Mark S. Nestor, MD, PhD; Glynis R. Ablon, MD
Dr. Nestor is from Center for Clinical and Cosmetic Research, Aventura, Florida; Department of Dermatology, University of Miami, Miller School of Medicine, Miami, Florida; Dr. Ablon Skin Institute, Manhattan Beach, California; Department of Dermatology, UCLA School of Medicine, Los Angeles, California
Disclosure: This study was supported through an investigator-initiated research grant from Medicis Aesthetics Inc., Scottsdale, Arizona. The development of the protocol, data collection, analysis, and interpretation of study results were conducted solely by the investigators. Dr. Nestor is a consultant for and has received research grant support from Medicis Aesthetics, has received research grant support from Merz, and has served as a consultant and speaker for Allergan. Dr. Ablon has served as a consultant for Medicis Aesthetics.
Abstract
Objective: To measure and compare the duration of action of abobotulinumtoxinA and onabotulinumtoxinA. Design: Randomized, double-blind, contralateral (split-face) study. Setting: Two United States clinical sites. Participants: Twenty subjects with severe frontalis lines at maximum elevation. Measurements: Subjects randomly received equal volumes of abobotulinumtoxinA or onabotulinumtoxinA (0.2mL) in five injection points on contralateral sides of the frontalis (N=40) using a dose ratio of 2.5:1.0 (total 25U abobotulinumtoxinA:10U onabotulinumtoxinA), respectively. Subjects were evaluated using a 4-point Frontalis Rating Scale and a new objective Frontalis Activity Measurement Standard for 210 days using predefined endpoints for efficacy. Results: Using the Frontalis Activity Measurement Standard, the median duration of “complete efficacy” was 72 days for abobotulinumtoxinA and 56 days for onabotulinumtoxinA (p=0.01), “full efficacy” was 103 days for abobotulinumtoxinA and 87 days for onabotulinumtoxinA (p<0.003), and “partial efficacy” was 105 days for abobotulinumtoxinA and 99 days for onabotulinumtoxinA (p=0.006). Using the Frontalis Rating Scale, the median duration of “complete efficacy” was 63 days for abobotulinumtoxinA and 44 days for onabotulinumtoxinA (p=0.006), “full efficacy” was 119 days for abobotulinumtoxinA and 77 days for onabotulinumtoxinA (p=0.005), and “partial efficacy” was 160 days for abobotulinumtoxinA and 145 days for onabotulinumtoxinA (p=NS). Adverse events included local bruising and occasional headache, but no significant inter-group differences. Conclusion: The contralateral Frontalis Activity Measurement Standard is well-suited for assessing the pharmacodynamic and clinical attributes of botulinum toxin type A and can be used to measure differences in the clinical properties of abobotulinumtoxinA and onabotulinumtoxinA. Using a dose ratio of 2.5:1.0, abobotulinumtoxinA displayed significantly longer duration of action than onabotulinumtoxinA.
(J Clin Aesthet Dermatol. 2011;4(9):43–49.)
The safety and effectiveness of abobotulinumtoxinA (ABO; Dysport™, Medicis Aesthetics, Inc., Scottsdale, Arizona; Azzalure®, Galderma Laboratories, Lausanne, Switzerland) and onabotulinumtoxinA (ONA; Botox® Cosmetic and Vistabel®, Allergan, Inc., Irvine, California) for aesthetic applications is well-established.[1–5] Both products share the same pharmacology and each is indicated for the temporary improvement of moderate-to-severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients 65 years of age or younger[6,7]; however, ABO and ONA differ with respect to unit potency and their nontoxin protein content due to differences in manufacturing.[8,9]
Therefore, each product possesses unique pharmacodynamic properties.[10] Clinical studies have attempted to compare the effectiveness and duration of ABO and ONA products, but lacked an objective system for measuring their effects on muscle activity.[11–16] Due to subjective and inconsistent assessment methods, clinical comparisons of ABO and ONA have yielded conflicting results.[10,12,14,17–21]
Few studies have specifically compared the longevity of botulinum toxin type A (BoNTA) products. One study compared the duration of effect of ABO and ONA using changes in glabellar line severity at maximum contraction as their endpoint and reported ONA had a longer duration of effect than ABO[22]; however, a subsequent study by the same investigators using the same dosing ratio of ABO and ONA reported no difference in the longevity of these products.[23] The results of a split-face study demonstrated ABO was superior to ONA after 30 days for the treatment of lateral orbital rhytids.[24]
The Frontalis Activity Measurement Standard (FMS) has recently been developed as a method for quantifying onset of action and efficacy of BoNTA. Additionally, refinements in the definitions of onset and efficiency were proposed (see Methods).[25]
Using the FMS and a modified version of the 4-point Frontalis Rating Scale (FRS),26 which rates frontalis rhytids as none (0), mild (2), moderate (3), or severe (3) at maximum elevation and at rest, the authors’ previous 30-day study showed that ABO achieved a significantly earlier initial onset of effect than ONA.[27] Although the proportion of treated frontalis sides demonstrating partial and full efficacy was similar for both products at 30 days, the FMS showed a significantly greater number of frontalis sides treated with ABO achieved complete efficacy (90 vs. 75%). The study also demonstrated that ABO was significantly less painful on injection and that there was no apparent difference in area of efficiency (spread). The current objective of this ongoing study is to measure and compare the duration of effect of ABO and ONA for an additional 180 days using the FRS and FMS.
METHODS
Subjects. The study was conducted at two United States trial sites and enrolled 20 female subjects who were 18 to 65 years of age with severe frontalis lines at maximum elevation. At the time of enrollment, frontalis line severity was established by investigator assessment using a standard 4-point photographic frontalis scale.26 Enrollment criteria required the frontalis to be relatively symmetrical at rest and maximum elevation as evaluated by the FMS.
Exclusion criteria included the following: an inability to significantly lessen the severity of frontalis lines by physically spreading them apart; prior treatment with any form of BoNTA during the past year; augmentation of the frontalis with temporary dermal fillers during the previous year or permanent or semi-permanent dermal fillers at any time; upper eyelid blepharoplasty; recent treatments to the frontalis including ablative skin resurfacing, nonablative treatment for skin dyschromias or skin tightening; retinoid, microdermabrasion, or prescription-strength glycolic acid treatments; allergy or hypersensitivity to BoNTA or any component of the products used in the study; or any concurrent therapy or condition that placed the subject at risk, such as a neuromuscular disorder, or compromised the objectives of the study, such as facial asymmetry or ptosis. Pregnant and nursing women were excluded from the study and women of childbearing potential were required to use a reliable form of contraception throughout the trial.
Botulinum neurotoxin injections. ABO and ONA were reconstituted with 2.4mL and 2.0mL preservative-free normal saline for injection, respectively. Identical volumes of ABO or ONA thus represented a dose ratio of 2.5:1.0. Each subject received 25U of ABO (5U injected into five points) and 10U of ONA (2U injected into five points) on contralateral sides of their frontalis (N=40) using identical injection patterns as previously described.[27] ABO and ONA were randomly administered by a blinded investigator to contralateral sides of each subject’s frontalis using five, 31-gauge, 0.3mL hubless insulin syringes each containing 0.04mL of BoNTA.
Frontalis measurements. Frontalis Rating Scale (FRS). Evaluation of contralateral frontalis rhytids were assessed by a blinded investigator. The FRS is a 4-point ranking of 0 (none), 1 (mild), 2 (moderate), and 3 (severe)28 and is a modified version of a validated 5-point scale for assessing the severity of hyperkinetic frontalis wrinkles.[27]
Frontalis Activity Measurement Standard (FMS). The FMS was developed as a new means for accurately quantifying changes in frontalis muscle activity by measuring the difference between the height of the frontalis at maximum elevation and at rest.[25] Using the same camera settings and lighting conditions, maximum frontalis elevation and frontalis elevation at rest are photographically recorded (Janus Photographic Systems, Enhanced Image Technologies, Charlotte, North Carolina). To ensure the maximal elevation effort of each patient is captured, five photos are taken separated by a one-minute rest period. Standardized photographic imaging software (FotoFinder Systems, Inc., Columbia, Maryland) is used to measure the distances between the central aspect of the base of the pupil and between the medial and lateral canthus in relation to the lower part of the frontalis (top of the eyebrow). The mean distance is then calculated based on these three measurements for the contralateral sides of each frontalis image. Measurements and calculations were performed by a blinded assistant investigator.
Assessments. Assessments for the FRS were made on Days 30, 45, 60, 75, 90, 105, 120, 135, 150, 165, 180, 195, and 210 following treatment by the blinded investigators.
Definitions of efficacy. Using the FRS and FMS method to measure frontalis activity, partial, full, and complete duration efficacy were defined as follows:
• Partial efficacy: ?1-point change in FRS scores (from 3 to 2) or 20-percent change in the difference between frontalis elevation at rest and maximum forehead elevation.
• Full efficacy: ?2-point change in FRS scores (from 3 to 1 or 0) or 33-percent change in the difference between frontalis elevation at rest and maximum forehead elevation.
• Complete efficacy: 3-point change in FRS scores (from 3 to 0) or ?66-percent change in the difference between frontalis elevation at rest and maximum elevation.
Safety. Reported adverse events were recorded and coded using the Medical Dictionary for Regulatory Activities terminology (MedDRA).
Statistical analysis. The variance of mean ABO and ONA scores was analyzed at every time point of the study. Kaplan-Meier analysis was used to compare ABO and ONA duration of action. Statistical significance of the Kaplan-Meier analysis was based on the log rank test. The Mann-Whitney nonparametric test of independent samples was also used in association with the Kaplan-Meier analysis to determine differences between medians among the treatment groups. Differences between medians for FRS and FMS for partial, full, and complete effect were examined. Chi-square analyses were used in this study to examine proportional differences between the treatment groups at each time point in the study. For all analyses, statistical significance was established at the 0.05 level.
Ethics. The protocol used in this study adhered to the Good Clinical Practice guidelines of the International Conference on Harmonization and was approved by the U.S. Institutional Review Board, Miami, Florida. Each enrolled subject provided informed consent before participating in any study-related activities.
RESULTS
Ten subjects were enrolled at each of the two study centers. These 20 subjects had a mean age of 45.1 years (range 19–63 years) and were of Caucasian (N=14) and Hispanic (N=6) race and ethnicity, respectively.
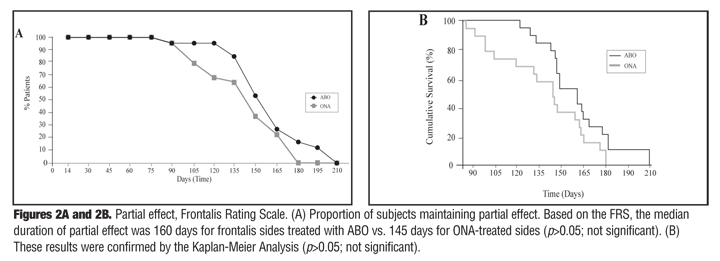
Partial effect. Using the FMS, the median duration of partial effect was 105 days for the sides treated with ABO and 99 days for sides treated with ONA (p=0.02; Figures 1a and 1b). FRS scores showed the median duration of partial effect to be 160 days for the sides treated with ABO and 145 days for ONA-treated sides (p>0.05, not significant; Figures 2a and 2b).
{kind=link}
{kind=link}
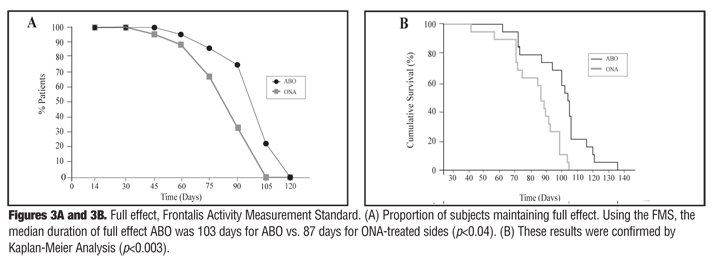
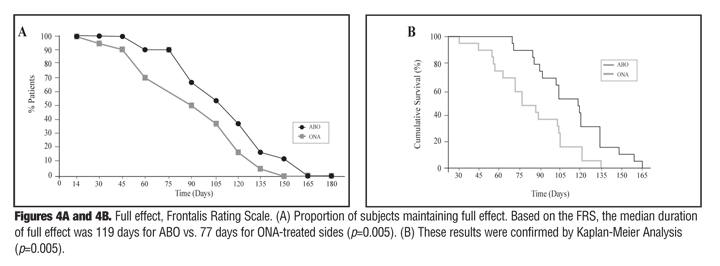
Full effect. The FMS indicated the median duration of full effect for frontalis sides treated with ABO was 103 days compared to 87 days for ONA-treated sides (p<0.04; Figures 3a and 3b). The FRS scores showed the median duration of full effect for frontalis sides treated with ABO was 119 days and 77 days for ONA-treated sides (p=0.005; Figures 4a and 4b).
{kind=link}
{kind=link}
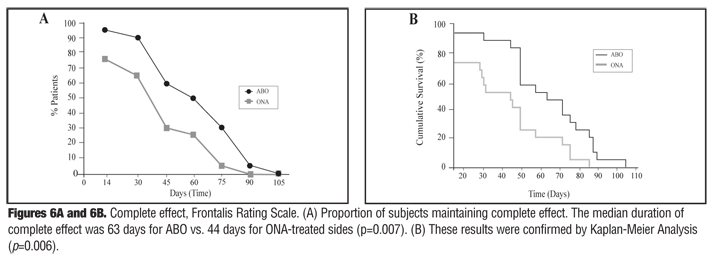
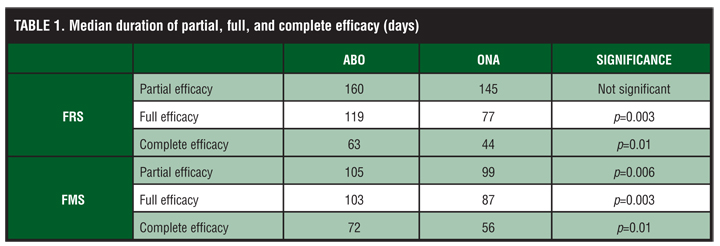
Complete effect. Based on the FMS, the median duration of complete effect for frontalis sides treated with ABO was 72 days and 56 days for ONA-treated sides (p=0.01; Figures 5a and 5b). Using the FRS, the median duration of complete effect for frontalis sides treated with ABO was 63 days compared to 44 days for ONA-treated sides (p=0.007; Figures 6a and 6b). These data are summarized in Table 1. Changes in frontalis height and wrinkle severity for one patient over the entire 210-day study period are shown in Figure 7.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Safety. Reported adverse events included bruising and occasional headache with no significant between-group differences.
DISCUSSION
The results of the initial 30 days of this study using the contralateral frontalis model demonstrated that the onset of effect for ABO occurred significantly earlier than for ONA.[27] Using new definitions for partial, full, and complete efficacy also revealed a greater proportion of ABO-treated frontalis sides achieved these efficacy endpoints compared to ONA. At 30 days post-treatment, the FMS showed 90 percent of the ABO-treated sides maintained complete efficacy versus 75 percent of the ONA-treated sides. In all cases, the FMS appeared to be more sensitive and detected clinical changes earlier than the FRS. Although the results were based on 20 treated subjects, the use of bilateral frontalis comparisons resulted in a statistical N=40.
During the subsequent 180 days, the contralateral frontalis model was able to detect differences in the duration of ABO and ONA activity. Using the FMS, the median duration of partial, full, and complete efficacy was maintained by a significantly higher proportion of frontalis sides treated with ABO. Additionally, the FRS analysis showed significant differences in the median duration of full and complete efficacy.
The FMS was a sensitive indicator of the total duration of BoNTA activity. Using the FMS, the proportion of treated frontalis maintaining partial, full, and complete efficacy reached zero after 135, 135, and 105 days for ABO compared to 105, 105, and 90 days for ONA, respectively. Using the FRS, the proportion of treated frontalis maintaining partial, full, and complete efficacy reached zero after 210, 165, and 105 days for ABO compared to 180, 135, and 90 days for ONA, respectively.
A literature review examined the duration of botulinum toxins for aesthetic applications.[29] Among 35 published articles, only three compared the duration of ABO and ONA. In the first study, patients with moderate or severe glabellar lines at maximum contraction (N=62) were randomly assigned to receive 20U of ONA or 50U of ABO in the glabella,22 which was the same 1:2.5 dosing ration for ONA and ABO used in the authors’ study. Using blinded evaluation of glabellar line severity, 53 percent of ONA-treated patients maintained at least a 1-point improvement after 16 weeks versus 28 percent of ABO-treated patients; however, a weakness of this study is that it compared two groups of patients rather than having each patient serve as her own control as the authors of this study did using the contralateral frontalis model. Consequently, the subjects treated with ONA were older than the ABO group and contained a higher proportion of patients with severe glabellar lines at baseline (52 vs. 45%).22 When these investigators repeated the study using more balanced patient groups, no difference was noted up to 20 weeks after treatment.[23] The same dosing ratio was used, but the total dose of BoNTA was greater in the second study (30 vs. 20U ONA and 50 vs. 75U ABO).
Another randomized, double-blind study also used a split-face model to compare ABO (30U) and ONA (10U) for the treatment of lateral orbital rhytids.24 Comparisons were based on the validated 5-point Merz scale. Although they used a slightly higher 3:1 dose ratio of ABO:ONA, their results are in agreement with the authors’ study and also demonstrated the clinical effects of ABO were significantly better than ONA for the treatment of lateral orbital rhytids after 30 days based on both investigator and patient assessments.
A third group of investigators also used a split-face model to compare BoNTA products for the treatment of periorbital rhytids[30]; however, they compared the efficacy of ONA and a new BoNTA free of complexing proteins (Xeomin®, Merz Pharmaceuticals, Frankfurt, Germany). The blinded evaluator assessment of photographic images at rest and maximum contraction indicated a similar therapeutic response rate for both products over the four-month study based on the 4-point Facial Wrinkle Scale.
The frontalis model and the FMS appear to be a sensitive and objective means for measuring the pharmacodynamic effects of BoNTA including duration of effect. The difference in the duration of clinical activity of the BoNTA products reported here may represent a novel finding. The important distinctions of this study that may account for any differences in results from previously published comparison studies include the use of a contralateral frontalis model, which precludes population group differences; the use of the FMS, which is an objective measure of muscle activity; the use of non-preserved saline with identical injection volumes; and five identical contralateral injection sites. Using the FRS and FMS, the bilateral frontalis model can be utilized to accurately study the clinical properties of BoNTA products and further assess the effects of dose, type, and volume of diluent used and injection patterns.
CONCLUSION
Using a bilateral frontalis model and two distinct evaluation methods, FRS and FMS, ABO was demonstrated to have a longer duration of effect (at a unit to unit ratio of 2.5:1) than ONA based on all definitions of efficacy. The FMS appears to be a sensitive and objective tool for measuring the pharmacodynamic effects of BoNTA including duration of action.
ACKNOWLEDGMENT
The authors acknowledge Dr. Michael Collins for data analysis and Dr. Carl S. Hornfeldt for editorial assistance during the preparation of this manuscript.
References
1. Carruthers J, Lowe N, Menter M, et al. A multicenter, double-blind, randomized, placebo-controlled study of the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J Am Acad Dermatol. 2002;46:840–849.
2. Carruthers J, Lowe N, Menter M, et al. Double-blind, placebo-controlled study of the safety and efficacy of botulinum toxin type A for patients with glabellar lines. Plast Reconstr Surg. 2003;112:1089–1098.
3. Ascher B, Zakine B, Kestemont P, et al. A multicenter, randomized, double-blind, placebo-controlled study of efficacy and safety of 3 doses of botulinum toxin A in the treatment of glabellar lines. J Am Acad Dermatol. 2004;51:223–233.
4. Monheit G, Carruthers A, Brandt F, Rand R. A randomized, double-blind, placebo-controlled study of botulinum toxin type A for the treatment of glabellar lines: determination of optimal dose. Dermatol Surg. 2007;33(Suppl):S51–S59.
5. Brandt F, Swanson N, Baumann L, Huber B. Randomized, placebo-controlled study of a new botulinum toxin type a for treatment of glabellar lines: efficacy and safety. Dermatol Surg. 2009;35:1893–1901.
6. Dysport™ for Injection [package insert]. Scottsdale, AZ: Medicis Aesthetics Inc.; 2009.
7. Botox® Cosmetic for Injection [package insert]. Irvine, CA: Allergan Inc.; 2009.
8. Lietzow M, Gielow E, Le D, Zhang J, Verhagen M. Subunit stoichiometry of the Clostridium botulinum type A neurotoxin complex determined using denaturing capillary electrophoresis. Protein J. 2008;27:420–425.
9. Panjwani N, O’Keeffe R, Pickett A. Biochemical, functional and potency characteristics of type A botulinum toxin in clinical use. Botulinum J. 2008;1:153–166.
10. Wenzel R, Jones D, Borrego J. Comparing two botulinum toxin type A formulations using manufacturers’ product summaries. J Clin Pharm Ther. 2007;32:387–402.
11. Lowe P, Patnaik R, Lowe N. A comparison of two botulinum type A toxin preparations for the treatment of glabellar lines: double-blind, randomized, pilot study. Dermatol Surg. 2005;31: 1651–1654.
12. Hexsel D, Dal’forno T, Hexsel Y, et al. A randomized pilot study comparing the action halos of two commercial preparations of botulinum toxin type A. Dermatol Surg. 2007;34:52–59.
13. Rystedt A, Swartling C, Färnstrand C, Naver H. Equipotent concentrations of Botox and Dysport in the treatment of palmar hyperhidrosis. Acta Derm Venereol. 2008;88:458–461.
14. Karsai S, Adrian R, Hammes S, et al. A randomized double-blind study of the effect of Botox and Dysport/Reloxin on forehead wrinkles and electromyographic activity. Arch Dermatol. 2007;143:1447–1449.
15. Wohlfarth K, Schwandt I, Wegner F, et al. Biological activity of two botulinum toxin type A complexes (Dysport and Botox) in volunteers: a double-blind, randomized, dose-ranging study. J Neurol. 2008;255:1932–1939.
16. Trindade de Almeida A, De Boulle K. Diffusion characteristics of botulinum neurotoxin products and their clinical significance in cosmetic applications. J Cosmet Laser Ther. 2007;9(Suppl 1):17–22.
17. Rosales R, Bigalke H, Dressler D. Pharmacology of botulinum toxin: differences between type A preparations. Eur J Neurol. 2006;13(Suppl 1):2–10.
18. Karsai S, Raulin C. Current evidence on the unit equivalence of different botulinum neurotoxin A formulations and recom-mendations for clinical practice in dermatology. Dermatol Surg. 2009;35:1–8.
19. Klein A, Carruthers A, Fagien S, Lowe N. Comparisons among botulinum toxins: an evidence-based review. Plast Reconstr Surg. 2008;121:413–422e.
20. Hexsel D, Rutowitsch M, DE Castro L, al e. Blind multicenter study of the efficacy and safety of injections of a commercial preparation of botulinum toxin type A reconstituted up to 15 days before injection. Dermatol Surg. 2009;35:933–940.
21. Wohlfarth K, Sycha T, Ranoux D, Naver H, Caird D. Dose equivalence of two commercial preparations of botulinum neurotoxin type A: time for a reassessment? Curr Med Res Opin. 2009;25:1573–1584.
22. Lowe P, Patnaik R, Lowe N. Comparison of two formulations of botulinum toxin type A for the treatment of glabellar lines: a double-blind, randomized study. J Am Acad Dermatol. 2006;55: 975–980.
23. Lowe N, Shah A, Lowe P, Patnaik R. Dosing, efficacy and safety plus the use of computerized photography for botulinum toxins type A for upper facial lines. J Cosmet Laser Ther. 2010;12:106–111.
24. Nettar KD, Yu KC, Bapna S, Boscardin J, Maas CS. An internally controlled, double-blind comparison of the efficacy of onabotulinumtoxinA and abobotulinumtoxinA. Arch Facial Plast Surg. 2011 Jun 20 [Epub ahead of print].
25. Nestor M, Ablon G. The Frontalis Activity Measurement Standard: a novel contralateral method for assessing botulinum neurotoxin type-A activity. J Drugs Dermatol. 2011;10(9);968–972.
26. Carruthers A, Carruthers J, Hardas B, et al. A validated grading scale for forehead lines. Dermatol Surg. 2008;34(Suppl 2): S155–S160.
27. Nestor M, Ablon G. Comparing the clinical attributes of abobotulinumtoxinA and onabotulinumtoxinA utilizing a novel contralateral frontalis model and the Frontalis Activity Measurement Standard. J Drugs Dermatol. 2011;10(10). In press.
28. Carruthers A, Carruthers J. A single-center dose-comparison study of botulinum neurotoxin type A in females with upper facial rhytids: assessing patients’ perception of treatment outcomes. J Drugs Dermatol. 2009;8:924–929.
29. Flynn T. Botulinum toxin: examining duration of effect in facial aesthetic applications. Am J Clin Dermatol. 2010;11:183–199.
30. Prager W, Wissmüller E, Kollhorst B, Williams S, Zschocke I. Comparison of two botulinum toxin type A preparations for treating crow’s feet: a split-face, double-blind, proof-of-concept study. Dermatol Surg. 2010;36(Suppl 4):2155–2160.