
J Clin Aesthet Dermatol. 2021;14(2):22–24.
by Rym Afiouni, MD; Josiane Helou, MD; Stephanie Matar, MD; and Roland Tomb, MD, PhD
All authors are with the Department of Dermatology, Hôtel-Dieu de France University Hospital, Saint Joseph University in Beirut, Lebanon.
FUNDING: No funding was provided for this article.
DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
ABSTRACT: Rosacea and cutaneous lupus erythematosus (CLE) are chronic inflammatory dermatoses. To our knowledge, no cases of granulomatous rosacea (GR) associated with CLE have been previously reported in the literature. We describe the case of a 38-year-old female patient who presented to our clinic with a diffuse scaly facial erythema, with the co-diagnoses of GR and CLE later confirmed with clinicopathological correlation.
KEYWORDS: Rosacea, granuloma, lupus erythematosus, Demodex
Both rosacea and cutaneous lupus erythematosus (CLE) are chronic inflammatory dermatoses that can present clinically with facial erythema and papules. To our knowledge, no cases of granulomatous rosacea (GR) associated with CLE have been previously described. Here, we describe the case of a 38-year-old female patient who presented to our clinic with a diffuse scaly facial erythema, with the co-diagnoses of GR and CLE later confirmed with clinicopathological correlation.
Case Presentation
A 38-year-old female patient presented to our dermatology department with persistent facial erythema persisting for two months prior to visiting our clinic. Upon examination, she had erythema, thick scales, and pustules on the entire face, particularly on her glabella, nose, and around the mouth (Figure 1). She had been already treated with doxycycline and topical and oral metronidazole, with little change. The patient noted exacerbation with sun exposure and heat. The patient had no significant personal or family history and had no lesions elsewhere on her body. She reported no systemic symptoms. Our differential diagnosis included CLE, rosacea, and severe seborrheic dermatitis.

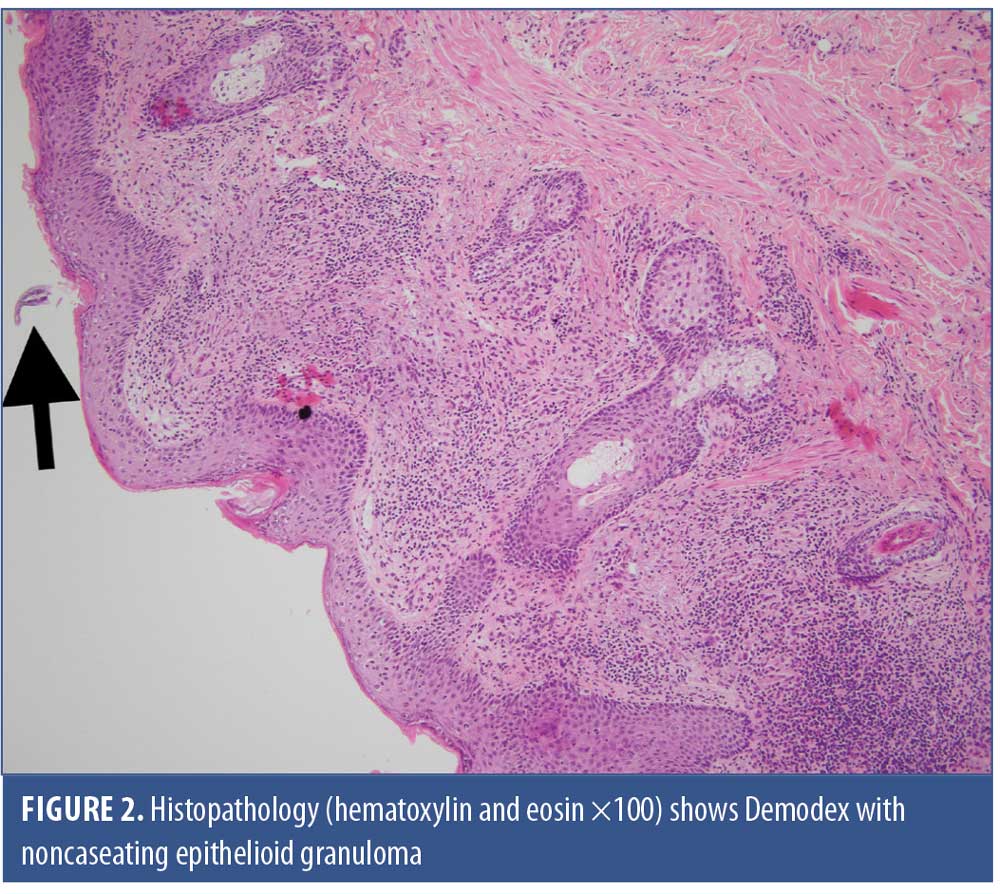
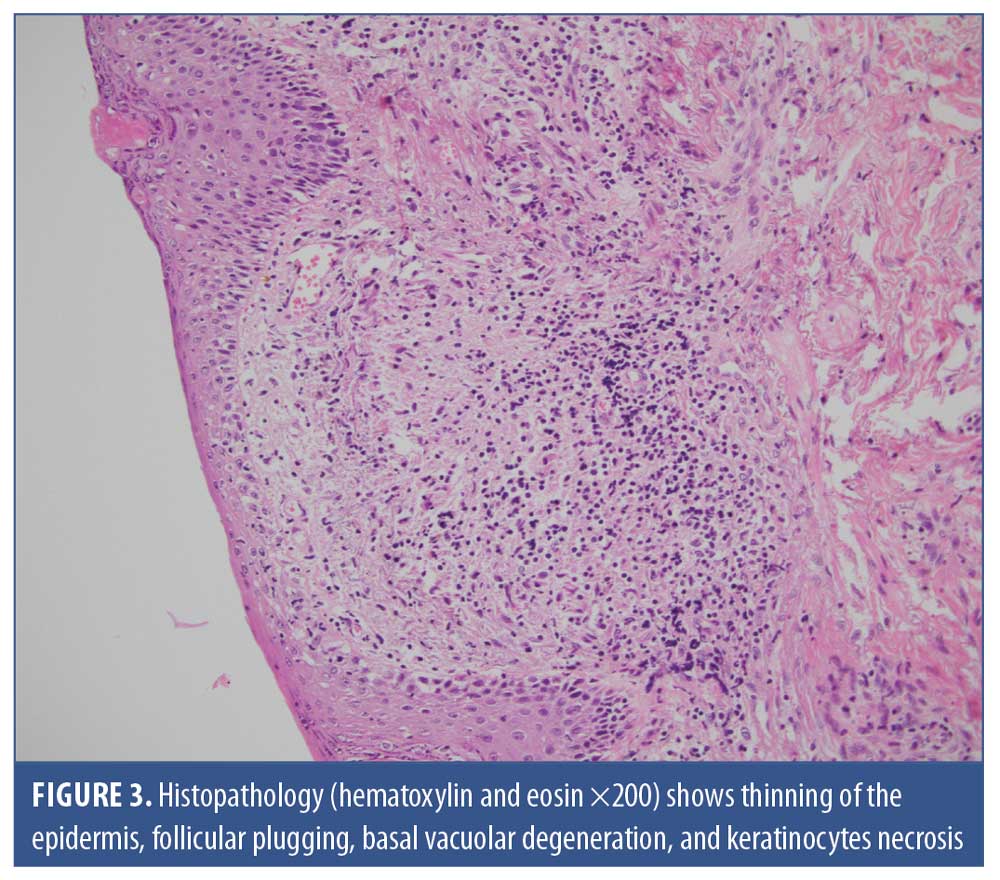
The patient received 200mg of itraconazole twice daily, with a biopsy scheduled for one week later; however, no improvement was observed with the itraconazole. The skin biopsy revealed orthokeratosis with follicular plugging, the presence of Demodex on the surface, thinning of the epidermis, keratinocytes necrosis, basal vacuolar degeneration, and thickening of the basement membrane on periodic acid-Schiff staining. In addition, an inflammatory infiltrate in the superficial dermis, noncaseating epithelioid granulomas (i.e., lymphocytes, histiocytes, giant cells), with sometimes free Demodex and pigmentary incontinence in an elastotic dermis (Figures 2 and 3) were observed. Further, direct immunofluorescence (DIF) was positive, with granular immunoglobulin G, immunoglobulin M, and C3 deposits noted along the basement membrane and surrounding the follicles. Overall, the patient’s presentation was compatible with the diagnosis of CLE associated with GR.
Blood tests confirmed a normal complete blood count (CBC), normal erythrocyte sedimentation rate (ESR), normal renal and liver panels, and normal complement components, with positive anti-nuclear antibodies (ANA 1/320) but negative anti-dsDNA, anti-Smith, anti-SSa, and anti-SSb antibodies. Based on this profile, systemic disease was ruled out.
Hydroxychloroquine (200mg twice daily) together with topical metronidazole was initiated. The patient showed improvement two months after the start of treatment, but continued to experience persistent flushing, erythema, and moderate scaling. Isotretinoin (20mg daily) was then added and the hydroxychloroquine was continued twice daily for three months. With further follow-up, the patient appeared to sustain improvement, with total clearance of the erythema and the scales (Figure 4). Follow-up lab tests showed normal CBC, normal ESR, negative ANA and anti-dsDNA, normal complement components, and normal hepatic and renal panels.

Discussion
Clinicians may sometimes face the diagnostic challenge of differentiating rosacea and CLE, given that both can present clinically with facial erythema and papules than can be triggered by sun exposure and histologically with perifollicular and perivascular lymphocytic infiltrate.1
GR is a rare chronic inflammatory dermatosis considered to be a variant of rosacea.2 Demodex folliculorum is an obligatory parasite of the hair follicles that may play a role in the pathogenesis of rosacea as well as the severity of the condition and its level of resistance to treatment.3,4 GR can also be associated with the presence of Demodex folliculorum,2 which is clinically characterized by erythematous papules and nodules on the face—especially around the eyes, nose, and mouth—that are usually exacerbated after consuming hot drinks or alcohol, exposure to heat, and steroid use.2,5 On histopathology, GR presents with noncaseating epithelioid granulomas in the superficial and mid-dermis.6 GR can mimic some facial granulomatous conditions on clinical and histological presentation, including cutaneous tuberculosis, lupus miliaria disseminatus faciei, and sarcoidosis.6 Our patient presented with centrofacial erythematous papules and pustules together with granulomas and Demodex on histopathology, in favor of the diagnosis of GR.
CLE is an autoimmune disease stratified as acute, subacute, and chronic CLE.7 Chronic CLE most commonly presents as discoid lupus erythematosus (DLE).7 Clinically, DLE starts with erythematosquamous macules or papules, then grows into plaques that can leave atrophic and pigmented scars.8 Rare variants of CLE, such as comedonal CLE, have been described in the literature.9 Skin lesions in CLE could be induced or exacerbated by sun exposure.10
Investigation with laboratory tests, including CBC, renal and hepatic panels, and ANA is recommended to exclude systemic disease.9 Furthermore, cutaneous biopsy is needed to confirm the diagnosis of CLE. Typical features include interface dermatitis, basal layer degeneration, perivascular and perifollicular infiltrates, hyperkeratosis, abundant mucin, and thinning of the epidermis.11 DIF of lesional skin may be required in equivocal cases, showing immunoglobulin (often immunoglobulin G) and complement components (often C3) deposits at the dermal–epidermal junction.12 Our patient presented with erythematous scaly plaques on the face exacerbated by sun exposure, with confirmed CLE on hematoxylin and eosin and DIF. Her lack of scarring is probably due to the early start of treatment.8
On histopathology, necrotic keratinocytes with lymphocytes, basal vacuolar degeneration, colloid bodies, and pigmentary incontinence must be looked for to confirm an interface process. In addition, follicular plugging is a marker for CLE.1 On the other hand, the presence of Demodex strongly favors rosacea.1,4 Therefore, in our case, histopathology confirmed the presence of both CLE and GR, which, to our knowledge, has never been described in the literature and could be considered as an overlap. More cases and eventually more studies are needed to evaluate the relationship and association between these two entities.
Treatment of GR usually consists of oral antibiotics (doxycycline or tetracycline), usually with a good response; oral isotretinoin is reserved for recalcitrant disease.2,13 Other therapies include topical metronidazole, azelaic acid, and benzoyl peroxide.5 In addition, antiparasitic treatment with topical 1% ivermectin for 30 days is highly efficacious in the case of rosacea associated with Demodex and is comparable to combined treatment by oral metronidazole (250mg twice daily) and topical 1% metronidazole once daily for 30 days.3 Demodex in addition to CLE could have contributed to the degree of treatment resistance to prior treatment with doxycycline observed in our patient.
Management of CLE depends on the presence of systemic disease. Our patient had cutaneous manifestations with no evidence of systemic disease. Photoprotection and smoking cessation are indicated for all patients with CLE.14 Topical corticosteroids are considered first-line for mild disease, while topical calcineurin inhibitors can also be used for steroid-sparing purposes.15 Hydroxychloroquine is considered appropriate for mild disease resistant to topical treatment or for mild-to-moderate disease.15 Limited studies suggest a favorable response to retinoids, including isotretinoin.15 Therefore, isotretinoin could have had an effect on both GR and CLE in our patient.
References
- Brown TT, Choi E-YK, Thomas DG, et al. Comparative analysis of rosacea and cutaneous lupus erythematosus: histopathologic features, T-cell subsets, and plasmacytoid dendritic cells. J Am Acad Dermatol. 2014;71(1):100–107.
- Chougule A, Chatterjee D, Yadav R, et al. Granulomatous rosacea versus lupus miliaris disseminatus faciei—2 faces of facial granulomatous disorder: a clinicohistological and molecular study. Am J Dermatopathol. 2018 Nov;40(11):819–823.
- Kubanov A, Gallyamova Y, Kravchenko A. Clinical picture, diagnosis and treatment of rosacea, complicated by Demodex mites. Dermatol Rep. 2019;11(1):7675.
- Chang Y-S, Huang Y-C. Role of Demodex mite infestation in rosacea: A systematic review and meta-analysis. J Am Acad Dermatol. 2017;77(3):441–447.e6.
- Lee GL, Zirwas MJ. Granulomatous rosacea and periorificial dermatitis: controversies and review of management and treatment. Dermatol Clin. 2015;33(3):447–455.
- Batra M, Bansal C, Tulsyan S. Granulomatous rosacea: unusual presentation as solitary plaque. Dermatol Online J. 2011;17(2):9.
- Walling HW, Sontheimer RD. Cutaneous lupus erythematosus: issues in diagnosis and treatment. Am J Clin Dermatol. 2009;10(6):365–381.
- Grönhagen CM, Nyberg F. Cutaneous lupus erythematosus: an update. Indian Dermatol Online J. 2014;5(1):7–13.
- Vieira ML, Marques ERMC, Leda YLA, et al. Chronic cutaneous lupus erythematosus presenting as atypical acneiform and comedonal plaque: case report and literature review. Lupus. 2018;27(5):853–857.
- Biazar C, Sigges J, Patsinakidis N, et al. Cutaneous lupus erythematosus: first multicenter database analysis of 1002 patients from the European Society of Cutaneous Lupus Erythematosus (EUSCLE). Autoimmun Rev. 2013;12(3):444–454.
- Kuhn A, Landmann A. The classification and diagnosis of cutaneous lupus erythematosus. J Autoimmun. 2014;48–49:14–19.
- Chasset F, Richez C, Martin T, et al. Rare diseases that mimic Systemic Lupus Erythematosus (Lupus mimickers). Jt Bone Spine Rev Rhum. 2019;86(2):165–71.
- Rallis E, Korfitis C. Isotretinoin for the treatment of granulomatous rosacea: case report and review of the literature. J Cutan Med Surg. 2012;16(6):438–441.
- Company-Quiroga J, Alique-García S, Romero-Maté A. Current insights into the management of discoid lupus erythematosus. Clin Cosmet Investig Dermatol. 2019;12:721–732.
- Fairley JL, Oon S, Saracino AM, Nikpour M. Management of cutaneous manifestations of lupus erythematosus: a systematic review. Semin Arthritis Rheum. 2020;50(1):95–127.