J Clin Aesthet Dermatol. 2019;12(11):32–34
 by Bruna Souza Felix Bravo, MD; Julien Totti de Bastos, MD; Camila Roos Mariano de Rocha, MD; Berta Alcala, MD; Stephanie Bianco, MD; Fernando Luis Lopes dos Santos, MD; and Leonardo Goncalves Bravo, MD
by Bruna Souza Felix Bravo, MD; Julien Totti de Bastos, MD; Camila Roos Mariano de Rocha, MD; Berta Alcala, MD; Stephanie Bianco, MD; Fernando Luis Lopes dos Santos, MD; and Leonardo Goncalves Bravo, MD
All authors are with Bravomed Clinic of Dermatology and Plastic Surgery in Rio de Janiero, Brazil.
FUNDING: No funding was provided for this study.
DISCLOSURES: Dr. BSF Bravo is a speaker for Allergan. The other authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: While the injection of botulinum toxin type A (BoNTA) in the neck area, for face contouring through the blockade of the platysmal bundles, and in the mandibular body line has previously been explored, reports of its application for the demarcation of the mandibular angle are more limited. This article described a new technique of BoNTA injection in the mandibular angle for the improvement of contour and definition. At roughly 15 days after application in 30 patients, better visualization of the mandibular angle and its contours was evident and, consequently, smoothing of the appearance of sagging around the mandible with no adverse effects was noted. Further investigation of this technique is warranted.
KEYWORDS: Botulinum toxin, mandible, mandibular angle
Botulinum toxin type A (BoNTA) is a popular aesthetic treatment used for facial rejuvenation and favored for its rapid effects with limited to no downtime.1,2 Commonly applied to the upper third of the face to improve the appearance of wrinkles and expression lines, its use has now extended to the lower third of the face treatment to address perioral lines and platysmal bundles and facilitate facial contour improvement.2–4
Previous reports exist in the literature regarding the use of BoNTA in the neck area, for face contouring through the blockade of the platysmal bundles, and in the mandibular body line; however, little has been mentioned about its application to the demarcation of the mandibular angle. This article aims to describe a new application technique of BoNTA in the angle of the mandible for the improvement of contour and definition.1–7
Methods
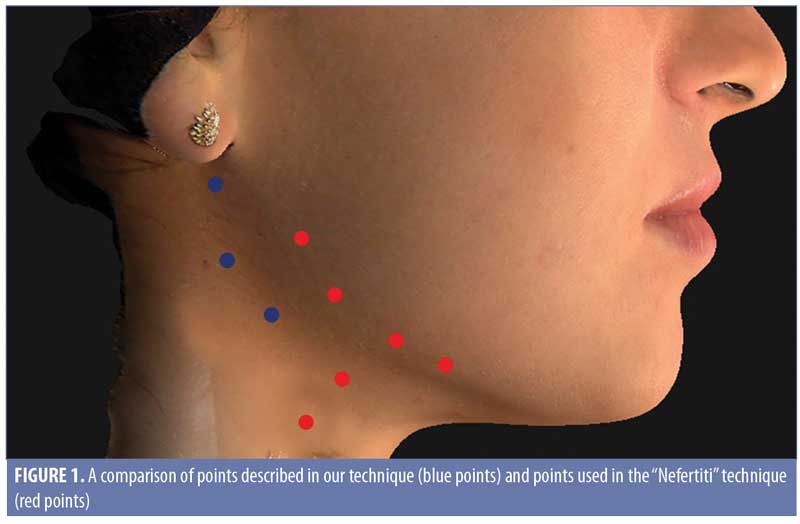
Patients who had an ill-defined jaw angle or who lost this definition during the aging process were eligible for inclusion in this study. A total of 30 patients were selected. All patients provided informed consent and photoconsent, and the study was conducted in accordance with the Declaration of Helsinki. The jaw angle was taken as a spot of reference for marking the points. The first point was marked at a 2-cm distance from the edge of the mandible, toward its angle, while two more points were also selected, one anterior and one superior to the starting point, with a distance of approximately 2-cm in between them (Figure 1). The dilution of the BoNTA used was 100 units for 1mL of 0.9% saline solution, applied with a syringe of 30 units (Becton, Dickinson and Company, Franklin Lakes, New Jersey) and a 30-gauge, 8-mm needle. The lowest dilution sought to facilitate a good safety level and an optimal effect on the platysma muscle, which is a thin muscle. Two to three units of BoNTA (Botox™; Allergan, Dublin, Ireland) were administrated intramuscularly at each described point.
Results
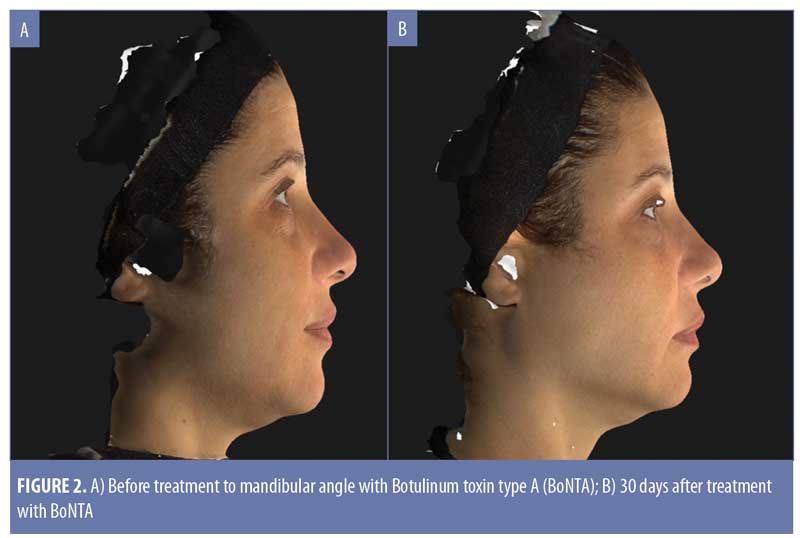
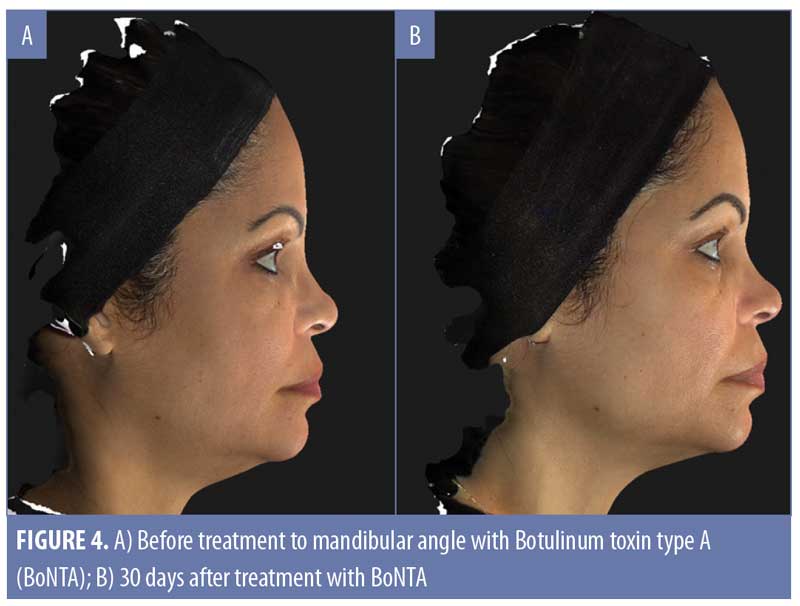
The authors retrospectively reviewed 30 patients who underwent treatment. Approximately 15 days after BoNTA application, increased prominence of the mandibular angle and its contours was evident, with decreased sagging in the same area. Photographic records were made using the VECTRA® H1 three-dimensional imaging system (Canfield Scientific, Parsippany, New Jersey) (Figures 2–4). On average, the duration of the treatment period was around 5 to 6 months. No adverse effects associated with the isolated use of this technique were observed.

Discussion
The aging process of the neck and mandibular region involves the loss of elasticity associated with bone resorption, volume depletion, and sagging, resulting in a loss of contour and definition in the mandible. The platysmal bundles become more prominent due to the loss of skin elasticity and separation of the muscle fibers.2,3
The platysma is a broad, flat muscle covering the anterior and lateral aspects of the neck. It rises from the superficial fascia over the upper chest and ascends superomedially from the neck to insert at the following three points: medially into the mentum, centrally into the periosteum of the ramus of the mandible, and laterally to the orbiularis oris, depressor angulis oris, and risorius muscles overlying subcutaneous tissue. When the upper and lower portions of the platysma contract, they pull the skin to the center of the muscle, forming horizontal lines in the neck.5,6
Currently, botulinum toxin is widely used in the platysmal bundles and was first described in this area by Brandt and Bellman.2 These researchers clinically demonstrated that the application of BoNTA in the platysma reduced the horizontal lines of the neck and improved mandibular contour. The action occurs because it produces an effect opposite to that which is provoked by the platysmal complex. The musculature of this region retracts the lower one-third of the face, erasing the definition of the jaw. With this treatment, there is a release of this downward tension, which relieves the depressing effect of this muscle, providing noninvasive facial rejuvenation.2,3
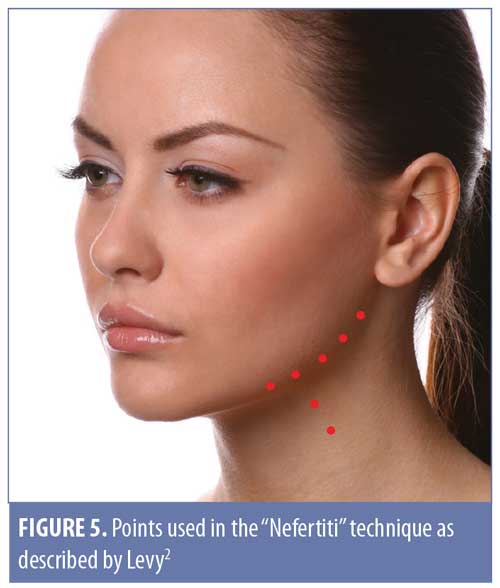
Levy2 described the use of BoNTA to improve the cervical appearance and redefine the contour of the mandible, labeling the technique “Nefertiti” (perfect mandibular contour) (Figure 5). Their results showed a remarkable contouring outcome of the mandible, elevation of the skin in the mandibular line, and elevation of the corners of the mouth; however, its points of application go only to the last lateral platysmal beam, not exceeding this area.
Carruthers et al4 suggested the use of BoNTA in the platysma by applying 1 to 2 units per point along the platysmal horizontal lines for a total of 15 to 20 units per side, in the intradermal plane, emphasizing that pursuing undercorrection is safer so as to avoid adverse effects.4 A microbotox approach (i.e., injection of small amounts of product into a surface plane) can also be used in the lower part of the face, aiming to achieve mandible elevation, improvement of the cervicomental contour, and blockage of the platysma (Figure 6).7

When using BoNTA in the lower one-third of the face, reported unwanted effects, although rare, can include ecchymoses, local discomfort, headache, dysphagia, mild neck weakness, speech disorders, asymmetries, and dry mouth.2,5 Diffusion or injection into the parotid and another salivary gland are not expected, as the application is made posterior to the jaw angle and in the lower portion of the mandible. If, however, an injection occurs in the glands, the likely adverse effect would be a reduction in saliva production. In order to avoid this possible effect, we advise doctors to perform local palpation during the patient’s clinical exam before BoNTA application, in order to elucidate an anomalous presence of salivary glands in this area. If this is observed, we suggest avoiding BoNTA application in this area. Few adverse effects have been reported with total doses of less than 100 units; for this reason, adherence to the use of appropriate doses and superficial application is highly recommended in order to avoid the toxin’s migration to the surrounding tissues.2
Initially, it is important to choose the patient appropriately in order to achieve the planned aesthetic outcome. Patients with an excess of sagging or fat in the mandibular area are not ideal candidates for this technique. There is a classification of sagging created by Carrhuters et al8 that defines a scale for neck volume ranging from Grade 0 (no sagging) to Grade 4 (very severe sagging). Using this scale, patients with sagging up to Grade 2 are expected to benefit from our proposed technique, while those with greater sagging might not notice any improvement.
For patients who desire improved definition of the mandibular contour in addition to that of the mandibular angle, we also applied the toxin to the lower edge of the mandible body using the technique described by Levy.2 With this approach, horizontal injections are made along each mandible and into the upper portion of the posterior platysmal band, resulting in a visible release of the platysma muscle’s downward pulling and thus, jawline recontouring. Patients who qualify for this procedure will show accentuation of the platysmal bands when contracting the platysma. In the technique described before, patients were injected with 2 to 3 units of BoNTA along and under each mandible and to the upper part of the posterior platysmal band, for a total of 15 to 20 units per side.
Conclusion
Previously, the perceived applicability of BoNTA was limited to the treatment of lines and expression marks. However, when its use is expanded to increasing definition of the angle of the mandible and facial contour, it can achieve three-dimensional, dynamic results. Together with the application of BoNTA in the masseter muscle, when this indication exists, the result is a slimming of the lower one-third of the face with a prominent and satisfactory aesthetic result. It is a low-cost and simple application technique with few complications.
In this article, we describe new points of the application of BoNTA for improving the definition of the mandibular angle, which is often diminished by the aging process or the anatomy of some patients. When combined with treatment of the facial and neck contour, a younger, harmonious, and more attractive facial appearance is achieved.
References
- Levy PM. Neurotoxins: current concepts in cosmetic use on the face and neck/jawline contouring/platysma bands/necklace lines. Plast Reconstr Surg. 2015;136(5 Suppl):80S–83S.
- Levy PM. The ‘Nefertiti lift’: a new technique for specific recontouring of the jawline. J Cosmet Laser Ther. 2007;9(4):249–252.
- Kim NH, Chung JH, Park RH, Park J. B The use of botulinum toxin type A in aesthetic mandibular contouring. Plast Reconstr Surg. 2005;115(3): 919–930.
- Carruthers J, Carruthers A. Aesthetic botulinum A toxin in the mid and lower face and neck. Dermatol Surg. 2003;29(5):468–476.
- Hoefflin S. Anatomy of platysma and lip depressor muscles. Dermatol Surg. 1998;24(11):1225–1231.
- de Almeida ART, Romiti A, Carruthers JDA. The facial platysma and its underappreciated role in lower face dynamics and contour. Dermatol Surg. 2017;43(8):1042–1049.
- Wu WT. Microbotox of the lower face and neck: evolution of a personal technique and its clinical effects. Plast Reconstr Surg. 2015;136(5 Suppl):92S–100S.
- Sattler G, Carruthers A, Carruthers J, et al. Validated assessment scale for neck volume. Dermatol Surg. 2012;38(2 Spec No.):343–350.