Nashida Beckett, MD, MPH, Department of Dermatology, Howard University College of Medicine, Washington, DC; Christina Lawson, BS, Department of Dermatology, Howard University College of Medicine, Washington, DC; George Cohen, MD, Department of Dermatology and Cutaneous Surgery, University of South Florida, Tampa, Florida
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Acne keloidalis nuchae is an idiopathic, scarring folliculitis characterized by the formation of papules and pustules that may ultimately develop into tumor-like masses distributed on the nape of the neck and occipital region of the scalp. This hyperproliferative disorder is most commonly seen in African-American men. While the pathogenesis remains uncertain, precipitating factors include localized trauma, chronic irritation, seborrhea, and androgen excess. The treatment of acne keloidalis nuchae is challenging and depends on the clinical stage of the disease; however, a multifaceted approach involving combination therapies has proven to be effective in some cases. Excision with healing by secondary intention is a recommended option for patients with large plaque- and tumor-stage acne keloidalis nuchae. This case report reviews the management of a patient with tumor-stage acne keloidalis nuchae successfully treated with electrosurgical excision and secondary intention healing with excellent cosmetic results and no recurrence of the disease. (J Clin Aesthet Dermatol. 2011;4(1):36–39.)
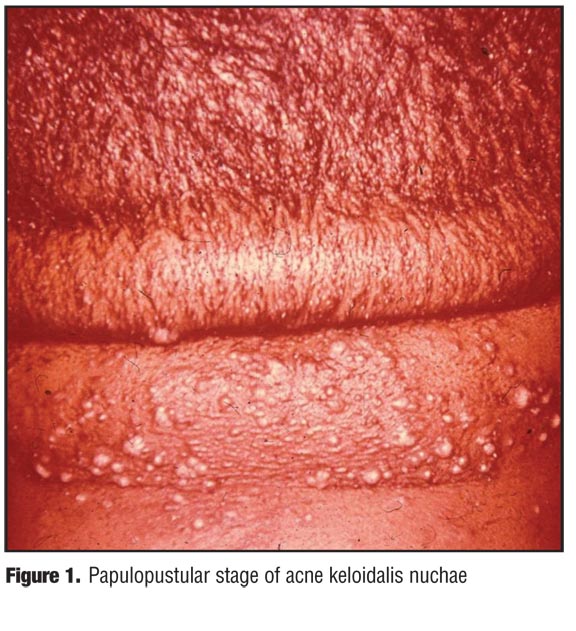
Acne keloidalis nuchae (AKN) is a chronic and often disfiguring condition of unknown etiology seen most frequently in African-American patients. Clinically characterized initially by papules and pustules on the posterior scalp and nape of the neck (Figure 1), these discrete lesions may merge to form keloidal plaques. In some patients, large keloidal masses may form. Topical agents (e.g., steroids, antibiotics, retinoids) alone or in combination have been used for mild-to-moderate cases, but the tumor stage of AKN does not respond to topical or intralesional therapy. In the authors’ experience, excision of the tumor, followed by secondary intention healing was a safe and effective method to free a patient of the unsightly keloidal masses and the associated bleeding, super-infection, and odor .
{kind=link}
Case Report
A 63-year-old African-American man presented to the dermatology clinic with a complaint of a 23-year history of “bumps on the back of the neck.” The patient stated that he had been previously treated with topical medications and intralesional corticosteroid injections without success. On physical examination, a 5x8cm keloidal mass was present on the occipital scalp representing the tumor stage of AKN (Figure 2).
{kind=link}
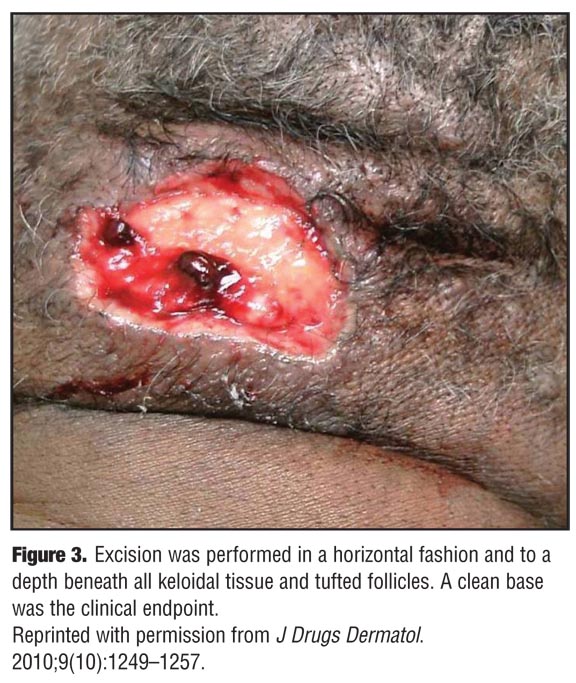
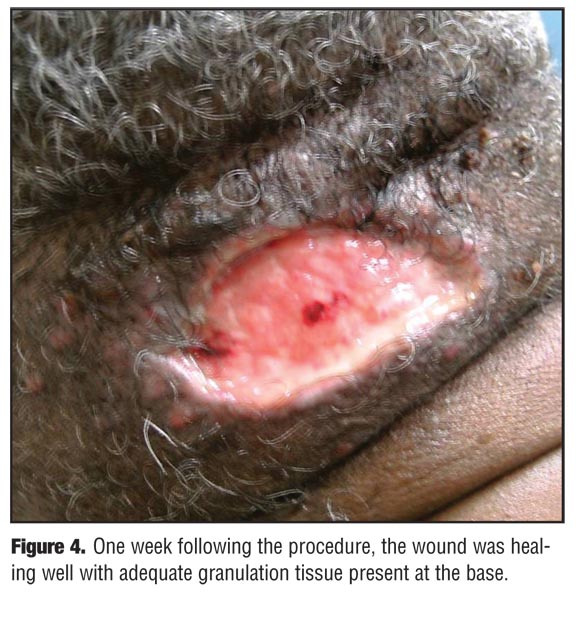
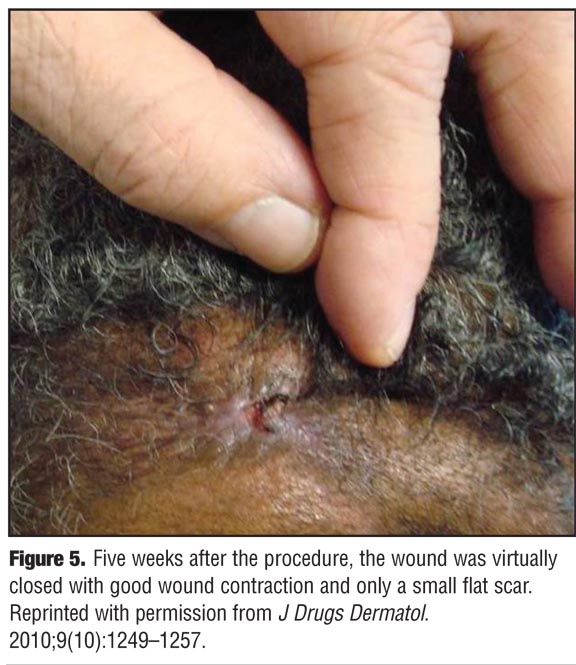
Local field block anesthesia with one-percent lidocaine with epinephrine was used prior to the excision of the tumor using an electrosurgical unit in the blended mode at a setting of 20 watts to simultaneously cut the tissue and coagulate small vessels. Excision was performed in a horizontal fashion and to a depth beneath all keloidal tissue and tufted follicles. A clean base was the clinical endpoint (Figure 3). Dressing with sterile gauze and petrolatum was applied postoperatively to keep the wound moist, and cefuroxime axetil 500mg (Ceftin, GlaxoSmithKline) twice daily was prescribed for seven days postoperatively to decrease the risk of infection. The patient was instructed to apply topical petroleum jelly, a nonadherent dressing, and gauze daily. One week following the procedure, the wound was healing well with adequate granulation tissue present at the base (Figure 4). Five weeks after the procedure, the wound was virtually closed with good wound contraction and only a small flat scar (Figure 5). At eight months follow up, there was no recurrence or need for adjuvant therapy.
{kind=link}
{kind=link}
{kind=link}
Discussion
Acne keloidalis nuchae, first described by Kaposi in 1869 as dermatitis papillaris capillitii, was coined by Bazin in 1972.[1,2] This idiopathic inflammatory condition is most commonly seen in young African-American men after puberty, representing approximately 0.45 percent of all dermatoses affecting African Americans.[3] The male-to-female ratio is approximately 20:1, and only rarely have cases of AKN been reported in women.[4,5]
Pathogenesis. AKN is a misnomer since it differs pathogenically from acne vulgaris and true keloids do not form.[3] However, the exact etiology of AKN is unknown. Many have proposed an etiology similar to that of pseudofolliculitis barbae, implicating the action of hairs curving into the skin leading to a foreign body inflammatory reaction.[4,6] Patients with AKN often cut their hair very short and may closely shave the hair on the neck. A prospective, hospital-based, observational study found that the initiating event in 90 percent of AKN cases was trauma from a haircut after the use of an electric razor.[7] Others, however, have found no histological evidence of hair shafts curving into the skin and insist that this correlation be abandoned. They instead describe this condition as a primary form of scarring alopecia similar to central centrifugal cicatricial alopecia.[8] Additional proposed etiological factors include constant irritation from shirt collars, chronic low-grade folliculitis,[9] and an autoimmune process.[2] In a small case series, four patients with AKN were found to have an associated acanthosis nigricans, suggesting that acne keloidalis may represent a cutaneous sign for the metabolic syndrome.[10] Cases of acne keloidalis occurring in Caucasian patients after cyclosporin use have also been reported.[11,12]
Clinical findings. The clinical spectrum of AKN is broad. Initial lesions are small, firm, discrete, follicular papules and pustules on the occipital scalp and posterior neck. With time, the papules coalesce into horizontal hairless keloidal plaques, which may be fringed with tufted hairs. In the most extreme forms, disfiguring tumor-like masses or abscesses exuding odiferous pus may be present. Although many cases of AKN are asymptomatic, patients may complain of pruritus or pain, and the lesions are often a cause of tremendous cosmetic concern.
Pathology. Histologically, early stages of AKN are characterized by a dense follicular and perifollicular inflammatory infiltrate consisting of neutrophils and lymphocytes.[4] In more advanced stages, disrupted and broken hair follicles become surrounded by granulomatous inflammation, perifollicular abscess formation, and dermal fibrosis.[13] The dermal fibrosis resembles the collagen fibers seen in scar tissue rather than that seen in true keloids.[4]
Medical treatment. Treatment of AKN can be challenging and is primarily empirical. The choice of therapeutic modality largely depends on the clinical stage of disease. Papulopustular lesions may respond to topical therapies, intralesional therapy, or physical modalities, while larger plaques and tumors generally require surgical excision. Topical therapies include corticosteroids, antibiotics, retinoids, and immune modulators, used as monotherapy or in combination. Class I or II topical corticosteroids applied twice daily may be efficacious and a recent open-label study found topical clobetasol propionate foam to be effective in improving mild-to-moderate lesions.[14] When pustules or other evidence of infection are present, topical clindamycin or erythromycin is warranted to decrease inflammation. Combination antibiotic and corticosteroid preparations are quite popular. Imiquimod cream prescribed daily for five consecutive days for a total of eight weeks has been successful in a few patients.[4] For mild-to-moderate cases not responsive to topical therapy, intralesional corticosteroids, usually triamcinolone acetonide, may be injected at three- to four-week intervals. Laser therapy (carbon dioxide or neodymium-doped yttrium aluminium garnet) and cryotherapy have also been proven successful in some patients.[4]
Surgical management. Surgical excision is the cornerstone of treatment for extensive plaque- and tumor-stage AKN. Surgical approaches include excision and grafting, excision with primary closure, excision with secondary intention healing, and staged excision with primary closure. Regardless of the type of closure chosen, the affected tissue must be excised to a depth extending at least to the base of the hair follicles in order to prevent recurrences.[15]
Excision with skin grafting is generally an inferior option as the cosmetic outcome is poor. Split-thickness skin grafts are typically atrophic, depressed, and do not match the surrounding skin in color, texture, or thickness.16 Excision with primary closure may also result in suboptimal cosmesis, as the surgical scar frequently stretches to a large area. In addition, this approach may restrict movement if the head has to be bent back during surgery to accomplish closure.[17] Furthermore, recurrences following excision with primary closure or skin grafting are not uncommon.[2,16,18] Primary closure in stages has been performed in order to avoid spread scars and restricted movement by closing the defect without undo tension.[16] However, this requires multiple procedures, which is inconvenient to the patient and may increase the risk of surgical complications.
Excision with secondary intention healing is an effective option in the treatment of extensive AKN that fails to respond to medical treatment or minor surgical intervention. Although the average time for wound healing is 6 to 8 weeks, this approach offers good cosmetic results as the wound often retracts to form a scar that is much smaller and flatter than the original one. Cosmesis is further improved when the excision is a horizontal ellipse of the posterior hairline and posterior aspect of the scalp, resulting in a more natural-appearing hairline.[4,16] In addition, recurrences may be fewer with secondary intention healing.[16,17,19,20] Electrosurgical excision offers the added benefit of improved hemostasis, decreasing postoperative bleeding and negating the need to tie off bleeding vessels. Some suggest that a Shaw scalpel or electrosurgical excision may produce greater postoperative pain because of additional thermal injury16,17; however, postoperative pain was not a major complaint in the patient described in this case.
Surgical removal of true keloids is almost always (50–100%) followed by even more aggressive regrowth of scar tissue. For this reason postsurgical adjuvant therapy with intralesional steroids, silicone sheets, imiquimod, or 5-flurouracil is recommended.21 Lesions of AKN, however, are not true keloids and recurrence rates are much lower. Minor recurrences are generally due to inadequate removal of hair follicles within the affected tissue.[17,20] For this reason, adjuvant therapy is not routinely recommended following surgical excision of AKN, but can be useful if an elevated scar develops after complete healing. In this case, only a small flat scar was present following electrosurgical excision, negating a need for adjuvant therapy.
Conclusion
In summary, the patient described in this case achieved excellent cosmetic results with no recurrence or postoperative complications following electrosurgical excision with secondary intention healing of tumor-stage AKN. Further research is needed to elucidate the cause of AKN. In order to develop an evidence-based approach to treating this and other hyperproliferative disorders in African-American patients, the secrets to wound healing, proliferation of fibroblasts, and the signals that regulate the scarring process must be unlocked. Empirically, electrosurgical excision of the keloidal tumors of AKN followed by secondary intention healing is a safe and effective way to eliminate the mass, pain, odor, and disfigurement of this disease. Optimal follow up and adjunctive therapy is yet to be determined.
References
1. Kaposi M. [Ueber die sogennante framboesia und mehrere andere arten von papillaren neubildungen der haut.] Arch Dermatol Syph. 1869;1:382–423.
2. Cosman B, Wolff M. Acne keloidalis. Plast Reconstr Surg. 1972;50:25–30.
3. Ogunbiyi A, George A. Acne keloidalis in females: case report and review of literature. J Natl Med Assoc. 2005;97:736–738.
4. Kelly AP. Pseudofolliculits barbae and acne keloidalis nuchae. Dermatol Clin. 2003;21:645–653.
5. Dinehart SM, Tanner L, Mallory S. Acne keloidalis in women. Cutis. 1989;44:250–252.
6. Kenny JA. Dermatoses common in blacks. Postgrad Med. 1977;61:122–127.
7. Salami T, Omeife H, Samuel S. Prevalence of acne keloidalis nuchae in Nigerians. Int J Dermatol. 2007;46:482–484.
8. Sperling LC, Homoky C, Pratt L, Sau P. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136:476–484.
9. Halder R. Hair and scalp disorders in blacks. Cutis. 1983;32:378–380.
10. Verma SB, Wollina U. Acne keloidalis nuchae: another cutaneous symptom of metabolic syndrome, truncal obesity, and impending/overt diabetes mellitus? Am J Clin Dermatol. 2010;11(6):433–436.
11. Azurdia RM, Graham RM, Weismann K, Guerin DM, Parslew R. Acne keloidalis in Caucasian patients on cyclosporine following organ transplantation. Br J Dermatol. 2000;143:465–467.
12. Carnero L, Silvestre JF, Guijarro J, Albares MP, Botella R. Nuchal acne keloidalis associated with cyclosporine. Br J Dermatol. 2001;144:429–430.
13. Vasily DB, Breen PC, Miller F. Acne keloidalis nuchae: report and treatment of a severe case. J Dermatol Surg Oncol. 1979;5:228–230.
14. Callender VD, Young CM, Haverstock CL, Carroll CL, Feldman SR. An open label study of clobetasol propionate 0.05% and betamethasone valerate 0.12% foams in the treatment of mild-to-moderate acne keloidalis. Cutis. 2005;75:317–321.
15. Kanthak FF, Cullen ML. Skin graft in the treatment of chronic furunculosis of the posterior surface of the neck (folliculitis keloidalis). South Med J. 1951;49:1154–1157.
16. Gloster HM Jr. The surgical management of extensive cases of acne keloidalis nuchae. Arch Dermatol. 2000;136:1376–1379.
17. Glenn MJ, Bennet RG, Kelly AP. Acne keloidalis nuchae: treatment with excision and second-intention healing. J Am Acad Dermatol. 1995;33:243–246.
18. Smith MJ, Odom R. Pseudofolliculitis capitis. Arch Dermatol. 1977;113:328–329.
19. Califano J, Miller S, Frodel J. Treatment of occipital acne keloidalis by excision followed by secondary intention healing. Arch Facial Plast Surg. 1995;1:308–311.
20. Bajaj V, Langtry JAA. Surgical excision of acne keloidalis nuchae with secondary intention healing. Clin and Exper Dermatol. 2007;33:53–55.
21. Juckett G, Hartman-Adams H. Management of keloids and hypertrophic scars. Am Fam Physician. 2009;80:253–260.