Mark S. Nestor, MD, PhD; Matthew B. Zarraga, DO; bHyunhee Park, DO
Dr. Nestor is Director of the Center for Clinical and Cosmetic Research, Center for Cosmetic Enhancement, Aventura, Florida;
Department of Dermatology and Cutaneous Surgery, University of Miami, Miller School of Medicine, Miami, Florida;
Drs. Zarraga and Park are Dermatology Fellow, Center for Clinical and Cosmetic Research, Aventura, Florida
Disclosure: This study was sponsored by a research grant from Erchonia Corporation, McKinney, Texas. Dr. Nestor has received honoraria as a speaker for Erchonia Corporation as well as from Zeltiq Aesthetics, Inc., and Human Med Inc. Drs. Zarraga and Park report no relevant conflicts of interest.
Abstract
Objective: To assess the safety and efficacy of low-level laser therapy as a noninvasive method for reducing upper arm circumference. Design: Randomized, double-blind study whereby healthy subjects (N=40) with a body mass index of 20 to 35kg/m2 received three 20-minute low-level laser therapy (N=20) or sham treatments (N=20) each week for two weeks. Measurements: Upper arm circumference was measured after three and six treatments and two weeks post-treatment. Primary success criterion was the proportion of subjects achieving a combined reduction in arm circumference of ?1.25cm measured at three equally spaced points between the elbow and the shoulder. Secondary outcomes included total measurement change at each time point and subjective satisfaction ratings. Results: After six treatments, the low-level laser therapy group showed a combined reduction in arm circumference of 3.7cm versus 0.2cm in the sham treatment group (p<0.0001). Significantly more subjects in the low-level laser therapy group (N=12; 60%) achieved ?1.5cm total decrease in upper arm circumference versus sham-treated subjects (N=0; 0%) (p<0.0005). Low-level laser therapy treatment resulted in a combined reduction in arm circumference of 2.2cm after three treatments and 3.7cm after six treatments (for each, p<0.0001) indicating a progressive and cumulative treatment effect. Body mass index remained unchanged for all subjects. A significantly greater number of subjects in the low-level laser therapy treatment group were satisfied with their results (p<0.05), believed their upper arm appearance improved (p<0.0005), and indicated the results exceeded expectations (p<0.05). The treatments were painless and no adverse events were reported. Conclusion: Noninvasive low-level laser therapy is safe, painless, and effective in reducing upper arm circumference and is associated with a high degree of subject satisfaction. (J Clin Aesthet Dermatol. 2012;5(2):42–48.)
Noninvasive body contouring is one of the fastest growing segments of the cosmetic aesthetic industry.[1] Surgical options carry disadvantages, such as the use of anesthetics,[2] pain, swelling, and long recovery,[3] and there is an increasing public demand for procedures with fewer side effects and shorter recovery times. Many new noninvasive body contouring technologies have been developed including suction-massage, radiofrequency energy, high-frequency focused ultrasound, cryolipolysis, and low-level laser therapy (LLLT).[4–13]
LLLT has been shown to be an efficacious adjunct therapy for numerous cosmetic procedures, including breast augmentation and lipoplasty.[14,15] With regard to body contouring, a randomized, double-blind, sham-controlled study using a 635nm LLLT device (Zerona®, Erchonia Corporation, McKinney, Texas) showed circumferential reduction of the waist, hips, and thighs following six treatments administered over a two-week period.[14–17] This device has been shown to provide other significant clinical benefits including reduction in cholesterol and leptin levels while remaining noninvasive and relatively risk free.[18] This device has been cleared by the United States Food and Drug Administration (FDA) as a noninvasive dermatological aesthetic treatment for the reduction of circumference of hips, waist, and thighs. The biochemical mechanism of action of LLLT appears to increase cyclic adenosine monophosphate (cAMP) production via cytochrome C oxidase activation, which causes the breakdown of cell lipids in adipocytes and the formation of transitory pores in their cell membrane with subsequent cell collapse.[19–21] Therefore, LLLT appears to provide a safe and effective alternative for the reduction of subcutaneous tissue volume.
The objective of the following double-blind, randomized, sham-controlled study was to assess the safety and efficacy of LLLT as a noninvasive method for reducing upper arm circumference.
METHODS
Study subjects. The study enrolled men and women (N=40) aged 18 to 65 years with a body mass index (BMI) of 20 to 35kg/m2. Participating subjects were randomized in a double-blind fashion to receive LLLT (N=20) or sham treatment (N=20). Subjects were required to meet the American Academy of Cosmetic Surgery criteria for brachioplasty22 and indicate their ability and willingness to maintain their usual diet and exercise regimen for the duration of the study. Subjects agreed to refrain from participating in any other body contouring or weight loss procedures or programs during the course of the study including, but not limited to, over-the-counter and prescription appetite suppressants, diet plans, surgical procedures, and alternative therapies.
Reasons for exclusion from participation in the study included chronic illness, such as diabetes mellitus and cardiovascular disease; prior cardiac surgery or implanted pacemaker; active or recurrent cancer, ongoing chemotherapy, or radiation therapy; mastectomy or other surgery involving the axillary lymph nodes; medical conditions known to cause weight changes, bloating, or edema; prior surgical intervention for weight loss or sculpting of the arms; active infection, wounds, or external trauma to the areas to be treated; mental illness or developmental disability that in the professional judgment of the investigator may preclude the comprehension of informed consent or jeopardize the objectives of the study; photosensitivity disorder; participation in any type of research during the past 30 days; breast feeding, pregnancy, or planned pregnancy prior to the end of study.
Treatment device. The low-level laser energy device is a noninvasive dermatological aesthetic treatment cleared by the FDA for use as a noninvasive aesthetic dermatological treatment for reducing the circumference of hips, waist, and thighs. The LLLT device consists of four independent diodes that are positioned 120 degrees apart and tilted at a 30-degree angle. A fifth diode is positioned at the centerline. The 17mW of red 635nm of laser light emitted from each diode is collected and processed through a proprietary lens that redirects the beam with a line refractor. The refracted light from each diode is bent into a random spiraling circle pattern that is independent of the other diodes. These overlapping patterns ensure total coverage of the target treatment area. The total amount of energy delivered to the skin during each treatment was 3.94J/cm2.
Procedure. Each subject was randomized to receive six active or sham treatments 2 to 3 days apart with the low-level energy laser device over a two-week period. Both the test and sham devices have the same physical appearance and emit light when activated that is indistinguishable to both the subject and the administration investigator. The investigator and subjects were provided with eye protection during the laser procedure.
Study assessments. The circumference of each upper arm was measured using a flexible tape measure at three equally distributed points between the elbow (olecranon) and the shoulder (acromion) while the arm was in a relaxed state. For each arm, the distance from the tip of the elbow to each measurement point was recorded at baseline to ensure that subsequent measurements were obtained at the same location. All arm circumference measurements were performed by a member of the investigative team not involved in performing LLLT treatments.
The primary outcome measure was the number of subjects achieving a total decrease in arm circumference of ?1.25cm for the three combined measurement points after two weeks (6 LLLT treatments) and the mean difference between the combined arm circumference measurements for the active treatment and sham groups at all time points. Secondary outcomes assessed at the completion of the study included changes in BMI and several subjective ratings, which measured subject attitudes about overall satisfaction with their results, improvements in the appearance of their upper arms, and their treatment expectations using five-point rating scales.
All study assessments were performed at baseline, at the completion of treatment, and two weeks post-treatment. Following the baseline physical examination, a blinded investigator noted any changes in existing skin condition including scars, cellulite, stretch marks, discoloration, stria, dimpling, and skin quality and elasticity following treatment. Details about food and drink consumption, physical activity, and adverse events for each subject were recorded daily.
Statistical analysis. For the primary efficacy outcome, Fischer’s exact test for two independent proportions was used to compare the proportion of successes between treatment groups. Analysis of variance (ANOVA) was used to compare changes in upper arm circumference measurements across four time points for each treatment group. The Tukey HSD test for post-hoc analysis was used to assess for significant changes between Baseline and Week 1, Week 1 and Week 2, Baseline and Week 2, Baseline and two weeks post-treatment, and Week 1 and 2 weeks post-treatment. Fischer’s exact test was also used to compare the two positive responses for each subjective assessment question with the two negative responses, such as “Improved a lot” and “Improved a little” versus “Worsened a little” and “Worsened a lot.” For each analysis, significance was established at p<0.05.
Ethics. The protocol used in this study adhered to the Good Clinical Practice guidelines of the International Conference on Harmonization and was approved by an independent Institutional Review Board (U.S. IRB, Miami, Florida, #2011 CCCR/01). Informed written consent was obtained from each subject prior to participation in any study-related activities.
RESULTS
Demographics. The entire study protocol was completed by all enrolled subjects. Thirty nine subjects were female and one subject was male. Subject ages ranged from 22 to 65 years with no significant age difference between the two treatment groups (Table 1).
{kind=link}
Upper arm circumference. Among the subjects undergoing LLLT treatment, 12 (60%) achieved a ?1.5cm decrease in upper arm circumference versus 0 (0%) of the sham-treated subjects (p<0.0005). The LLLT treatment group showed a 3.7cm combined reduction in arm circumference versus a 0.2cm reduction in the sham treatment group after the six treatments and at the two-week post-treatment assessment (for each, p<0.0001). A 2.2cm reduction in total circumference measurement occurred following the first week of three laser procedures (p<0.0001) and a 3.7cm reduction following the second week of three laser procedures (p<0.0001), indicating a progressive and cumulative treatment effect of the laser (Figure 1). For the right arm, there was a significant decrease in circumference between Baseline and Week 1 (p<0.01) and between Week 1 and Week 2 (p<0.01), which remained stable between Week 2 and Week 4. Similarly for the left arm, there was a significant decrease in circumference between Baseline and Week 1 (p<0.01) and between Week 1 and Week 2 (p<0.05), which remained stable between Week 2 and Week 4. For sham-treated subjects, there were no statistically significant changes detected between any time points for either arm.
{kind=link}
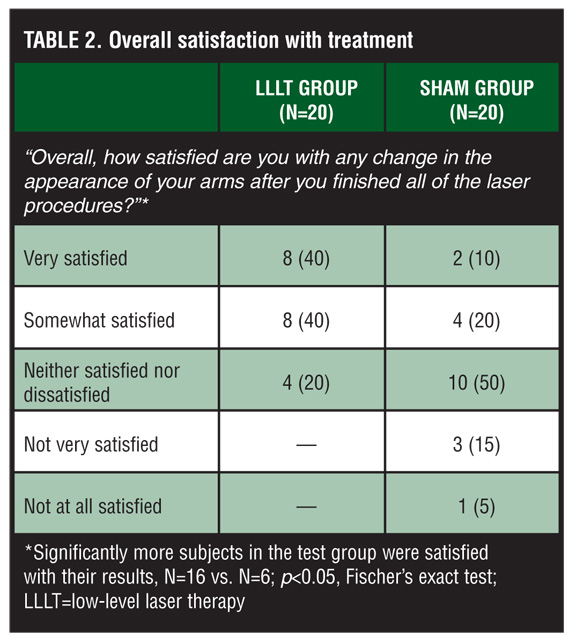
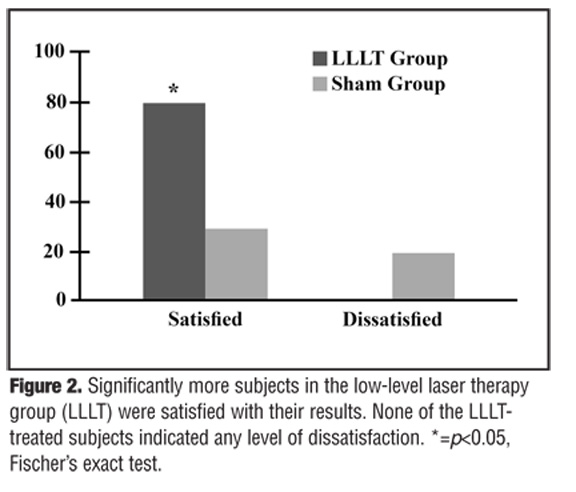
Subject satisfaction assessments. With respect to subjective measures, a significantly greater number of subjects in the LLLT group was satisfied with its results (N=16 vs. N=6; p<0.05) (Table 2, Figure 2
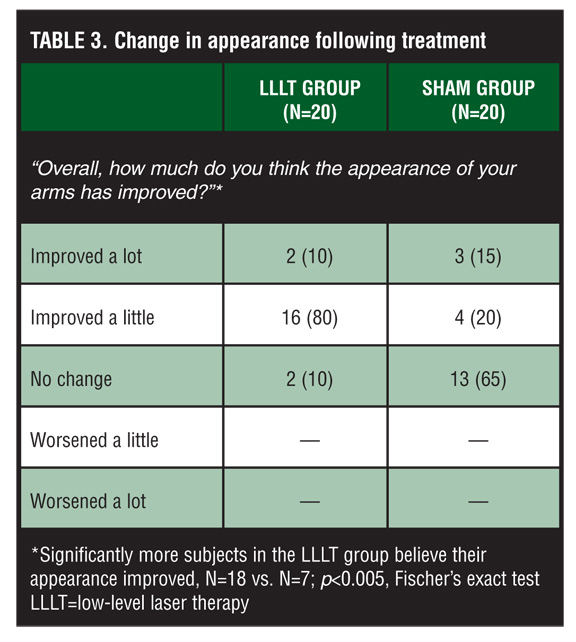
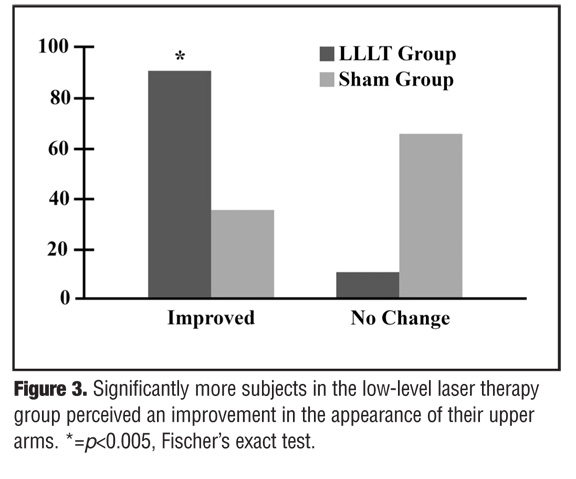
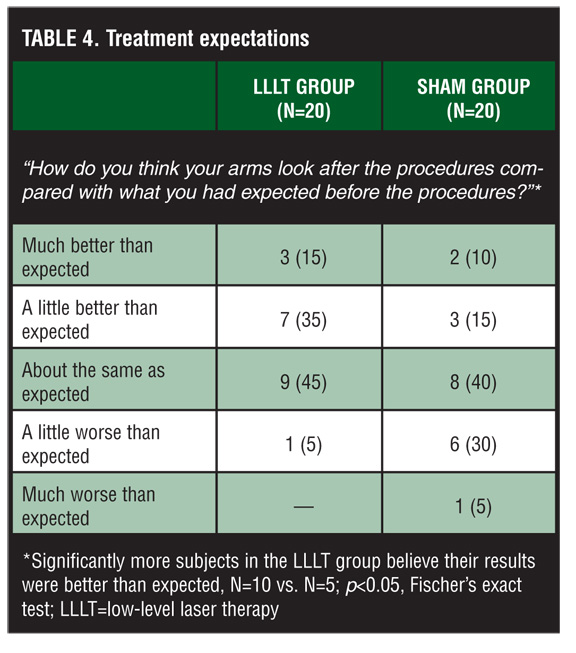
). A significantly higher number of LLLT-treated subjects also indicated the appearance of their upper arms improved (N=18 vs. N=7; p<0.005) (Table 3, Figure 3) and believed that the beneficial effects of the laser procedure exceeded their expectations (N=10 vs. N=5; p<0.05) (Table 4, Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Body mass index. BMI measurements did not change significantly across or between any of the three measurement points for either LLLT- or sham-treated subject groups. For subjects in the LLLT group, the mean (standard deviation, SD) BMI was 27.96 (5.00), 28.12 (5.09), and 27.97 (5.07) at Baseline, end of treatment, and two weeks post-treatment, respectively, while the mean BMI for the sham-treated subjects was 28.59 (4.86), 28.69 (4.95), and 28.69 (4.93) at the same time points. Further, there were no deviations from baseline diet and exercise patterns or concomitant medication use that might impact study outcome measures.
Safety. No treatment associated pain or discomfort of any kind was reported by the subjects. No changes in baseline physical examination of the treatment areas were observed and there were no reports of adverse events.
DISCUSSION
Low-level light therapy has been shown to provide a safe and effective therapeutic option for several clinical applications including acute pain associated with rheumatoid arthritis,[23] osteoarthritis,[24] and neck pain.[25] It has also been shown to increase the speed of wound healing[26,27] and curing infections around dental implants.[28] More recently, it has been shown that LLLT can be used as a method for performing noninvasive body contouring.[29]
The biochemical effects of low-level energy laser on adipose tissue appears to be mediated through an effect on cytochrome C oxidase, a large mitochondrial membrane enzyme that facilitates the transfer of electrons from cytochrome C to oxygen. In this manner, LLLT stimulates the mitochondria in adipocytes to increase adenosine triphosphate (ATP) synthesis with subsequent upregulation of cAMP. The increased cAMP stimulates cytoplasmic lipase, which converts triglycerides into fatty acids and glycerol, which can pass through pores formed in the cell membrane.[20,21] In a study conducted by Neira et al,[30] high magnification scanning and transmission electron microscope images of adipose tissue revealed this transitory pore formation. Following the application of low-level laser energy, fatty acids, glycerol, and triglycerides pass across the membrane through these transitory pores and into extracellular space resulting in complete adipocytes deflation.[30] It is presumed that triglyceride and fatty acid oxidization occurs within the extracellular space.[18,21,31–40]
Although significant clinical and histological effects of LLLT on adipocytes have been demonstrated, some skepticism regarding the clinical effectiveness of LLLT as well as potential confounding variables persist. A recent study conducted by Elm et al[41] showed no significant reduction in waist circumference at either seven days or one month following LLLT treatment; however, this study was flawed in three important ways: first, the number of subjects was extremely small (N=5); second, only partial body sites were treated; and finally, one of the authors failed to disclose a significant conflict of interest.[41]
Conversely, the double-blind, placebo-controlled trial conducted by Jackson et al[16] randomized 67 subjects to undergo six laser treatments over a two-week period (three treatments weekly spaced two days apart) with a multiple diode head, low-level laser (635nm, 17mW; N=35), or sham treatment with a multiple-head non-laser light emitting diode (635nm, 2.5mW; N=32). Following treatment, the decrease in total circumference measurements was significantly greater for the LLLT subjects at all time points. No adverse events were reported.[16,42]
Although it had been hypothesized that fat released following LLLT treatment may appear in the bloodstream where it might adversely affect the lipid profile, a nonrandomized, uncontrolled study that assessed serum triglyceride and cholesterol levels subsequent to LLLT showed an actual reduction in both serum cholesterol and leptin levels.[18]
In summary, the results of this double-blind, controlled, randomized study designed to assess the efficacy of 635nm LLLT in reducing upper arm circumference demonstrated a significant progressive and cumulative treatment effect among treated subjects. Any potential confounding variables from a prior body contouring study including diet, supplements, and measuring errors were satisfactorily addressed. Since all study participants were blinded as to whether or not they were in the treatment group, and no study participants in either group experienced a change in BMI or deviated from baseline diet and exercise patterns, the authors conclude that the decrease in arm circumference is the result of LLLT treatments. Subjective evaluations confirmed the effectiveness of the treatments. Further studies will optimize the results of 635nm LLLT, investigate other possible indications for treatment, and assess the overall metabolic effect of treatment.
CONCLUSION
Noninvasive LLLT was significantly more effective at reduction of arm circumference than sham treatments at every tested time point. This study showed significant results without any apparent confounding variables. Subjective assessments were significantly positive for the treatment group. No pain or discomfort of any kind was associated with treatment and no adverse events were reported by any subject throughout the study. Together, these results indicate low-level energy laser treatment appears to be a safe and effective method for noninvasively reducing upper arm circumference.
ACKNOWLEDGMENT
The authors acknowledge the assistance of Dr. Carl S. Hornfeldt during the preparation of this manuscript.
References
1. Body Shaping and Cellulite Reduction: Technology Proliferation Driven by Demand. Aliso Viejo, CA: Medical Insight, Inc.; 2009.
2. Sood J, Jayaraman L, Sethi N. Liposuction: anaesthesia challenges. Indian J Anaesth. 2011;55:220–227.
3. Dhami LD. Liposuction. Indian J Plast Surg. 2008;41(Suppl): S27–S40.
4. Winter ML. Post-pregnancy body contouring using a combined radiofrequency, infrared light and tissue manipulation device. J Cosmet Laser Ther. 2009;11:229–235.
5. Brightman L, Weiss E, Chapas AM, et al. Improvement in arm and postpartum abdominal and flank subcutaneous fat deposits and skin laxity using a bipolar radiofrequency, infrared, vacuum and mechanical massage device. Lasers Surg Med. 2009;41:791–798.
6. Anolik R, Chapas AM, Brightman LA, et al. Radiofrequency devices for body shaping: a review and study of 12 patients. Semin Cutan Med Surg. 2009;28:236–243.
7. Moreno-Moraga J, Valero-Altes T, Martinez Riquelme A, et al. Body contouring by non-invasive transdermal focused ultrasound. Lasers Surg Med. 2007;39:315–323.
8. Teitelbaum SA, Burns JL, Kubota J, et al. Noninvasive body contouring by focused ultrasound: safety and efficacy of the Contour I device in a multicentered, controlled clinical study. Plast Reconstr Surg. 2007;120:779–789.
9. Gadsden E, Aguilar MT, Smoller BR, Jewell ML. Evaluation of a novel high-intensity focused ultrasound device for ablating subcutaneous adipose tissue for noninvasive body contouring: safety studies in human volunteers. Aesthet Surg J. 2011;31:401–410.
10. Dover J, Burns J, Coleman S, et al. A prospective clinical study of noninvasive cryolypolysis for subcutaneous fat layer reduction-interim report of available subject data. Lasers Surg Med. 2009;S21:45.
11. Manstein D, Laubach H, Watanabe K, et al. Selective cryolysis: a novel method of non-invasive fat removal. Lasers Surg Med. 2009;40(S20):595–604.
12. Manstein D, Laubach H, Watanabe K, et al. A novel cryotherapy method of non-invasive, selective lipolysis. Lasers Surg Med. 2008;40(S20):104.
13. Coleman SR, Sachdeva K, Egbert BM, et al. Clinical efficacy of noninvasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg. 2009;33:482–488.
14. Mulholland RS, Paul M, Chalfoun C. Noninvasive body contouring with radiofrequency, ultrasound, cryolipolysis, and low-level laser therapy. Clin Plastic Surg. 2011;38: 503–520.
15. Jackson R, Roche G, Butterwick JK, et al. Low level laser-assisted liposuction: 2004 clinical trial of its effectiveness for enhancing ease of liposuction procedures and facilitating the recover process for patients undergoing thigh, hip and stomach contouring. Am J Cosmet Surg. 2004;21:191–198.
16. Jackson RF, Dedo DD, Roche GC, et al. Low-level laser therapy as a non-invasive approach for body contouring: a randomized, controlled study. Lasers Surg Med. 2009;41: 799–809.
17. Neira R, Ortiz-Neiraq C. Low-level laser-assisted liposculpture: clinical report of 700 cases. Aesthetic Surg J. 2002;22:451–455.
18. Maloney R, Shanks S, Jenney E. The reduction in cholesterol and triglyceride serum levels following low-level laser irradiation: a non-controlled, non-randomized pilot study. Laser Srug Med. 2009;21S:66.
19. Karu TI. Mitochondrial signaling in mammalian cells activated by red and near-IR radiation. Photochem Photobiol. 2008;84:1091–1099.
20. Karu T. Photobiology of low-power laser effects. Health Phys. 1989;56:691–704.
21. Karu TI, Afanasyeva NI. Cytochrome C oxidase as primary photoacceptor for cultured cells in visible and near IR regions. Doklady Akad Nauk (Moscow). 1995;342:693–695.
22. Gilmore JE AR, Fragen RA, et al. 2006 Guidelines for Liposuction Surgery. Chicago, IL: American Academy of Cosmetic Surgery; 2006.
23. Brosseau L, Robinson V, Wells G, et al. Low level laser therapy (Classes I, II and III) for treating rheumatoid arthritis. Cochrane Database Syst Rev. 2005;4:CD002049.
24. Jamtvedt G, Dahm KT, Christie A, et al. Physical therapy interventions for patients with osteoarthritis of the knee: an overview of systematic reviews. Phys Ther. 2008;88:123–136.
25. Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet. 2009;374:1897–1908.
26. da Silva JP, da Silva MA, Almeida AP, et al. Laser therapy in the tissue repair process: a literature review. Photomed Laser Surg. 2010;28:17–21.
27. Posten W, Wrone DA, Dover JS, et al. Low-level laser therapy for wound healing: mechanism and efficacy. Dermatol Surg. 2005;31:334–340.
28. Sculean A, Schwarz F, Becker J. Anti-infective therapy with an Er:YAG laser: influence on peri-implant healing. Expert Rev Med Devices. 2005;2:267–276.
29. Jewell ML, Solish NJ, Desilets CS. Noninvasive body sculpting technologies with an emphasis on high-intensity focused ultrasound. Aesthetic Plast Surg. 2011 Apr 1. Epub ahead of print.
30. Neira R, Arroyave J, Ramirez H, et al. Fat liquefaction: effect of low-level laser energy on adipose tissue. Plast Reconstr Surg. 2002;110:912–922.
31. Karu T. Ten Lectures on Basic Science of Laser Phototherapy. Grangesberg, Sweden: Prima Books AB; 2007.
32. Lubart R, Eichler M, Lavi R, et al. Low-energy laser irradiation promotes cellular redox activity. Photomed Laser Surg. 2009;23:3–9.
33. Terenin AN. Photochemistry of Dyes and Other Organic Compounds. Moscow, Leningrad: Publishing House of the USSR Academy of Science; 1947.
34. Marcus RA, Sutin N. Electron transfer in chemistry and biology. Biochm Biophys. 1985;811:265–322.
35. Konev SV, Belijanovich LM, Rudenok AN. Photoreactivations of the cytochrome oxidase complex with cyanide: the reaction of heme a3 photoreduction. Membr Cell Biol (Moscow). 1998;12:743–754.
36. Byrnes KR, Wu X, Waynant RW, et al. Low power laser irradiation alters gene expression of olfactory ensheathing cells in vitro. Lasers Surg Med. 2005;37:161–171.
37. Geiger PG, Korytowski W, Lin F, et al. Lipid peroxidation in photodynamically stressed mammalian cells: use of cholesterol hydroperoxides as mechanistic reporter. Free Radic Biol Med. 1997;23:57–68.
38. Geiger PG, Korytowski W, Girotti AW. Photodynamically generated 3-beta-hydroxy-5 alpha-cholest-6-ene-5-hydroperoxide: toxic reactivity in membranes and susceptibility to enzymatic detoxification. Photochem Photobiol. 1995;62:580–587.
39. Klebanov GI, Chichuk TV, Osipov AN, et al. The role of lipid peroxidation products in the effect of He-Ne laser on human blood leukocytes. Biofizika. 2005;50:862–866.
40. Vladimirov IuA, Klebanov GI, Borisenko GG, et al. Molecular and cellular mechanisms of the low intensity laser radiation effect. Biofizika. 2004;49:339–350.
41. Elm CM, Wallander ID, Endrizzi B, Zelickson BD. Efficacy of a multiple diode laser system for body contouring. Lasers Surg Med. 2011;43:114–121.
42. Turok D. A new non-invasive approach for body contouring: the application of low-level laser therapy. Anti-Aging Medical News. 2009;Winter:31–33.