinine kinase, ANA, ENA, and anticentromere antibody, was unremarkable. Considering her medical history, skin type, and reported history of poor wound healing and scarring, both laser resurfacing and laser-assisted extraction were deferred. She was started on tazarotene 0.1% cream at bedtime, targeting transepidermal elimination; the assessment of her response to the treatment is forthcoming. The patient continues to be monitored by both the rheumatology and dermatology departments.


Discussion
Due to the increased likelihood of clinical misdiagnosis, the prevalence of MMOC may be underestimated.9,10 This neglected condition not only raises cosmetic concerns for patients but also presents challenges in treatment. One clinical mimicker of MMOC is miliary calcinosis cutis (MCC).11 Distinguishing between the two entities is crucial because both have been regarded as secondary to other clinical conditions, such as systemic sclerosis and dermatomyositis for MMOC, and renal failure and myeloma for MCC, among others.12 On histopathology, MCC presents with calcium salt deposits localized in the dermal-subcutaneous tissue junction in MCC, while MMOC is characterized by bone fragments in the mid-dermis.12
The etiology of MMOC has been attributed to intramembranous ossification occurring in specific areas within the dermis.13,14 In the literature, it is often described as a presumptive metaplastic response to preexisting conditions, typically of an inflammatory nature. This process involves the activation of resident mesenchymal multipotent cells, which are influenced by bone-related cytokines, leading them to follow an osteoblast-like pathway.15 Recognizing the female preponderance of MMOC, estrogens have been implicated in disease pathogenesis.7 However, controversy exists, as cases in men and postmenopausal women have also been reported.16 Recently, Cutibacterium acnes deoxyribonucleic acid (DNA) has been identified within MMOC lesions, raising concerns for a possible pathogenic association.17
Clinically, MMOC is characterized by 0.5- to 3-mm papules, most commonly manifesting on the face.18,19 These papules may exhibit a whitish hue, though pigmented variants have also been described.20 Diagnostic confirmation is achieved through histopathologic examination, which demonstrates bone spicules of different dimensions located within the dermis or subcutaneous tissue.21,22 These bone formations contain numerous osteocytes and are marked by cement lines, which may appear more prominent under polarized light. Moreover, osteoblasts are commonly observed along the surface of the spicules, with osteoclasts often found in Howship’s lacunae.23 In cases where additional clinical findings suggest hereditary conditions or other secondary causes, serum calcium and parathyroid hormone levels can aid in excluding such conditions.6,24 Additional imaging studies can also be employed to assess the extent of the disease.25
Treatment options for MMOC are limited. Initially, bisphosphonates were employed with the goal of reducing bone remodeling, with poor success.26 Topical retinoids are an adequate initial therapy, especially for superficial lesions or those with a diameter of 1 mm or less.27,28 However, escalation of therapy is often necessary, for example, using dermabrasion with punch biopsy,29 scalpel incisions and curettage,30 or needle-assisted extraction.9,31,32 Erbium:yttriumaluminum-garnet (YAG) laser,33 Nd:YAG laser,8 and CO2 laser34 have also been described as treatment alternatives.
Our previous experience performing CO2 laser-assisted extraction in the treatment of MCC inspired us to adopt a similar strategy for MMOC.35 Both conditions required manual extraction; however, MMOC lesions were morphologically different, exhibiting a lobulated aspect and a notably firmer attachment to the dermis than MCC. Postlaser care is crucial to minimize the risks of scarring and pigmentary changes. While laser-assisted extraction may offer beneficial results, clinicians should remain cautious of the potential risks associated with any laser-assisted or extraction technique.
Conclusion
MMOC is an often underrecognized condition that requires histopathologic confirmation with implications for diagnosis and treatment. Our case reports underscore the importance of considering MMOC in patients presenting with firm, asymptomatic facial papules. MMOC can significantly impact quality of life due to cosmetic concerns. Treatment options are limited and often involve manual extraction, which can be laser-assisted. Clinicians should remain vigilant for potential complications associated with treatment.
References
- Wilckens M. Ueber die Verknocherung und Verkalkung der Haut. Inaug Dissert, Göttingen. Kaestner, 1858, p. 6.
- Virchow R. Die krankhaften Geschwülste. A. Hirschwald; 1863-1867.
- Shigehara H, Honda Y, Kishi K, Sugimoto T. Radiographic and morphologic studies of multiple miliary osteomas of cadaver skin. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86(1):121-125.
- Kishi K, Kawahara K, Moriya I, Komatsu H, Sato M, Aono K. Clinical and radiographic study of multiple miliary osteomas of the skin. Dentomaxillofac Radiol. 1984;13(2):105-108.
- Duarte IGL. Multiple injuries of osteoma skin in the face: therapeutical least invasive in patients with acne sequela – case report. An Bras Dermatol. 2010;85(5):695-698.
- Duarte BM, Pinheiro RR, Cabete J. Multiple miliary osteoma cutis: a comprehensive review and update of the literature. Eur J Dermatol. 2018;28(4):434-439.
- Myllylä RM, Haapasaari KM, Palatsi R, et al. Multiple miliary osteoma cutis is a distinct disease entity: four case reports and review of the literature. Br J Dermatol. 2011;164(3):544-552.
- Barolet AC, Litvinov IV, Barolet D. Multiple miliary osteoma cutis treatment response to Q-switched Nd:YAG laser: a case report. SAGE Open Med Case Rep. 2020;8:2050313X20910562
- Thielen AM, Stucki L, Braun RP, et al. Multiple cutaneous osteomas of the face associated with chronic inflammatory acne. J Eur Acad Dermatol Venereol. 2006;20(3):321-326.
- Kim D, Franco GA, Shigehara H, Asaumi J, Hildenbrand P. Benign miliary osteoma cutis of the face: a common incidental CT finding. AJNR Am J Neuroradiol. 2017;38(4):789-794.
- Chabra IS, Obagi S. Evaluation and management of multiple miliary osteoma cutis: case series of 11 patients and literature review. Dermatol Surg. 2014;40(1):66-68.
- Niebel D, Poortinga S, Wenzel J. Osteoma cutis and calcinosis cutis: “similar but different”.
J Clin Aesthet Dermatol. 2020;13(11):28-31. - Oikarinen A, Tuomi ML, Kallionen M, Sandberg M, Väänänen K. A study of bone formation in osteoma cutis employing biochemical, histochemical and in situ hybridization techniques. Acta Derm Venereol. 1992;72(3):172-174.
- Basler RS, Taylor WB, Peacor DR. Postacne osteoma cutis. X-ray diffraction analysis. Arch Dermatol. 1974;110(1):113-114.
- Elli FM, Boldrin V, Pirelli A, Spada A, Mantovani G. The complex GNAS imprinted locus and mesenchymal stem cells differentiation. Horm Metab Res. 2017;49(4):250-258.
- Conlin PA, Jimenez-Quintero LP, Rapini RP. Osteomas of the skin revisited: a clinicopathologic review of 74 cases. Am J Dermatopathol. 2002;24(6):479-483.
- Kondo M, Yamanaka K. Detection of Cutibacterium acnes from multiple miliary osteoma cutis. Clin Case Rep. 2022;10(10):e6492.
- Mosquera H, Reyes E, Medina CL. Osteoma cutis miliar múltiple de la cara, reporte de un caso. Rev Asoc Colomb Dermatol. 2019;22(3):243-245.
- Bouraoui S, Mlika M, Kort R, Cherif F, Lahmar A, Sabeh M. Miliary osteoma cutis of the face.
J Dermatol Case Rep. 2011;5(4):77-81. - Moritz D, Elewski B. Pigmented postacne osteoma cutis in a patient treated with minocycline: report and review of the literature. J Am Acad Dermatol. 1991;24
(5 Pt 2):851-853. - Ma HJ, Jia CY, Yang Y, Song LJ, Hu R, Li TH. Primary multiple miliary osteoma cutis: an unusual Chinese case. Int J Dermatol. 2014;53(1):73-75.
- Delaleu J, Cordoliani F, Bagot M, Bouaziz JD, Vignon-Pennamen MD, Lepelletier C. Miliary osteoma cutis of the face. Article in French. Ann Dermatol Venereol. 2020;147(4):313-315.
- Camozzato C, Basso Fde O, Duquia RP, Boff AL, de Almeida HL Jr. Facial miliary osteoma in HIV patient. An Bras Dermatol. 2011;86(4 Suppl 1):S66-S68.
- Ward S, Sugo E, Verge C, Wargon O. Three cases of osteoma cutis occurring in infancy. A brief overview of osteoma cutis and its association with pseudo-pseudohypoparathyroidism. Australas J Dermatol. 2011;52(2):127-131.
- Alhazmi D, Badr F, Jadu F, Jan AM, Abdulsalam Z. Osteoma cutis of the face in CBCT images. Case Rep Dent. 2017;2017:8468965.
- Goldminz D, Greenberg R. Multiple miliary osteoma cutis. J Am Acad Dermatol. 1991;24(5 Pt 2):878-881.
- Smith CG, Glaser DA. Treatment of multiple miliary osteoma cutis with tretinoin gel. J Am Acad Dermatol. 1999;41(3 Pt 1):500.
- Cohen AD, Chetov T, Cagnano E, Naimer S, Vardy DA. Treatment of multiple miliary osteoma cutis of the face with local application of tretinoin (all-trans-retinoic acid): a case report and review of the literature. J Dermatolog Treat. 2001;12(3):171-173.
- Fulton JE Jr. Dermabrasion-Loo-punch-excision technique for the treatment of acne-induced osteoma cutis. J Dermatol Surg Oncol. 1987;13(6):655-659.
- Altman J, Nehal K, Busam K, Halpern AC. Treatment of primary miliary osteoma cutis with incision, curettage, and primary closure.
J Am Acad Dermatol. 2001;44(1):96-99. - Duarte B, Pinheiro RR, Cabete J. Multiple miliary osteoma cutis: an overlooked dermatosis? J Eur Acad Dermatol Venereol. 2018;32(1):e20-e22.
- Baskan E, Turan H, Tunali S, Toker SC, Adim SB, Bolca N. Miliary osteoma cutis of the face: Treatment with the needle microincision‐extirpation method. J Dermatolog Treat. 2007;18(4):252-254.
- Ochsendorf FR, Kaufmann R. Erbium:YAG laser ablation of osteoma cutis: modifications of the approach. Arch Dermatol. 1999;135(11):1416.
- Kim SY, Park SB, Lee Y, et al. Multiple miliary osteoma cutis: treatment with CO2 laser and hook. J Cosmet Laser Ther. 2011;13(5):227-230.
- Aristizabal M, Aristizabal J, Giraldo D, Loboguerrero O, Gold MH. Milia‐like idiopathic calcinosis cutis of the forehead in an adult without Down’s syndrome successfully treated with a CO2 laser. J Cosmet Dermatol. 2020;19(1):102-104.