Claudia Hernandez, MD; Dianne DeLeon, BA
Dr. Hernandez is from University of Illinois at Chicago, Department of Dermatology, Chicago, Illinois; Ms. DeLeon is from University of Illinois at Chicago, College of Medicine, Chicago, Illinois
Disclosure: The authors have no financial or proprietary interest in the subject matter or materials discussed in the manuscript.
Abstract
Pincer nail deformity represents a loss in the normal convex shape of the nail and has been reported in association with various diseases and medications. The authors report a man with end-stage renal disease due to bladder carcinoma who developed pincer nail deformity while on hemodialysis. Previous case reports cite diabetes as a suspected cause of pincer nail development in patients with renal failure. However, the patient described in this case was not diabetic and his nail dystrophy is likely related to arteriovenous fistula placement. (J Clin Aesthet Dermatol. 2011;4(12):43–45.)
A 55-year-old man with end-stage renal disease (ESRD) secondary to obstructive uropathy and bladder cancer presented with progressive nail deformity involving multiple fingers while undergoing hemodialysis. The patient initially presented to the dermatology clinic for nail thickening and scaling of the fingernail folds associated with occasional tenderness. After a one-year follow up, pincer nail deformity (PND) was evident.
His past medical history was significant for hypertension, congestive heart failure, coronary artery disease, chronic obstructive pulmonary disease, gastroesophageal reflux disease (GERD), and hyperparathyroidism. Family history was not significant for any skin or nail disorders. The patient developed ESRD in 1992 from obstructive uropathy when diagnosed with transitional cell carcinoma of the bladder. He underwent cystectomy with ileal conduit that year and started hemodialysis in 1995 after renal function did not improve. Numerous arteriovenous fistulas (AVF) were placed for hemodialysis access due to complications and included the following: 1) right upper extremity AVF failure in 1996, 2) left upper extremity AVF from 1997 to 2001, 3) right upper extremity AVF in 2002 that did not mature, and 4) left axillary AVF in 2002 that underwent pseudoaneurysm repair in 2008. His last fistula thrombosed and was not salvageable necessitating left internal jugular vein catheter placement in 2010. At the time this article was written, the patient was awaiting clearance for a bilateral nephrectomy procedure to reduce the risk of infection and receiving hemodialysis three times per week. His medications included the following: ergocalciferol, darbepoetin alfa, fluticasone nasal spray, lansoprazole, cinacalcet, sevelamer, metoprolol, aspirin, and simvastatin.
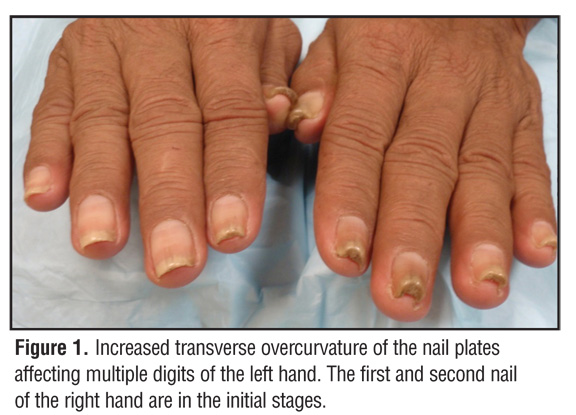
Physical examination was significant for a light yellow discoloration and subungual thickening of several nail plates. There was scaling of the medial and lateral nail folds and increased transverse overcurvature of the distal nail plate, consistent with a pincer nail deformity (Figure 1). These changes, particularly the subungual thickening and nail plate overcurvature, were more severe in the left hand (Figure 2). No pitting of the nail plate was seen. His toenails were thickened bilaterally, but no nail deformity was evident. No palmoplantar keratoderma was appreciated on examination.
{kind=link}
{kind=link}
Potassium hydroxide (KOH) preparation from scale present at nail folds and periodic acid-Schiff (PAS) staining of a nail clipping were negative for hyphae. The patient was offered additional testing including repeat PAS staining and fungal culture of the nail plate, but declined. Etiologies for his nail changes were discussed, including onychomycosis, renal disease, and AV fistulas.
Discussion
PND is characterized predominantly by nail thickening and a transverse overcurvature of the nail plate along its longitudinal axis. The nail edges press deeply into the lateral nail fold, creating a curvature that increases distally along the nail and progressively pinches the nail bed. Pincer nail deformity may be either inherited or acquired.[1] The mechanism of inheritance is still unknown. The etiology and pathogenesis of acquired pincer nail deformity is not yet clear but has been reported in close relation to systemic diseases, such as psoriasis, Kawasaki disease, gastrointestinal malignancies, and systemic lupus erythematosus.[2–5] Other associated conditions include tinea unguium onychomycosis, implantation cyst, and myxoid pseudocyst.[6–8]
Beta-blockers have also been reported as a suspected cause of PND due to the development of pincer nails within six months of treatment and subsequent reversal after the cessation of medication.[9,10] Although the patient in this case was on metoprolol for hypertension, he had been on a stable dose for several years, making it an unlikely cause of his nail changes. Pamidronate is another medication recently reported to be associated with PND development.[11]
Various nail pathologies have been reported to occur in 62 to 86 percent of patients with ESRD undergoing hemodialysis. These abnormalities include pincer nail deformity but more commonly half-and-half nails, absence of lunula, onycholysis, and splinter hemorrhages (Table 1).[12–14] Pincer nails are also a recognized iatrogenic complication of AVF placement used for hemodialysis access. The pathogenesis of this process involves the development of pseudo-Kaposi sarcoma and venous hypertension, resulting in a circulatory disturbance of the microvasculature. Ultimately, this leads to tissue hypoxia in the five digits distal to the AVF. Hwang et al[15] reported the gradual resolution of PND after fistula ligation, which further supports the causal relationship between AVFs and this nail deformity. Of note, our patient’s nail deformities were more advanced on his left side, which correlates with the side of his body with longer functioning AVFs. Kirkland et al[16] reported the first case of acquired PND associated with ESRD in a patient who had not yet undergone hemodialysis. The report advocates the possibility of diabetes and renal disease contributing to microvascular damage in the nail bed. Since ESRD in our patient was secondary to obstructive uropathy from bladder cancer, rather than diabetes, these microvasculature complications were not implicated in his nail abnormalities. Additionally, the development of PND occurred after a 15-year history of ESRD and the time course of nail changes was not associated with any deterioration in renal function.
{kind=link}
Conclusion
The occurrence of PND is quite rare and more reports of its occurrence in patients with chronic renal failure due to obstructive uropathy may clarify the pathogenesis of nail changes in this patient population. Thorough physical and laboratory examinations and comprehensive documentation of medical histories will be fundamental in the establishment of the etiologic factors of PND.
References
1. Baran R, Haneke E, Richert B. Pincer nails: definition and surgical treatment. Dermatol Surg. 2001;27(3):261–266.
2. Baran R. Letter: pincer and trumpet nails. Arch Dermatol. 1974;110(4):639–640.
3. Vanderhooft SL, Vanderhooft JE. Pincer nail deformity after Kawasaki’s disease. J Am Acad Dermatol. 1999;41(2 Pt 2):341–342.
4. Jemec GB, Thomsen K. Pincer nails and alopecia as markers of gastrointestinal malignancy. J Dermatol. 1997;24(7): 479–481.
5. Majeski C, Ritchie B, Giuffre M, Lauzon G. Pincer nail deformity associated with systemic lupus erythematosus. J Cutan Med Surg. 2005;9(1):2–5.
6. Higashi N. Pincer nail due to tinea unguium. Hifu. 1990;32:40–44.
7. Su YT, Lee JYY. Pincer nail deformity associated with an arteriovenous fistula for hemodialysis. Dermatologica Sinica. 2010;28(2):87–88.
8. Baran R, Broutart JC. Epidermoid cyst of the thumb presenting as pincer nail. J Am Acad Dermatol. 1988;19(1 Pt 1):143–144.
9. Bostanci S, Ekmekci P, Akyol A, et al. Pincer nail deformity: inherited and caused by a beta-blocker. Int J Dermatol. 2004;43(4):31.
10. Greiner D, Schöfer H, Milbradt R. Reversible transverse overcurvature of the nails (pincer nails) after treatment with a beta-blocker. J Am Acad Dermatol. 1998;39(3):486–487.
11. Failla V, Richert BJ, Nikkels AF. Pincer nails associated with pamidronate. Clin Exp Dermatol. 2011;36(3):305–306.
12. Dyachenko P, Monselise A, Shustak A, et al. Nail disorders in patients with chronic renal failure and undergoing haemodialysis treatment: a case-control study. J Eur Acad Dermatol Venereol. 2007;21(3):340–344.
13. Salem A, Al Mokadem S, Attwa E, et al. Nail changes in chronic renal failure patients under haemodialysis. J Eur Acad Dermatol Venereol. 2008;22(11):1326–1331.
14. Martinez MA, Gregório CL, Santos VP, et al. Nail disorders in patients with chronic renal failure undergoing hemodialysis. An Bras Dermatol. 2010;85(3):318–323.
15. Hwang SM, Lee SH, Ahn SK. Pincer nail deformity and pseudo-Kaposi’s sarcoma: complications of an artificial arteriovenous fistula for haemodialysis. Br J Dermatol. 1999;141(6):1129–1132.
16. Kirkland CR, Sheth P. Acquired pincer nail deformity associated with end stage renal disease secondary to diabetes. Dermatol Online J. 2009;15(4):17.