 J Clin Aesthet Dermatol. 2020;13(4):23–34
J Clin Aesthet Dermatol. 2020;13(4):23–34
by Niamh Corduff, MBBS; Yates YY Chao, MD; Stephanie CK Lam, MBChB; Joyce Lim, MBBS; Ting Song Lim, MD; Kiran Lohia, MD; Isabel Mangubat, MD; Adri Prasetyo, MD; Atchima Suwanchina, MD; and Je-Young Park, MD
Ms. Corduff is with the Cosmetic Refinement Clinic in Geelong, Australia. Dr. Chao is with the Chao and Chiu Institute of Dermatology in Taipei, Taiwan. Ms. Lam is with the Central Health Medical Practice in Hong Kong. Dr. Lim is with Joyce Lim Skin & Laser Clinic in Singapore. Dr. Lim is with the Clique Clinic in Selangor, Malaysia. Dr. Lohia is with Isya Aesthetics in New Delhi, India. Dr. Mangubat is with Renergy Dermatology and Laser Center in the Philippines. Dr. Prasetyo is with Rejuva Skin & Beauty in Surabaya, Indonesia. Dr. Suwanchinda is with Medisci Biointegrative and Antiaging and Cosmetic Medical Center in Bangkok, Thailand. Dr. Park is with Oracle Dermatology and Plastic Surgery Center in Seoul, Korea.
FUNDING: No funding was provided for this study.
DISCLOSURES: Merz Asia Pacific, Pte. Ltd. sponsored the preparation of this manuscript and the article processing charge. Niamh Corduff is a consultant for Merz Asia Pacific and Australia. Adri Prasetyo is a consultant for Merz Asia Pacific. All other physicians report no relevant conflicts of interest.
ABSTRACT: Objective. A group of established aesthetic physicians sought to develop treatment guidelines for assessing Asian face morphologies that reflect accurate and current beauty standards across Asia.
Design. Physicians completed surveys, debated, and voted on their clinical strategies and developed an alternative simplified visual tool of assessment (SVAT) that discerns between country variations in genetic and ideal morphotypes.
Setting. Electronic and paper surveys were followed by consensus debates and voting.
Participants. Established aesthetic physicians practicing regularly on Asian patients.
Measurements. A clinically applicable SVAT was developed, which considered facial index, mid-face projection, upper and lower face shape, submalar contour, nose length and dorsal height, eye shape and brow shape, proportion of lips-to-lower face and ratio of upper-to-lower lip, and chin shape.
Results. For facial shape change, physicians always assessed the horizontal thirds, facial symmetry, and lip-chin complex profile, and also analyzed overall face shapes and Ogee curves. Criteria for creating oval-shaped faces was also defined and included treating indications, such as loss of angularity and bilateral masseter muscle hypertrophy, narrow jawlines, and longer and wider foreheads. Critical differences and similarities in country-specific aesthetic preferences, treatment requests, and considerations or strategies were uncovered, including the inadequacy of assessing overall peripheral facial shapes.
Conclusion. This consensus establishes the assessment and treatment criteria for achieving ideal shapes for Asian patients. Specific descriptors are affected by variations; therefore, we present the visual criteria for Asian facial morphotypes. We hope that physicians new to treating Asian patients can use this clinical information to improve their practice.
KEYWORDS: Face shape, Asian, anthropometric, aesthetic medicine, treatment strategy
Face shape analysis is complicated by differences in facial structures and shapes between Asian ethnicities, yet understanding how facial shapes and proportions determine attractiveness is central to positive outcomes. A recent consensus provided specific recommendations on combining minimally invasive technologies for treating Asian patients, including fillers, botulinum toxins, and energy devices.1 However, formulating optimal treatment strategies remains difficult for physicians with limited knowledge of the evaluation or creation of ideal Asian face shapes.
Widely accepted standards for facial shape evaluation, such as the Phi mask or Golden Ratio, were developed from Caucasian anatomies and reflect Western ideals of sunken cheeks and sharper, prominent zygomas.2 Applying these strategies to Asian faces is detrimental, as many Asians have brachiocephalic faces and dislike conspicuous zygomas.3,4 Koreans prefer slimmer, oval, or slightly chubby, baby-like faces with subtle zygomas.5–7 Elsewhere, Asian facial attractiveness is influenced by the neoteny of baby-like features, including larger facial upper thirds (forehead), but reduced facial lower thirds (mandible) and convex soft tissue profiles.8,9 A regional classification of Asian facial morphotypes revealed that female faces perceived as unattractive were round, square, or long.10 Asian women will request more pronounced tapers from the maxilla to the mandible to minimize the lower-third prominence and create a ‘V’-shaped face.10
Although the oval face shape is accepted as the female ideal in East Asia, the inverted triangular shape (i.e., heart shape) is also popular.11,12 A consensus meeting was convened among a group of established cosmetic physicians practicing regularly on Asian patients to develop guidelines in the assessment of Asian face morphologies. In preparing for this meeting, current methodologies were evaluated and an alternative simplified visual tool of assessment (SVAT) developed for use in clinical practice that discerns between country variations in genetic and ideal morphotypes. This consensus establishes the criteria for such assessments and establishes how to achieve ideal shapes.
Methods
Physicians were surveyed in two phases to understand their evaluation and creation of ideal face shapes for Asian patients. First, expert survey responses facilitated discussions and development of questions for a second survey using a simplified visual assessment tool. This was widely disseminated to collect insights and agreement for ethnically Chinese patients and Thai and Korean patients. The results were not ethnically stratified but were considered as a whole.
Paper-based survey. A literature review, summarized in the introduction, and survey on Caucasian and Asian face shape assessment were disseminated to the experts. Responses were collated, analyzed, and discussed. Current general facial assessment, country-specific facial feature assessment practices, and evaluations performed during oval-shaping from non-ideal shapes were surveyed. Questions were either multiple choice or open-ended.
a. Oval-shaping assessments. The prioritization criteria for determining if a face was oval, the features analyzed and treated when shaping to an oval face, and the features that were their treatment priorities were discussed.
b. General and country-specific assessments. The survey also considered factors relevant to country of practice:
i. Full-face frontal appearance evaluation.13,14 Facial type, vertical proportions, transverse proportions, facial symmetry, and the mandibular midline were considered. Evaluations included visual estimations for alar base width, intercanthal width, mouth width, bizygomatic facial width (from the most lateral point of each zygomatic arch), vertical facial height, bitemporal width, bigonial width, and facial symmetry.
ii. Facial profile evaluation. This was determined relative to the anteroposterior maxilla position, through the Frankfort plane cranial-base reference point.
iii. Other factors specific to Asian anatomies.15 Brachycephalic head shapes, flat faces (characterized by a protruding zygomatic bone in the anterolateral direction and a pronounced mandibular angle), flat noses, flat lateral facial aspects, and shallow facial depths were assessed. Indexes used to determine skull shape, cranial length-breadth index (ratio), upper facial index, transverse craniofacial index, transverse frontal index, and frontozygomatic index were discussed.
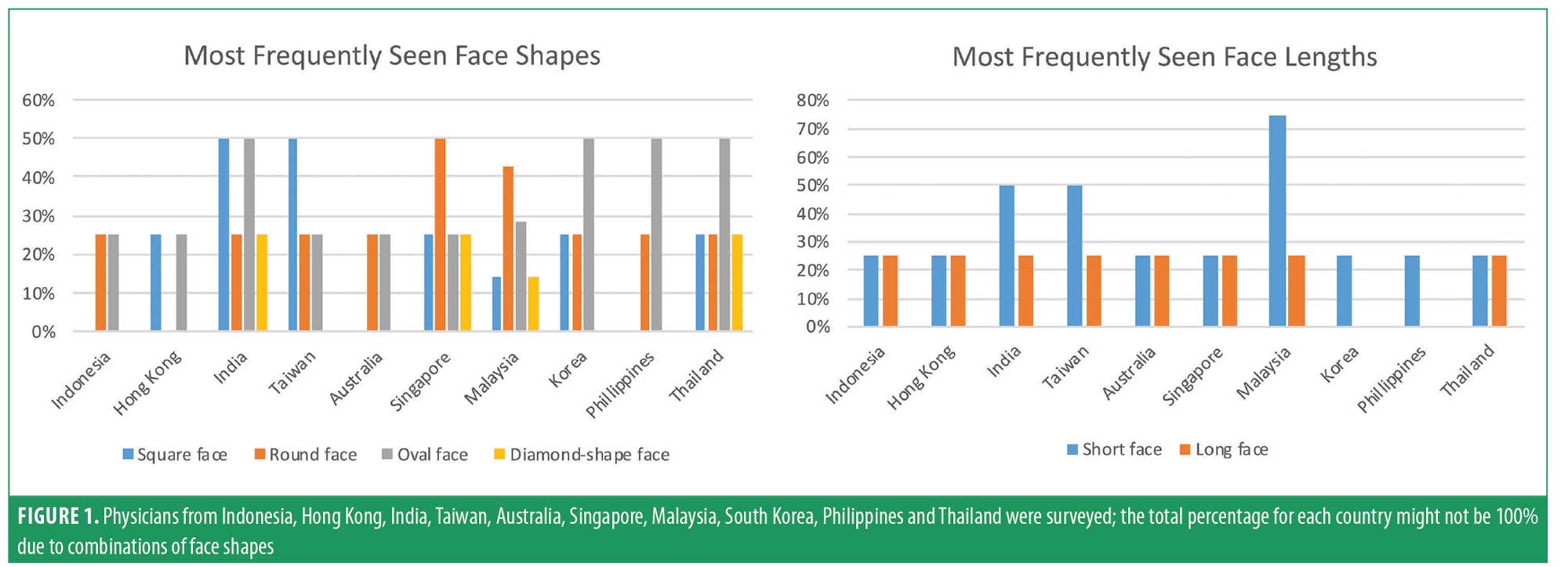
Following discussion of the survey results, factors lacking high (8/10 experts) or absolute (10/10 experts) agreement were debated. A new SVAT (Figure 1) was used to assess the dominating features and shapes of the experts’ patients and to describe the desired treatment outcomes that allowed for country-specific and racial differences. The applicability of the SVAT to Asian patient assessment was evaluated and agreed upon.
Electronic survey. Survey questions, including the use of the SVAT were adapted for electronic dissemination via SurveyMonkey (SurveyMonkey Inc. San Mateo, California, USA; www.surveymonkey.com) to physicians from Singapore (n=4), Malaysia (n=3), Thailand (n=10), Taiwan (n=36), and Korea (n=15), collectively abbreviated as Asia Pacific (APAC) physicians. Responses (n=68) were compiled using SurveyMonkey’s native spreadsheet and charting functions. A consensus was reached when more than 75 percent of physicians agreed with a response, a strong consensus was reached if more than 90 percent agreed, and absolute consensus was reached when all respondents agreed.
Results
Results of paper-based survey. The authors were surveyed on their current procedure for general face shape assessments. For facial shape change (Table 1), all (100%) experts assessed the frontal view of the horizontal thirds, facial symmetry, and facial profile of the lip-chin complex. The majority (90%) also analyzed overall shapes (e.g., diamond, square, oblong, round, and heart) and the presence of Ogee curves. Of these experts, 50 to 70 percent evaluated the facial index, relative positioning of facial landmarks, vertical-fifths and the lateral view or facial profile of the horizontal-thirds, and mandibular angle-to-menton distance. Only 20 percent evaluated the neoclassical canons of divine proportions or alignment with Golden Ratios.
Sixty percent of the expert physicians anthropometrically measured overall face shape before and after treatment, suggesting that APAC physicians find such metrics clinically impractical or unrealistic (Table 2). Those who reported doing so had no preference for particular facial angles or measurement methods. Neither eye lengths nor the adjusted relative positions of facial angles from “ideal” angles were assessed. However, 70 percent of physicians measured facial height before and after treatment (Table 3); half of these physicians also checked facial trisection proportions, further subdivided the anterior lower facial area into thirds, or measured the adjusted relative positions of facial landmarks. Only 50 percent measured facial width before and after treatment using the rule of fifths (40%) and checked that the alar base width was equal to the intercanthal distance (ICD; 40%). Twenty percent measured the adjusted relative positions of facial landmarks when assessing facial widths.

With respect to the generalized peripheral facial shape, all paper-surveyed physicians in Indonesia, Hong Kong, India, Taiwan, Australia, Singapore, Malaysia, South Korea, Philippines, and Thailand observed oval shapes and short faces (Figure 1). Diamond shapes were rarely observed. Indonesian, Hong Kong, and Australian patients presented all face shapes equally. The percentage did not total to 100 percent in all countries, as many faces were considered to be combinations of shapes, highlighting the subjectivity of physician assessment if, as in this physician sample, intuitive or experience-based assessment is used instead of standardized facial measurements.
When changing square/rectangle faces to ovals (Table 4), most experts prioritized treating masseter hypertrophy (90%), increased temporal width (80%), broad chins (80%), or non-existent chin angles. When changing round faces to ovals (Table 5), all experts examined the degree of excess soft tissue and bony deficiencies (100%), 90 percent examined the loss of angularity (due to increased submalar and mandibular soft tissue) and bilateral masseter muscle hypertrophy, and 80 percent determined if faces were circular. A highly curved hairline, unrounded cheeks, and low temples were less important factors. When changing diamond faces to ovals (Table 6), 90 percent of experts examined whether the jawline was narrow and assessed the prominence of the chin and cheekbones, which would be slightly wider than the mid-forehead, lower forehead, and jaw (80%). Physicians rarely diagnosed equal forehead and jaw widths, or a wide forehead combined with prominent cheekbones. When changing heart-shaped faces to ovals (Table 7), 90 percent of experts looked for narrow chins (90%), increased triangulation of the zygoma and chin (80%), and a longer and wider forehead (80%). Fewer experts diagnosed equivalent zygoma and lower forehead widths (50%) or prominent jaws (70%).

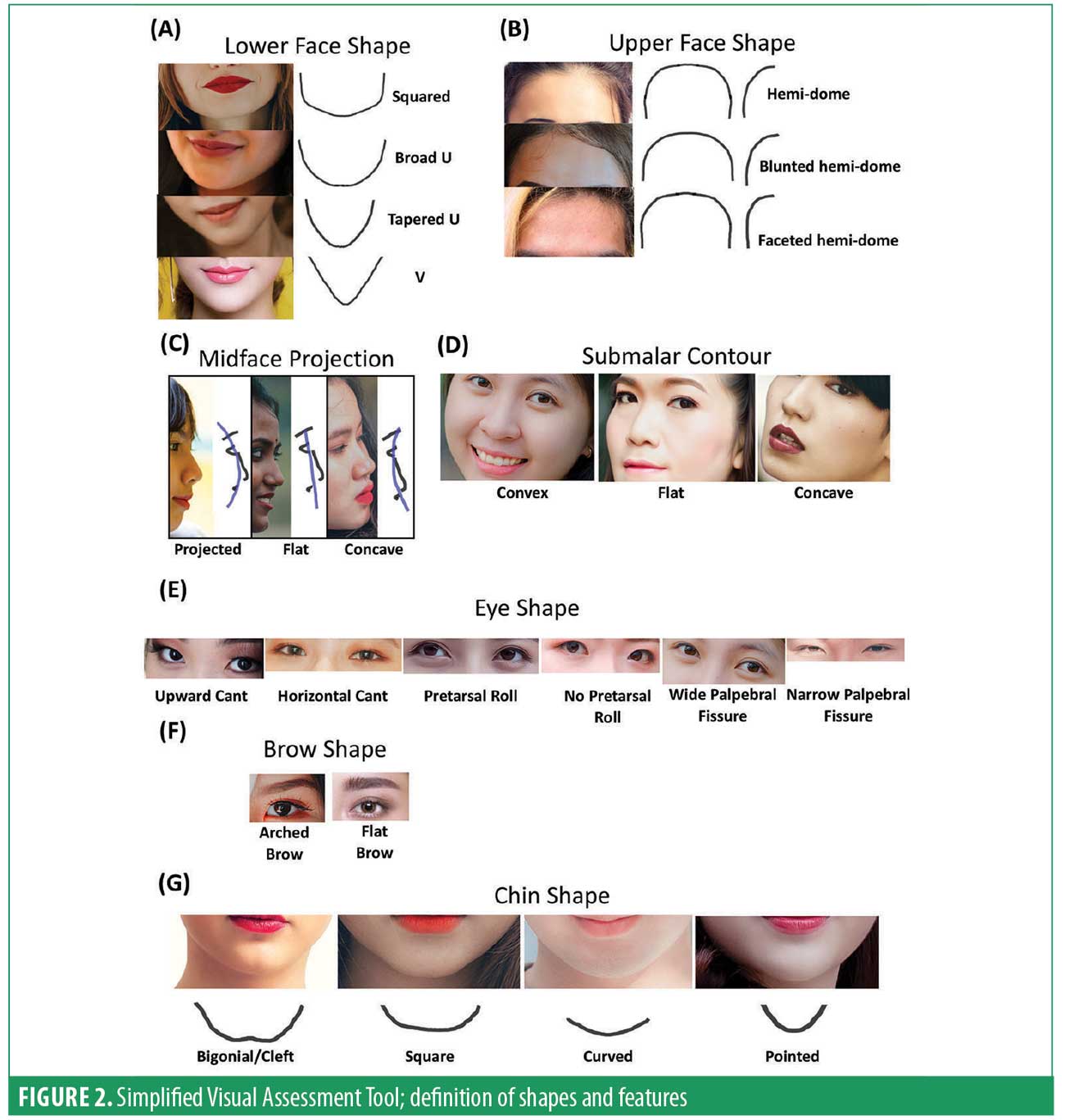
Each expert provided their country-specific aesthetic preferences and treatment requests or strategies. The overall peripheral facial shape was found to be an inadequate assessment tool to differentiate between country-specific, inherent, and desired morphologies. Sex-stratified comparisons between each country and for each facial feature considered desirable or undesirable and that are treatable using current strategies were discussed. To differentiate, current methods of assessment require detailed anthropological measurements, which, while considered the gold standard for academic purposes, are not used widely in clinical practice. Thus, the new SVAT was developed (Figure 2). To ensure consistency, all baseline characteristics, facial shapes, and features were defined prior to voting.
Facial Index (FI). FI is determined from the anteroposterior (AP) view: the height from the nasion to the gonion (i.e., tip of the chin) to the bizygomatic width (i.e., the widest point of the zygomatic arch seen from the AP). For this simple clinical guide, accurate assessment of the FI is unnecessary, but the FI can guide the assessment of long (i.e., leptoprosopic), equilateral (i.e., mesoprosopic), or short (i.e., euryprosopic) faces.
Lower face (LF) shape. The LF (Figure 2A) is viewed from the AP silhouette, from the zygomatic arches and downwards from cranially to caudally. Four LF shapes were identified:
Square shape, where the side of the face tapers vertically down from the zygomatic arch to the angle of the mandible and curves to a broad, nearly flat chin
Broad U-shape, where the side of the face has a convex curve from the zygomatic arch, a maximum (acute) curve at the mandibular angle that blends into a broad chin with a shallow convexity
Tapered U-shape, where the curve from the zygomatic arch has less convexity, and the chin curve is narrower and more convex
V-shape, where almost straight lines stretch from the zygoma arch down to a narrow, deep convexity at the chin. Therefore, the lateral-aspect curve of the square shape is the most convex, while the curve of the inferior chin is the least convex. These curves change with the lateral aspect curve, becoming least convex, while the inferior chin curve becomes most convex as the lower face becomes V-shaped.
Upper face (UF) shape. The UF (Figure 2B) is described based on the silhouette of the forehead and temple in AP and lateral views. The hairline is irrelevant, as it can be modified by hairdressers rather than injectors. The rounded hemidome UF shape comprises a well-rounded forehead and slightly convex temples. The blunted hemidome UF comprises a flatter forehead with flat temples. The faceted hemidome UF comprises a flat forehead with concave temples.
Mid-face projection. The mid-face (Figure 2C) is assessed from lateral views of the maxilla, with its overlying soft tissues forming three levels of projection: projected, flat and concave.
Nose length and dorsal height. The nose length (Figure 2C) is assessed from lateral views of the nasion to the tip, while dorsal height is graded as low, mid, or high.
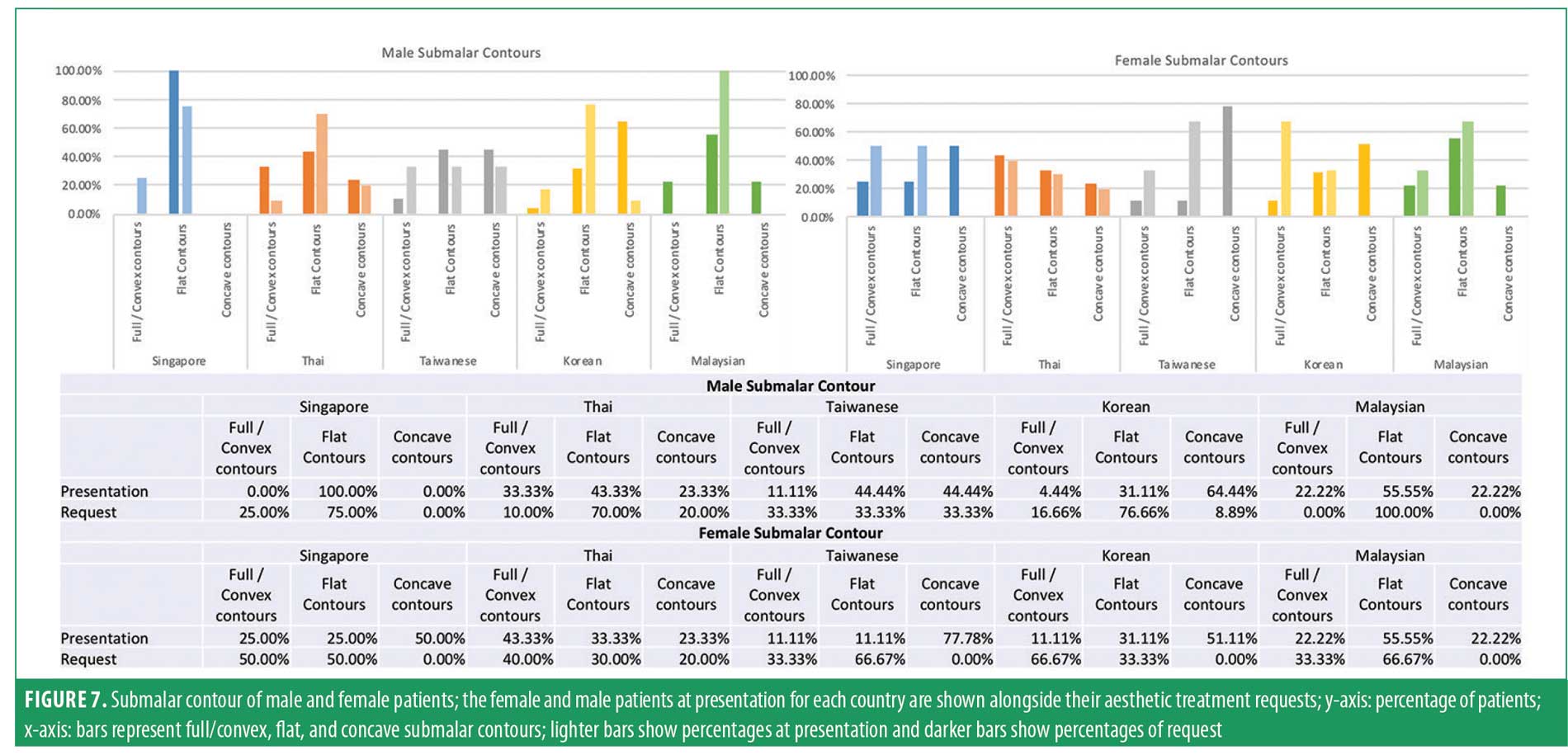
Submalar contour. The soft tissue curvature from the malar prominence to the jawline is assessed from frontal and oblique views and is classified as convex, flat, or concave (Figure 2D).
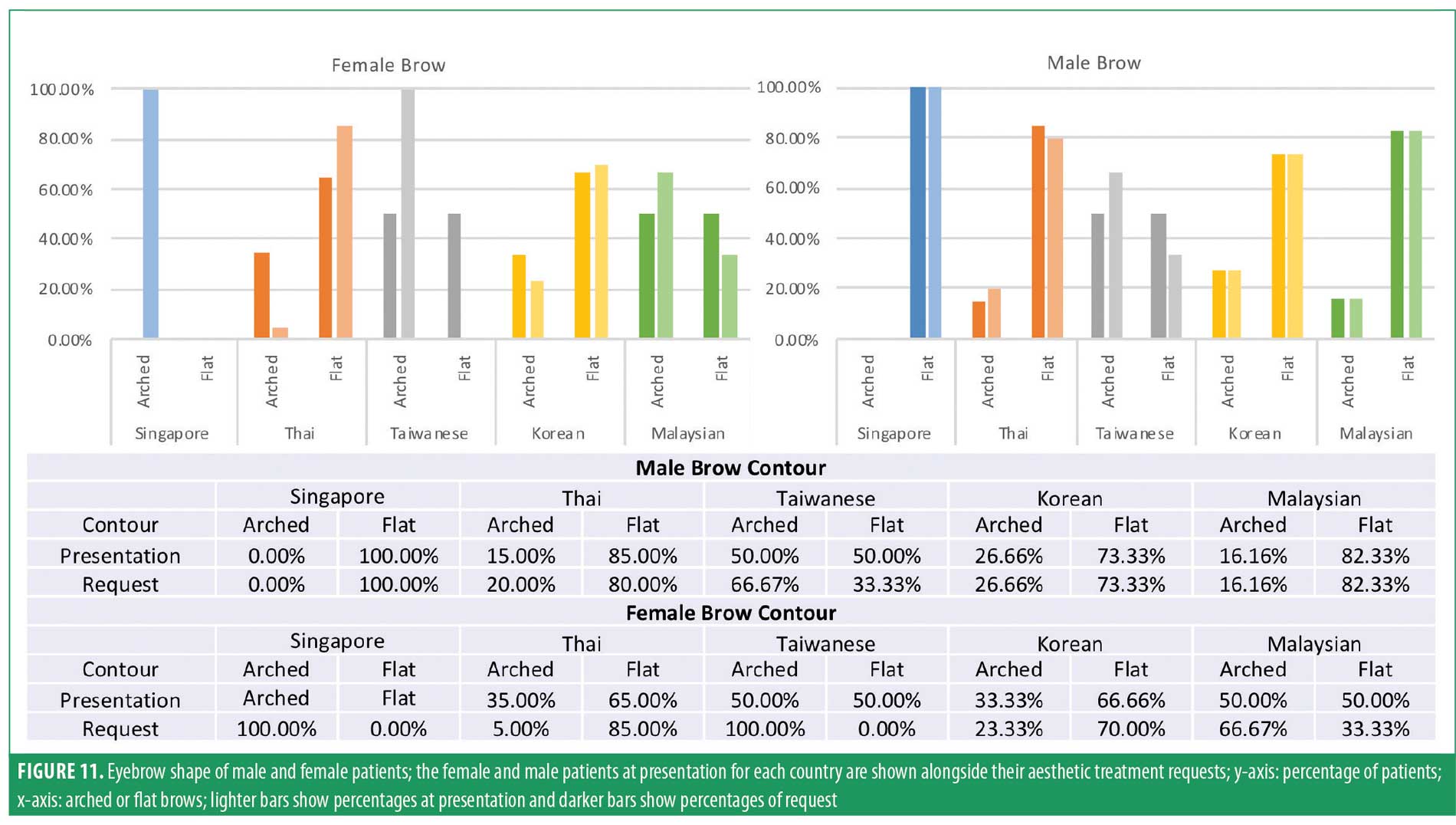
Eye shape and brow shape (Figure 2E). Whether the palpebral fissure has an upward, horizontal, or downward cant, is wide or narrow, and whether a pretarsal roll is full, has some presence or is absent, are assessed. The brow is described as arched or flat.
Proportion of lips to lower face and ratio of upper to lower lip. Lips are first assessed according to the percentage proportion of combined heights of the upper and lower lip compared with the height of the lower-third of the face (from the base of the nose to the tip of the chin). Three lip proportion grades are described: one-third, one-sixth, and in-between. Lip ratio is assessed according to the upper to lower lip ratio based on the vermillion height in the AP view and is either 1:1, 1:2, or in-between.
Chin shape (Figure 2F). Four chin shapes are described based on their combination of bony and soft tissue effects. Bigonial chins have a central cleft, square chins have a straight chin base, curved chins have a convex-curved chin base, and pointed chins have a markedly convex chin curve.
Results of electronic survey. The survey was electronically distributed to physicians in Singapore, Thailand, Malaysia, Korea, Taiwan, and India. The collected information on patient presentation and treatment requests pertains only to patients seeking aesthetic treatment, not the general public. A lack of response from Indian physicians resulted in this group being excluded from analysis.
Facial index (Figure 3). In Singapore, 58.33 percent of male patients presented with equilateral mesoprosopic faces and 33.33 percent with short euryprosopic faces; however, they preferred longer faces, with 41.66 percent requesting long leptoprosopic faces, and 41.66 percent requesting equilateral faces. In Korea, 51.11 percent of male patients presented with euryprosopic faces, yet 73.33 percent requested equilateral faces. In Malaysia, 66.67 percent of male patients had equilateral faces and no short faces, but 33.33 percent requested euryprosopic faces. Thai and Taiwanese male patients presented with and requested more equivalent facial proportions. Female patients in Thailand and Korea had predominantly short faces (63.33% and 55.55%, respectively) and preferred equilateral faces (53.33% and 66.67%, respectively). Female patients in Malaysia had mostly equilateral and long faces (44.44% each) at presentation, but 66.67 percent requested short faces.

Mid-face projection (Figure 4). Across APAC, the majority of male patients presented with flat mid-faces. Thai (23.33%), Korean (35.22%) and Malaysian (33.33%) patients also presented with concave mid-faces. They requested more projection to already projected, flat, or concave mid-faces. Female patients in Singapore, Thailand, Korea, and Malaysia presented predominantly with flat and concave mid-faces. No female concave mid-faces were reported in Taiwan. Except Malaysia, APAC physicians reported that all female patients (100%) requested projected mid-faces. Most (44.44%) Malaysians requested either projected or flat mid-faces.

Upper-face shape (Figure 5). Korean (95.55%), Singaporean (80%), Thai (83.33%), and Malaysian (77.78%) male patients presented with mostly faceted hemidomes. Malaysian male patients requested the fullness of a blunted hemidome (66.67%). Taiwanese male patients presented with a rounded (66.67%) or blunted hemidome (33.33%) and preferred less fullness. Female patients in Singapore, Thailand, Korea, Malaysia, and Taiwan had a variety of presentations, but mainly requested rounded hemidomes.

Lower-face shape (Figure 6). With respect to lower face shape, Taiwanese, Thai, and Korean male patients presented with square (33.3%, 60%, 46.67%, respectively) and broad (66.67% 40%, 53.33%, respectively) lower faces, and preferred tapering to a broad-U ( 33.33%, 50%, 46.67%, respectively) or tapered-U (33.33%, 30%, 46.67%, respectively). Singaporean and Indian male patients (60% and 66.67%, respectively) presented with broad-U shapes. Sixty percent and 66.67 percent, respectively, requested a square-shaped lower face. All APAC female patients requested narrowing of the lower face into a tapered-U or V-shape. The V-shape was most popular in Thailand, where 60 percent of female patients requested it.

Submalar contours (Figure 7). No clear pattern exists across APAC. Patients presented with convex, flat, and concave contours. However, male patients across APAC, except Taiwan, predominantly preferred flat contours. Female patients in Korea (66.67%) preferred fuller convex contours, whereas Malaysian (66.67%) and Taiwanese (66.67%) female patients preferred flat submalar contours.
Nose length and dorsal height (Figure 8). Using the SVAT, all countries had female and male patients with mostly low, mid-height, and short length (65%–100%) noses and preferred nose elongation (75%–100%) and increased dorsal height. Sixty to 100 percent of Singaporean, Thai, Korean, and Malaysian female patients requested high dorsal height noses.

Eye shape; eye cant and palpebral fissure width (Figure 9). Fifty percent of Thai male and female patients had downward cants, although a horizontal cant was most prevalent in APAC. A horizontal cant was most preferred by male patients. Further, 58.33 percent of female patients in Singapore presented with upward cants and preferred horizontal cants, while 66.67 percent of female patients in Malaysia requested upward cants. Female Thai patients that had downward (50%) or horizontal (40%) cants requested horizontal (43.30%) or upward cants (33.30%). Taiwanese and Malaysian physicians observed equivalent numbers of narrow and wide palpebral fissures in female patients, but other physicians observed mostly narrow palpebral fissures in female patients, all of whom favored wide fissures. All APAC male patients preferred wide palpebral fissures.

Eye shape; pretarsal rolls (Figure 10). Pretarsal rolls are absent in some Thai male and female patients (40% and 40%, respectively) and Taiwanese male and female patients (33.33% and 33.33%, respectively). Male patients from Singapore, Taiwan, Korea, and Malaysia (66.67%–82.22%) demonstrated pretarsal rolls and requested to create or maintain this. However, 50 percent of Thai male patients and 60 percent of Thai female patients did not want these.

Brow shape (Figure 11). All APAC male patients predominantly had flat brows and requested this; however, 66.67 percent of Taiwanese male patients preferred arched brows. APAC female patients presented with and requested both arched and flat brows. Singaporean (100%), Taiwanese (100%), and Malaysian (66.67%) female patients requested arched brows, while Thai (85%) and Korean (70%) patients requested flat brows.
Proportion of lips to lower face and ratio of upper to lower lip (Figure 12). Across APAC, the lips of most male patients occupy between one-third and one-sixth of the lower face, except in Taiwan (49.49%), where lips occupy one-third of the lower face. In all countries, most male patients preferred between one-third and one-sixth proportions. Female patients had similar proportions to males, but most requested one-third proportions; however, Malaysian patients preferred between one-third and one-sixth proportions. 100 percent of Malaysian female patients and 82.83 percent of Malaysian male patients presented with 1:1 upper to lower lip ratios, but only 66.67 percent of male and female patients requested to maintain this. Forty-five percent of Thai patients requested a 1:1 ratio. Otherwise, requested ideals for male and female patients were 1:2 or between 1:1 and 1:2.

Chin (Figure 13). A majority (76.66%) of Korean male patients presented with square chins and 90 percent of patients requested curved chins, whereas 55.55 percent of males in Malaysia had curved chins and all (100%) requested square chins. In Singapore (50%), Thailand (60%), and Taiwan (66.67%), male patients also requested square chins. Female patients in all countries tended to present with curved chins. Fifty percent of female patients in Singapore, 60.00 percent in Thailand, and all patients in Taiwan requested pointed chins, whereas only 3.33 percent of Korean and 33.33 percent Malaysian female patients requested this.

Discussion
Recently, structural differences between attractive Caucasian and Asian faces were photogrammetrically analyzed by morphing the frontal and lateral face views for each race, defining facial landmarks, and measuring relative photographic pixel distances and angles.16 Proportions were considered ideal when each facial third had equal lengths, and attractive faces had uniform measurements. Yet ratio measurements suggested that attractive faces actually fail to match the equal-fifths theory of facial proportions, implying that established standards of facial beauty are outdated, irrelevant, and do not meet current perceptions of beauty. Long-held rules and concepts about facial configurations are no longer applicable. New standards are needed for physicians seeking guidance and instruction on treating Asian patients.
Many treatment recommendations for this cohort were built on principles derived from Caucasian patients, or from physicians who treat too few patients of Asian ethnicities. Such recommendations fail to accurately capture the spectrum of physical characteristics, cultural perspectives, and aesthetic ideals of all Asian ethnicities. Worse, they suggest that Caucasian patient treatment strategies can be easily adapted to all Asian patients with only minor modifications.
Instead, it is imperative that such information be provided by physicians who regularly treat Asian patients, as these physicians have culturally sensitive and relevant expertise in this area. The physicians participating in this survey satisfy these criteria and have shared their clinical experiences and opinions in this consensus. They defined patients as having an oval face when the center of the face was at the mid-point of the intercanthal distance (ICD) in the horizontal plane, when all facial features sit on the ICD line, and when the frontal projection of the nose (i.e., tip) and chin both rest on Reidel’s plane. Cheeks must display a lateral curve with a sufficiently wide zygomatic arch and no subzygomatic depression. In the lower face, the mandible chin line must be smooth and continuous for an oval face mandibular angle, while the jaw (i.e., bigonial width) must be narrower than the forehead (i.e., temporal width). A well-projected chin and the absence of masseter hypertrophy, parotid gland hypertrophy, and prejowl sulcus indentation are necessary.
When shaping non-oval faces to the oval ideal, the experts agreed that the top areas for judging the presence of an oval shape in the upper face were the temples (e.g. temporal fullness), the cheeks (e.g. lateral cheek curve and bizygomatic width), and the jaw, chin, or masseter in the lower face (Table 4). They also agreed that oval faces must have full temples, foreheads, and cheeks. The presence of ideal facial ratios is important and includes assessments of the facial index, rule of thirds, and rule of fifths. An ideal face must also display a smooth Ogee curve and egg-shaped outline.
While the principles of ideal oval shape are applicable across APAC, significant morphological variations and ideals exist that are not addressed by this peripheral descriptor. As stated in this consensus, while anthropological measurements are the most accurate and reliable for facial assessments and developing treatment guidelines, they are not widely used in clinical practice or beyond academic centers. It is difficult for new doctors to quickly assess facial shapes in clinical practice, and a simplified, easy-to-use tool is needed to help assess facial shapes, guide treatment decisions, and ensure desired outcomes are achieved.
In arriving at this new SVAT, numerous facial shapes were evaluated from publicly available images, broken down into smaller facial regions, and classified. Example images from the internet were de-identified for use here. Consensus agreement was reached to accept and implement the SVAT for describing the morphological features that are prevalent, trendy, and desirable, which vary widely across APAC. Using this new SVAT, the consensus meeting and subsequent electronic survey identified variations in trends across the region. Singaporean and Korean male patients preferred longer, more equilateral, and proportioned faces, whereas one-third of Malaysian male patients and two-thirds of Malaysian female patients preferred shorter faces. Hong Kong and Taiwanese Chinese were usually balanced (i.e., euryprosopic) but requested longer faces (i.e., leptoprosopic-shaping). Malaysian female patients requested shorter faces, while other Asian female patients preferred evenly proportioned faces. Physicians should be aware that the mid-faces of Korean, Thai, Malaysian, and Singaporean patients can be concave, and across APAC, patients request increased mid-face projection. Thai and Korean male patients preferred a more tapered lower face, while Singaporean and Korean male patients preferred wider and more angled lower faces. While Malaysian male patients preferred blunted upper faces, Taiwanese men preferred more faceted upper faces, and APAC female patients preferred a more rounded and fuller upper face. APAC male patients preferred horizontal eye cants, while some Malaysian and Thai female patients preferred an upward cant. Thai patients of both sexes might request pretarsal roll removal. Singaporean, Taiwanese, and Malaysian female patients preferred arched brows, but flat brows were preferred by Thai and Korean female patients and all APAC male patients except Taiwanese men. The pointed chins popularized in Korean media are requested more commonly by Thai, Singaporean, and Taiwanese patients than Korean patients. In Taiwan and Hong Kong, frequently observed square or curved female chins required intervention to create pointed chins, especially in younger patients, whereas older patients favored curved chins. Chinese male patients had square or bigonial shapes and preferred these, whereas Korean male patients preferred curved chins. Taiwanese Chinese male patients had bigonial shapes but preferred slightly squarer appearances. Indonesian patients had similar aesthetic requests. Commonalities exist, such as the unpopularity of a sculpted submalar concavity (popular among Caucasians) among Asian patients, who prefer rounded or flat cheeks. Asian patients generally requested nose lengthening and raising of the dorsal height. Generally, patients preferred lips with 1:2 or between 1:1 and 1:2 upper to lower lip ratio, and to occupy one-third of the lower face. However, Malaysian female patients preferred a one-third to one-sixth ratio. In countries that are multi-ethnic, such as Malaysia, it must be emphasized that, depending on their ethnicity, both sexes might equally prefer euryprosopic, mesoprosopic, and leptoprosopic faces.
Authors from different countries had different treatment priorities when creating the ideal face shape. Singaporean physicians would treat, in order, the mid-face, the chin, and the upper face. Indian, Malaysian, and Hong Kong physicians would treat the mid-face followed by the lower face and the upper face. Taiwanese physician priorities were feature-specific, starting with the chin, then cheek volume, and, finally, the forehead. Those from Indonesia would treat the chin, temple, and, finally, the mid-face. Australian physicians would progress from the lower, to the mid, and then the upper face. These priorities are determined by midfacial aging, which can deteriorate the lower face. Thai physicians would begin by assessing the lower face aging morphology to determine the severity of aging, before progressing to the mid and upper face. However, Thai physicians that were surveyed would commence treatments from the mid-face, as this area is the true cause of visible aging and will determine the severity of visible lower face aging. They would then proceed with treating the upper face and correcting specific features, most commonly the chin.
Our summary of key facial characteristics is therefore a critical starting point for physicians planning treatments. More experienced physicians might also wish to measure the frontal horizontal thirds, facial symmetry, facial profile of the lip-chin complex, overall facial shapes, and the presence of Ogee curves. While anthropometrical measurements are unnecessary for the overall face shape or facial features, some physicians might find measuring facial heights helpful.
Conclusion
Commonly used morphotype assessment tools are based on Caucasian faces. This document is the first real-world, clinically applicable description of Asian face shape assessments from practicing and experienced clinicians, derived from a variety of Asian faces. We showed that considerable differences in Asian morphotypes and desired outcomes exist between Asian cultures. Instead of using specific country or regional descriptors, which will be affected by these variations, we presented a panel of visual criteria that can be used to assess and communicate the many differences in Asian facial morphotypes. In sharing their expertise and knowledge, the authors hope that physicians new to treating Asian patients, or those wishing to deepen their practice, now have essential clinical information on a topic for which there is great interest but little practical guidance.
Acknowledgments
The authors express their appreciation to Merz Asia Pacific, Pte. Ltd., for funding the preparation of this manuscript and Shawna Tan for manuscript writing and editorial assistance.
References
- Chao YYY, Chhabra C, Corduff N, et al. Pan-Asian Consensus–Key recommendations for adapting the World Congress of Dermatology Consensus on combination treatment with injectable fillers, toxins, and ultrasound devices in Asian Patients. J Clin Aesthet Dermatol. 2017 Aug;10(8):16–27.
- Anic-Milosevic S, Mestrovic S, Prlic A, et al. Proportions in the upper lip-lower lip-chin area of the lower face as determined by photogrammetric method. J Craniomaxillofac Surg. 2010;38:90e95.
- Hanihara T. Frontal and facial flatness of major human populations. Am J Phys Anthropol. 2000 Jan;111(1):105–134.
- Lee C. Asian Malar and Mandibular Surgery: Background, History of the Procedure, Problem. Medscape site. 26 Oct 2018. https://emedicine.medscape.com/article/1280538-overview. 7 Apr 2020.
- Hong SE, Liu SY, Kim JT, Lee JH. Intraoral zygoma reduction using L-shaped osteotomy. J Craniofac Surg. 2014;25(3):758–761.
- Kim YH, Cho BC, Lo LJ. Facial contouring surgery for asians. Semin Plast Surg. 2009;23(1):22–31.
- Marx P. The World Capital of Plastic Surgery. The New Yorker site. 16 Mar 2015. https://www.newyorker.com/magazine/2015/03/23/about-face. 7 Apr 2020.
- Bashour M. An objective system for measuring facial attractiveness. Plast Reconstr Surg. 2006;118:757e776.
- Sforza C, Laino A, D’Alessio R, et al. Soft-tissue facial characteristics of attractive Italian women as compared to normal women. Angle Orthod. 2009;79:17–23.
- Sundaram H, Huang PH, Hsu NJ, et al. Pan-Asian aesthetics toxin consensus group. Aesthetic spplications of botulinum toxin A in Asians: an international, multidisciplinary, pan-Asian consensus. Plast Reconstr Surg Glob Open. 2016 Dec 7;4(12):e872.
- Goodman GJ. The oval female facial shape–a study in beauty. Dermatol Surg. 2015 Dec;41(12):1375–1383.
- Gao Y, Niddam J, Noel W, et al. Comparison of aesthetic facial criteria between Caucasian and East Asian female populations: an esthetic surgeon’s perspective. Asian J Surg. 2018 Jan;41(1):4–11.
- Lloyd T, Pabla R, Sharma S, Hunt N. Orthognathic Surgery. In: Farhadieh R, Bulstrode N, Cugno S, eds. Plastic and Reconstructive Surgery: Approaches and Techniques. 1st edition. Chichester, West Sussex; Hoboken, NJ: John Wiley & Sons, Ltd, 2015:279–293.
- Naini FB and Gill DS. Facial Aesthetics: 2. Clinical Assessment. Dent Update 2008; 35: 159-170
- Kim HJ, Seo K, Lee HK, Kim J. Clinical Anatomy of the Face for Filler and Botulinum Toxin Injection. Springer Singapore; 2016;46.
- Rhee SC. Differences between Caucasian and Asian attractive faces. Skin Res Technol. 2017;00:1–7.