J Clin Aesthet Dermatol. 2019;12(12):35–38

by Priyanka Sharma, MD; Anand Kumar, MD; Ankita Tuknayat, MBBS; Gurvinder P. Thami, MD; and Ritu Kundu, MD
Drs. Sharma, Kumar, and Thami are with the Department of Dermatology at the Government Medical College and Hospital in Chandigarh, India. Dr. Tuknayat is with the Government Medical College and Hospital in Chandigarh, India. Dr. Kundu is with the Department of Pathology at the Government Medical College and Hospital in Chandigarh, India.
FUNDING: No funding was provided for this study.
DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: Lucio phenomenon (LP) is a rare reactional state seen in cases of diffuse lepromatous leprosy. Lucio leprosy is a pure, primitive, and diffuse form of lepromatous leprosy. It is observed almost exclusively in Mexico and Central America and is considered a globally restricted phenomenon. However, isolated cases are being reported worldwide. Patients with Lucio leprosy often present with manifestations of LP, which includes purpuric macules with multiple and extensive areas of ulceration with bizarre-patterned, angulated borders mainly affecting the extremities. LP is difficult to recognize, especially in nonendemic countries, which can lead to a delay in its diagnosis and management. We report a case of LP due to its occurrence in the classical form of lepromatous leprosy and rarity in North India.
KEYWORDS: Lepromatous leprosy, Lucio phenomenon, purpuric macules
Hansen’s disease, or leprosy, a chronic infection caused by Mycobacterium leprae, is an old and widespread disease with a higher incidence in developing countries.1 It runs a chronic indolent course that can become complicated by acute, immune-mediated phenomena called lepra reactions.2 Lucio phenomenon is one such rare reactional state seen peculiarly in the pure and primitive diffuse form of lepromatous leprosy and less commonly in borderline forms.3,4 This phenomenon was first described by Lucio and Alvarado5 in Mexico in 1852 and further elaborated by Latapi and Zamora6 in 1948 after the identification of histopathological changes involving multiple acute, necrotizing cutaneous vasculitis. It was considered a globally restricted phenomenon endemic to Mexico and Central America until sporadic cases were reported from nonendemic areas of the world, including the United States, Spain, Cuba, and countries in Southeast Asia, the Middle East, South America, and the South Pacific.7–12 It is clinically characterized by severe necrotizing cutaneous lesions, mainly on the extremities.12 Here, we present a rare case of a man with Lucio phenomenon in a previously undiagnosed case of lepromatous leprosy in India.
Case Presentation
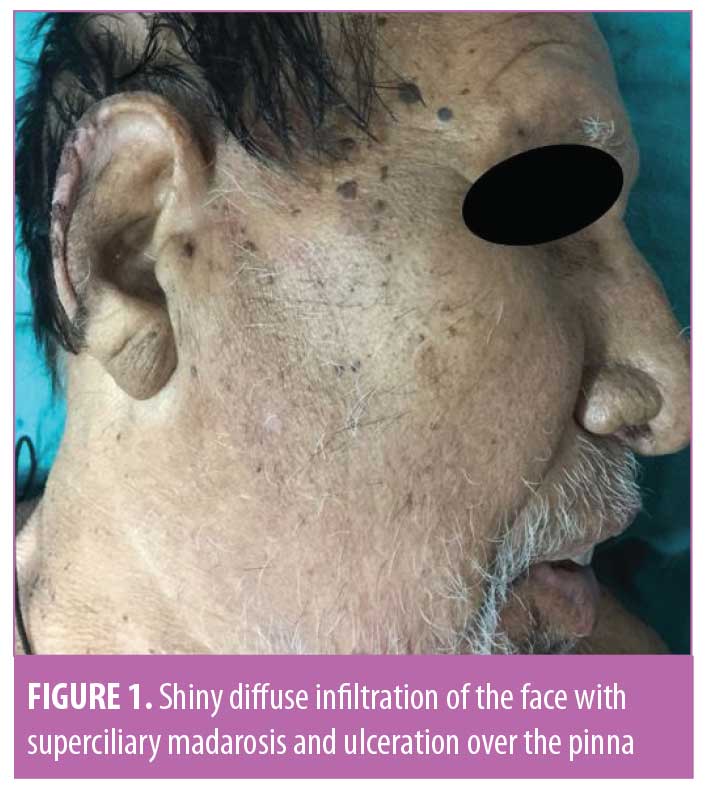
A 71-year-old man presented with extensive cutaneous ulcerations over the upper and lower extremities that appeared two weeks prior. The lesions first appeared as purpuric macules over the legs, followed by the buttocks, arms, trunk, and ears. After a week, the lesions gradually became coalesced in geographic patterns and developed a dusky erythematic appearance with subsequent ulceration. The patient had a history of recurrent swelling of the legs, decreased tactile sensations over the hands and feet, and recurrent episodes of epistaxis for last few years. He had not sought medical intervention in the past for his illness. On examination, the treatment team observed diffuse infiltration of the patient’s face, ear lobules, and back, with ciliary and supraciliary madarosis and a shiny appearance of the face (Figure 1). There were extensive deep, bizarrely shaped, punched out ulcers with polycyclic margins, predominantly over the legs and buttocks, with yellowish necrotic slough and an overlying blackish adherent crust. Ulcers were surrounded by a zone of bright red infiltrated skin (Figure 2a). There were also irregularly shaped, dusky red, purpuric macules over the dorsum of the hands and extensor aspects of the forearms (Figure 2b). Further, there was bilaterally symmetrical thickening of the ulnar, radial, lateral popliteal, posterior tibial, and great auricular nerves without associated tenderness. Bilateral glove and stocking anesthesia was also present. Cranial nerve examination was normal. There was no motor weakness present in the limbs. Slit skin smear examination from the earlobes and eyebrows revealed a morphological index (percentage of solid stained bacilli calculated after examining 200 red-staining elements lying singly) of 80 percent and bacteriological index (density of the both live and dead bacilli in the smears) of 5+. Histopathological examination revealed foamy macrophages (Figure 3a), dermal vessels showing ischemic necrotizing vasculitis endarteritis obliterans due to endothelial proliferation (Figure 3b), and clumps of acid-fast bacilli (AFB) periadnexally, perivascularly, and within the macrophages and endothelial cells. Complete blood count revealed hemoglobin 7.6g/dL, erythrocyte sedimentation rate (Westergren method) of 28mm in the first hour, and reticulocyte count of 14 percent. Coagulation profile, liver function tests, renal function tests, urinalysis, blood sugar, antinuclear factor, rheumatoid factor, sputum for AFB, Mantoux test and chest X-ray were normal. Serology for human immunodeficiency virus, syphilis, and hepatitis B surface antigen was negative. Tissue smears and cultures for fungus, bacteria, Mycobacterium tuberculosis, and atypical mycobacteria were negative.



Based on clinicohistopathological findings a diagnosis of lepromatous leprosy (Ridley–Jopling) with Lucio phenomenon was made. The patient was started on a World Health Organization multibacillary multidrug therapy (MB-MDT) regimen—rifampicin 600mg once a month, dapsone 100mg daily, and clofazimine 300mg once a month and 100mg daily. In addition, prednisolone 1mg/kg per day was also started. After two weeks of treatment, the ulcers started healing with central achromic scars and surrounding hypepigmented borders (Figure 4).

Discussion
Vasculonecrotic reactions in leprosy includes Lucio phenomenon and vasculonecrotic erythema nodosum leprosum.13 Lucio phenomenon is usually associated with an untreated or inadequately treated, well-established, diffuse, nonnodular form of leprosy known as Lucio leprosy but also called lepra bonita, which is Spanish for “pretty leprosy,” due to the shiny myxedoematoid appearance of the skin seen in this form.14,15 However, its occurrence is not exclusive to Lucio leprosy, as it has been reported in the classic nodular form of lepromatous and borderline leprosy.4 Lucio phenomenon usually begins as painful purpuric lesions that evolve into well defined, multiangulated, jagged ulcerations with a geometric shape involving—in descending order of frequency—the feet, legs, hands, forearms, thighs, arms, and rarely, the trunk and face. Ulcers heal in about 2 to 8 weeks, leaving curvilinear jagged atrophic hypochromic scars with a surrounding halo of hyperpigmentation. There is an absence of associated fever, constitutional symptoms, and systemic involvement and neuritis.16 The exact etiopathogenesis of Lucio phenomenon is unclear. The most accepted hypothesis is uninhibited multiplication of lepra bacilli leading to diffuse infiltration of the integument in an anergic background and enhanced exposure of mycobacterial antigen to circulating antibodies, resulting in vasculitis.17 Latapi and Zamora6 considered it to be a hypersensitivity response due to high antigenic load because of synergism between M. leprae and cocci causing superadded infections. Recently, a new organism, Mycobacterium lepromatosis, has been isolated from some of these patients but more evidence is required to establish its causative role.18 Furthermore, vascular and perivascular deposits of immunoglobulins and complement have been demonstrated in lesions of Lucio phenomenon, suggesting a possible role of immune complex in its pathogenesis.19 Lucio phenomenon characteristically shows highly positive bacteriological and morphological indices. Histological features are colonization of the endothelial cells by acid-fast bacilli; endothelial proliferation of the medium-sized vessels of the mid-dermis with passive venous congestion; and neutrophilic infiltration, ischemic epidermal necrosis, and necrotizing vasculitis of the small vessels of the superficial dermis.20 Differential diagnoses include vasculonecrotic erythema nodosum, systemic vasculitis, disseminated intravascular coagulation, cutaneous tuberculosis, deep mycoses, and tertiary syphilis. Lucio phenomenon might be confused with vasculonecrotic erythema nodosum leprosum, which presents as painful necrotic ulcers with constitutional symptoms, neuritis, and sometimes visceral involvement.4 However, the distinctive clinical and histopathological features may aid in differentiating the two (Table 1). Treatment of Lucio phenomenon includes multibacillary multidrug therapy for leprosy, which includes rifampicin, dapsone and clofazimine for 12 months. A short course of high-dose corticosteroids (1mg/kg/day) can be effective in controlling the immune reaction in the initial phase, especially in severe cases.13 Since Lucio leprosy is often unmasked by Lucio phenomenon, a high index of suspicion is very important for early diagnosis, and prompt treatment can improve the disease outcome in areas nonendemic for Lucio leprosy.
References
- Lastória JC, Abreu MAMM de. Leprosy: review of the epidemiological, clinical, and etiopathogenic aspects—part 1. An Bras Dermatol. 2014;89(2):205–218.
- Scollard DM, Smith T, Bhoopat L, et al. Epidemiologic characteristics of leprosy reactions. Int J Lepr Mycobact Dis Off Organ Int Lepr Assoc. 1994;62(4):559–567.
- Donner RS, Shively JA. The “Lucio phenomenon” in diffuse leprosy. Ann Intern Med. 1967;67(4): 831–836.
- Chandrashekar L, Kumari R, Thappa D, et al. Is it Lucio phenomenon or necrotic erythema nodosum leprosum? Indian J Dermatol. 2013;58(2):160.
- Lucio R, Alvarado I. Opusculo Sobre el Mal de San Lazaro o Elefanciasis de los Greigos. México:M. Murguía; 1852.
- Latapi F, Chevez Zamoro A. The ‘spotted’ leprosy of Lucio. An introduction to its clinical and histological study. Int J Leprosy. 1948;16:421–430.
- Moschella SL. The lepra reaction with necrotizing skin lesions. A report of six cases. Arch Dermatol. 1967;95(6):565–575.
- Herath S, Navinan MR, Liyanage I, et al. Lucio’s phenomenon, an uncommon occurrence among leprosy patients in Sri Lanka. BMC Res Notes. 2015;8:672.
- Rocha RH, Emerich PS, Diniz LM, et al. Lucio’s phenomenon: exuberant case report and review of Brazilian cases. An Bras Dermatol. 2016;91(5 Suppl 1):60–63.
- Choon SE, Tey KE. Lucio’s phenomenon: a report of three cases seen in Johor, Malaysia. Int J Dermatol. 2009;48(9):984–988.
- Kaur C, Thami GP, Mohan H. Lucio phenomenon and Lucio leprosy. Clin Exp Dermatol. 2005;30(5):525–527.
- Strobel M, Ndiaye B, Carayon A. [Lepromatous leprosy with extensive ulcerations and cachexia. The Lucio phenomenon? Lazarine leprosy?]. Acta Leprol. 1979;(76-77):331–333. Article in French.
- Fogagnolo L, de Souza EM, Cintra ML, Velho PENF. Vasculonecrotic reactions in leprosy. Braz J Infect Dis Off Publ Braz Soc Infect Dis. 2007;11(3): 378–382.
- Costa IMC, Kawano LB, Pereira CP, Nogueira LSC. Lucio’s phenomenon: a case report and review of the literature. Int J Dermatol. 2005;44(7):566–571.
- Prem Anand P, Oommen N, Sunil S, Deepa MS, Potturu M. Pretty leprosy: another face of Hansen’s disease! A review. Egypt J Chest Dis Tuberc. 2014;63(4):1087–1090.
- Sehgal VN. Lucio’s phenomenon/erythema necroticans. Int J Dermatol. 2005;44(7):602–605.
- Sehgal VN, Srivastava G, Sharma VK. Contemplative immune mechanism of Lucio phenomenon and its global status. J Dermatol. 1987;14(6):580–585.
- Alvarado-Villa G, Vera-Cabrera L, Velarde-Felix JS. “Lucio’s phenomenon” associated with Mycobacterium lepromatosis. Am J Trop Med Hyg. 2016;94(3):483–484.
- Quismorio FP, Rea T, Chandor S, et al. Lucio’s phenomenon: an immune complex deposition syndrome in lepromatous leprosy. Clin Immunol Immunopathol. 1978;9(2):184–193.
- Vargas-Ocampo F. Diffuse leprosy of Lucio and Latapí: a histologic study. Lepr Rev. 2007;78(3):248–260.