Rishi Kumar Gandhi, MD, Department of Dermatology, Wright State University Boonshoft School of Medicine, Dayton, Ohio; Jacquelyn Coloe, MD, Department of Dermatology, University of Miami Miller School of Medicine, Miami, Florida; Sara Peters, MD, Division of Dermatopathology, The Ohio State University, Columbus, Ohio; Matthew Zirwas, Division of Dermatology, The Ohio State University, Columbus, Ohio; Kamruz Darabi, MD, Division of Dermatopathology, The Ohio State University, Columbus, Ohio
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Objective: To report a case of Wells syndrome (eosinophilic cellulitis) in a patient who was previously hospitalized twice and received several antibiotic treatments. Setting: Inpatient hospital consultation. Participant: One patient diagnosed with Wells Syndrome based on supporting clinical history, histopathological examination, and other laboratory data. Measurement: Change in signs and symptoms over time. Results: Improvement of skin lesions after administration of corticosteroids. Conclusion: Wells syndrome is a clinical condition that mimics bacterial cellulitis. It is characterized as an erythematous, edematous tender plaque with predilection for the lower extremity. The authors report this case to warn clinicians about other primary dermatological disorders that resemble infectious cellulitis in order to avoid misdiagnoses and delayed treatment. (J Clin Aesthet Dermatol. 2011;4(7):55–57.)
Wells syndrome, also known as eosinophilic cellulitis, is a rare condition that was first described in 1971 as a “recurrent granulomatous dermatitis with eosinophilia.”[1] Approximately 80 cases have been reported internationally.[2] The pathophysiology is unknown; however, many regard this disease as a hypersensitivity reaction arising from a variety of allergic stimuli or arthropod reactions.[3] Clinically, it presents as a tender, pruritic, edematous cellulitis-like eruption.Here, the authors present a case of Wells syndrome that was successfully treated with corticosteroids after no therapeutic response to antibiotics and inpatient hospitalizations.
Case Report
A 50-year-old Caucasian man with a history of chronic hepatitis C virus infection (HCV) presented to the hospital three weeks after noticing redness and pain on his left medial ankle in association with low-grade temperatures and chills. Prior to presentation, he had been treated with ciprofloxacin and cephalexin with no changes in his lower extremity. The patient had similar, milder prior episodes involving his hands and forearms that subsided without treatment. A wound culture showed pan-susceptible Streptococcus pyogenes. He was admitted to the hospital, received three days of intravenous vancomyocin, and was discharged home with a 10-day course of trimethoprim-sulfamethoxazole. Despite initial improvement for three weeks, his extremity showed reoccurrence of redness, swelling, and pain (Figure 1). He was restarted on oral trimethoprim-sulfamethoxazole for a few days as an outpatient with no improvement. His skin lesions continued to worsen with fever, and he was subsequently admitted to the hospital and restarted on vancomyocin. After minimal response to several systemic and topical regimens, other tests were performed. He underwent magnetic resonance imaging (MRI) for suspicion of osteomyelitis. An ultrasound duplex and magnetic resonance venography (MRV) were performed to search for deep vein thrombosis (DVT) and venous incompetence. A computed tomography (CT) scan was ordered to locate possible abscess. His entire imaging evaluation was negative and excluded these disorders. Bacterial, fungal cultures, and human immunodeficiency virus (HIV) tests were all negative. The entire laboratory evaluation was unremarkable, except for peripheral eosinophilia that increased from 5.3 to 11 percent during his acute flareup.
{kind=link}
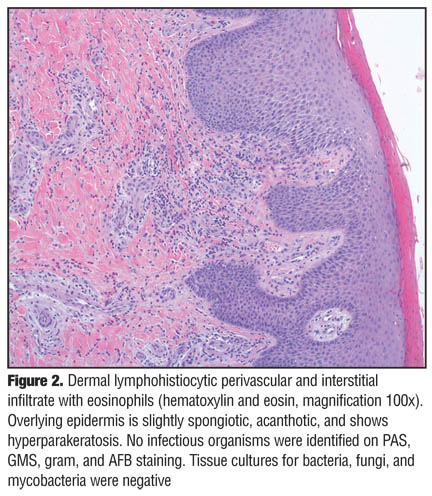
A skin biopsy showed superficial and deep perivascular chronic inflammatory infiltrate admixed with eosinophils (Figure 2 and Figure 3). No histopathological evidence of nodular lymphocytic infiltration or vasculitis was present. A direct immune fluorescence (DIF) examination was negative. Although no discernable “flame figures” were identified, he was given the diagnosis of Wells syndrome. He began a six-week prednisone taper. At the conclusion of therapy, edema and pain resolved with mild residual blanching erythema.
{kind=link}
{kind=link}
DISCUSSION
This case demonstrates that Wells syndrome merits stronger consider-ation in the setting where bacterial cellulitis does not respond to antibiotics. Consideration of this diagnosis may have avoided costly imaging studies, inpatient hospitalization, and adverse side effects from broad-spectrum anti-biotics. The authors discuss different derma-tological disorders that present similar to those described in this case and represent diagnostic challenges.
Infectious cellulitis is usually the first suspicion in a patient such as the one presented in this case. A tiny break in the skin barrier allows bacteria to enter the skin and cause infection. The source of inoculation can be from a number of causes, but some risk factors include small fissures between the toes from a fungal infection, diabetic ulcers, peripheral vascular disease, or any kind of insect bite.[4] The area is typically glossy and shiny with sharp demarcations, usually on a limb, though other areas of the body can be affected. Bacterial or fungal cellulitis also rapidly expands within the first 24 hours as opposed to noninfectious causes. Patients may also experience systemic signs of cellulitis, such as fever, chills, malaise, and myalgia. Immunocompetency of the patient should be assessed when considering fungal cellulitis. Cryptococcal cellulitis can present strikingly similar to bacterial cellulitis, and a high index of suspicion should be maintained, especially in immunosuppressed patients.[5] Given the patient’s history of chronic HCV infection, cryoglobulinemia, cryofibrinogenemia, and leukocytoclastic vasculitis were also considered. These diseases typically consist of purpuric skin lesions, which were not seen in this patient.[6]
Allergic contact dermatitis and irritant contact dermatitis also mimic cellulitis. In both cellulitis and contact dermatitis, one can see erythema, blistering, or crusts. However, the main symptom of cellulitis is pain, while allergic contact dermatitis exhibits pruritus. Irritant contact dermatitis commonly causes burning pain and pruritus is not severe. Both irritant and allergic contact dermatitis will appear in a distribution that is related to the allergen or irritant, for instance, at the application site of a topical medication.[7] The authors attribute the epidermal changes in the biopsy from the dorsal foot to the protracted course with application of multiple antiseptics and compression dressings over weeks. This may have resulted in a superimposed irritant contact dermatitis picture histologically. Although contact dermatitis and fungal infection cannot be excluded in this case, the lack of pruritus and grossly visible scaling argue against allergic contact dermatitis. Negative fungal tissue culture and fungal stains make fungal infection a less probable source. The lack of immune-globulin and complement deposition on direct immunofluorescence argue against precursor lesions of immunobullous disorders, such as bullous pemphigoid. The local presentation to one leg and lack of frank bullae argues against the latter as well.
Venous thrombophlebitis, DVT, or stasis dermatitis can also resemble cellulitis. Features of stasis dermatitis are mottled brown dyspigmentation of the lower leg, varicose veins, and pitting edema. In advanced cases of chronic stasis due to venous insufficiency leading to lipodermatosclerosis, one may observe an “inverted champagne bottle,” appearance of the lower leg.[8] The histopathological features of stasis dermatitis are spongiosis, dilated dermal vessels, extravasation of red blood cells, and dermal hemosiderin deposition with cannonball angioplasia in the superficial dermis.[9] These features were not seen in the biopsy of this case. In addition, the patient failed to respond to elevation and compression making this diagnosis less likely.
Other more superficial infections of the skin can also be included in the differential. Simple impetigo or candidiasis can exhibit the same erythema, although on palpation, the skin does not feel as edematous or inflamed as cellulitis. Additionally, candidiasis should exhibit some scaling of the skin that is not seen in cellulitis, and oftentimes in the vicinity of the large erythematous plaque, smaller satellite lesions can be seen. Impetigo typically exhibits a “honey-colored crust,” on the surface of erythematous plaques and patches.
Wells syndrome (eosinophilic cellulitis) is an acute, recurrent, pruritic dermatitis that is often described as a cellulitis-like eruption with edema and eosinophils present in the dermis. Less common but reported presentations also include nodules, vesicles, bullae, and urticaria.10–12 Histo-pathological findings involve an acute stage, subacute stage, and resolving stage. In the acute stage, dermal edema and an eosinophilic infiltrate are seen in the upper and deep dermis. In the subacute stage, “flame figures” have a distinct appearance and represent intense eosinophilic degranulation of major basic protein coating collagen bundles in the dermis. These flame figures are not specific to eosinophilic cellulitis and occur in other conditions, such as bullous pemphigoid, tinea pedis, or insect bite reactions. In the resolving stage, phagocytic histiocytes palisade around the flame figures, and a granuloma may form in an attempt to eliminate the flame figures.[13] The histological pattern of the resolving stage needs to be kept in mind when deciding whether to deal with late-stage eosinophilic cellulitis or deep fungal or mycobacterial infections. Deeper sections through the specimen may reveal flame figures or micro-organisms on special stains. However, since flame figures are not specific for eosinophilic cellulitis and micro-organism stains have very low sensitivity, the gold standard to rule out fungal or mycobacterial cellulitis is tissue culture.
Previous reports postulate that eosinophilic cellulitis may be a result of a hypersensitivity reaction to an arthropod bite or bee sting.[14,15] Other identified causes include drugs, various infections, Churg-Strauss syndrome, or overlap with hypereosinophilic syndrome.[16] The lesions usually heal without scarring over 2 to 8 weeks; however, reoccurrence is common. Systemic corticosteroids are the most effective treatment and can be safely administered for short periods of a few weeks and can be repeated when reoccurrence happens.
This case emphasizes the need to understand uncommon and common dermatological disorders that cause a cellulitis-like eruption. Initially, clinicians should perform appropriate diagnostic work up directed by history and physical examination. Selection of additional tests or therapy should avoid harm to the patient and not exacerbate existing skin disease. Vigilance to the different disorders discussed here will help guide further management and patient care.
References
1. Wells GC. Recurrent granulomatous dermatitis with eosinophilia. Trans St Johns Hosp Dermal Soc. 1971;57:46–56.
2. “Wells syndrome” June 2010. http://emedicine.medscape.com/ article/1124844-overview Accessed on March 12, 2011.
3. Melski JW. Wells’ syndrome, insect bites, and eosinophils. Dermatol Clin. 1990;8(2):287–293.
4. Swartz MN. Cellulitis: clinical practice. N Engl J Med. 2004; 350:904–912.
5. Anderson DJ, Schmidt C, Goodman J, et al. Cryptococcal disease presenting as cellulitis. Clin Infect Dis. 1992;14(3) 666–672.
6. Chen KR, Carlson JA. Clinical approach to cutaneous vasculitis. Am J Clin Dermatol. 2008;9(2):71–92.
7. Belsito DV. Occupational contact dermatitis: etiology, prevalence, and resultant impairment/disability. J Am Acad Dermatol. 2005; 53(2):303–313.
8. Wollinsky CD, Waldorf H. Chronic venous disease. Med Clin North Am. 2009;93(6):1333–1346.
9. “Stasis Dermatitis” February 2007. http://www.emedicine.com/ derm/TOPIC403.HTM Accessed on March 12, 2011.
10. Odia SG, Purschel W, Worret WI, et al. Hypereosinophilic cellulitis (Wells’ syndrome) resembling urticarial. Acta Derm Venerol (Ljubljana). 1994;6:193–195.
11. Home SA, McHenry P. Nodular presenentation of eosinophilic cellulitis (Wells’ syndrome). Clin Exp Dermatol. 2001; 26(8): 677–679.
12. Ferreli C, Pinna AL, Atzori L, et al. Eosinophilic cellulitis (Wells’ syndrome): a new case description. J Eur Acad Dermatol Venereol. 1999;13(1):41–45.
13. Moosavi M, Mehregan DR. Wells’ syndrome: a clinical and histopathologic review of seven cases. Int J Dermatol. 2003; 42(1):62–67.
14. Lin HL, Lin JN, Chen CW. Eosinophilic cellulitis after honeybee sting. J Formos Med Assoc. 2009;108(12): 964–966.
15. Schorr WF, Tauscheck Al, Dickson KB, et al. Eosinophilic cellulitis (Wells’ syndrome): histologic and clinical features in arthropod bite reactions. J Am Acad Dermatol. 1984; 11(6): 1043–1049.