Physical Modalities for Acne, Rosacea, and their Sequelae
Section Editor: Emmy M. Graber, MD
This month’s installment by Emily M. Wise, MD; Emmy M. Graber, MD
Dr. Graber is Assistant Professor, Department of Dermatology, Boston University, Boston, Massachusetts. Dr. Wise is Resident in Dermatology, Boston University School of Medicine, Department of Dermatology, Boston, Massachusetts. Disclosure: Drs. Graber and Wise report no relevant conflicts of interest.
Abstract
In the past, the safety of performing procedures while patients are on isotretinoin has been questioned. Macrocomedones are traditionally resistant to treatment with isotretinoin alone. The authors present a technique that is safe to employ while patients are on isotretinoin to effectively eliminate macrocomedones without complication.
Introduction
Despite decades of research that have yielded a large arsenal of both pharmacological and physical treatment modalities, the management of acne vulgaris remains a challenge for patients and physicians alike. Isotretinoin (13-cis-retinoic acid) has been a mainstay of therapy in the United States for severe nodulocystic or recalcitrant scarring acne for nearly three decades. Isotretinoin possesses the unique ability to target all four steps responsible for acne pathogenesis: inflammation, abnormal keratinization, colonization with Propionibacterium acnes, and sebum production.[1] For patients with macrocomedonal lesions (defined as comedones greater than 1mm), treatment may be even more difficult, as these patients are at greater risk for flares both with initiation of isotretinoin as well as after completion of a full course of therapy.[2–4] Many studies suggest that macrocomedonal extraction prior to beginning isotretinoin may prevent severe flares during the initiation phase of isotretinoin; however, little has been reported on extraction techniques concurrently while on isotretinoin therapy.
One approach to patients with macrocomedonal lesions that are either slow to respond to isotretinoin or are simply recalcitrant to isotretinoin therapy is to mechanically extract the lesions using a comedone extractor during the patient’s routine isotretinoin maintenance visits. Adjunctive procedures used for acne treatment while on isotretinoin have historically been avoided, as there have been reports in the literature describing keloid formation following both dermabrasion and laser treatments.[5,6] Here, the authors report performing a series of mechanical macrocomedonal extractions on a patient while concurrently on isotretinoin that resulted in resolution of the lesions with no residual scarring. Because macrocomedones can be both aesthetically and psychologically displeasing, treatment of these lesions while on isotretinoin may be paramount in achieving more complete acne clearance, thus optimizing patient satisfaction.
Technique
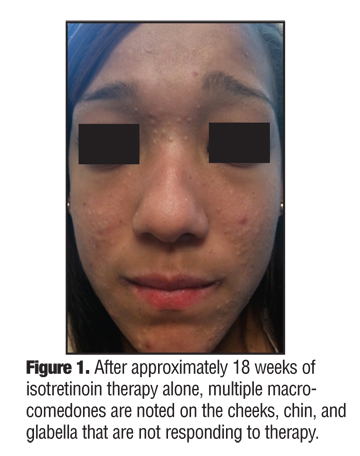
The authors report a case of a 20-year-old woman with acne characterized by inflammatory lesions and macrocomedones. Recalcitrant to numerous oral and topical acne regimens, she was started on isotretinoin therapy with a goal dose of 7,000mg (125mg/kg at 56kg). After approximately three months of therapy, while she noticed marked improvement in many of her inflammatory lesions, she had multiple residual macrocomedones that were cosmetically displeasing and persistent despite her medical therapy (Figure 1). While continuing on the isotretinoin, the authors performed a series of in-office manual extractions of her macrocomedones that resulted in dramatic improvement of the lesions without residual scarring (Figure 2).
{kind=link}
{kind=link}
Manual extraction of comedonal lesions has been well-described in the literature, but the utility of using it as adjuvant therapy while on isotretinoin has, to our knowledge, not been described. The technique is safely and easily performed and should not leave residual scarring if executed correctly. The lesions should be prepped with alcohol and a tiny prick incision should be made using a beveled large-bore needle or sharp surgical blade, lightly piercing the epidermis. Light-to-medium pressure should be applied directly atop the lesion with a comedone extractor until all of the contents have been expressed. While the patient may experience minor discomfort secondary to pressure, complaints of pain should prompt the physician to reevaluate the technique. The patient should, as per usual, be counseled about sun avoidance and protection methods as well as the importance of avoiding any further digital manipulation of the lesions. Other risks to consider include incomplete extraction and comedone recurrence.[7]
Discussion
The manual extraction of macrocomedones is a simple in-office procedure that can be performed without residual scarring during a patient’s isotretinoin course. Physicians should not hesitate to use this age-old technique in the right patient population, namely those with recalcitrant macrocomedones or those with macrocomedones that are slow to resolve on isotretinoin alone.
Other methods that have been documented to be beneficial for treatment of comedones include fulguration and electrocautery with an epilating needle, with one study suggesting that electrocautery is better for large closed comedones than fulguration.[8] Another study specifically evaluated the usefulness of light cautery in the treatment of large (greater than 3mm) comedones and reported satisfactory cosmetic results.[2] These methods, unlike simple comedone extraction, can be painful and less well tolerated.
The results described in this report made a significant impact on the cosmetic appearance of the authors’ patient in addition to the improvement in her overall psychological state. This procedure was performed during multiple routine isotretinoin maintenance visits and with each visit, the patient was evaluated for residual scarring and recurrent lesions and was asked about subjective satisfaction with the procedure. Overall, the authors feel that this procedure is an easy and reliable method to help patients achieve more rapid and satisfactory acne clearance and can be safely performed while a patient is concurrently on isotretinoin.
References
1. Layton AM, Knaggs H, Taylor J, et al. Isotretinoin for acne vulgaris: 10 years later—a safe and successful treatment. Br J Dermatol. 1993;129:292–296.
2. Kava TI, Tursen U, Kokturk A, Ikizoglu G. An effective extraction technique for the treatment of closed macrocomedones. Dermatol Surg. 2003;29(7):741–744.
3. Demircay Z, Kus S, Sur H. Predictive factors for acne flare during isotretinoin treatment. Eur J Dermatol. 2008;18(4):452–456.
4. Bottomley WW, Culiffe WJ. Severe flares of acne following isotretinoin: large closed comedones (macrocomedones) are a risk factor. Acta Derm Venereol. 1993;73(1):74.
5. Rubenstein R, Roenigk HH Jr, Stegman SJ, Hanke CW. Atypical keloids after dermabrasion of patients taking isotretinoin. J Am Acad Dermatol. 1986;15(2 Pt 1):280–285.
6. Zachariae H. Delayed wound healing and keloid formation following argon laser treatment or dermabrasion during isotretinoin treatment. Br J Dermatol. 1988;118(5):703–706.
7. Taub AF. Procedural treatments for acne vulgaris. Dermatol Surg. 2007;33(9):1005–1026.
8. Bottomley WW, Yip J, Knaggs H, Cunliffe WJ. Treatment of closed comedones—comparisons of fulguration with topical tretinoin and electrocautery with fulguration. Dermatology. 1993;186(4):253–257. `