James Q. Del Rosso, DO; Julie Harper, MD; Radhakrishnan Pillai, PhD; Robert Moore, PhD
Dr. Del Rosso is Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada; Dr. Harper is Clinical Associate Professor of Dermatology, University of Alabama, Birmingham, Alabama; Dr. Pillai is Director Project Management, Dow Pharmaceutical Sciences, Petaluma, California; Dr. Moore is Associate Principal Scientist, Dow Pharmaceutical Sciences, Petaluma, California
Disclosure: Dr. Del Rosso is a consultant, speaker, and/or researcher for Coria/Valeant, Allergan, Galderma, Graceway, Intendis, Medicis, Onset Dermatologics, Obagi Medical Products, Ortho Dermatologics, PharmaDerm/Nycomed, Promius, Ranbaxy, Stiefel/GSK, TriaBeauty, Triax, Unilever, and Warner-Chilcott. Dr. Del Rosso did not receive compensation for authoring this article. Dr. Harper reports no relevant conflicts of interest. Drs. Pillai and Moore are employees of Dow Pharmaceutical Sciences, developers of micronized tretinoin (0.05%) gel.
Abstract
Background: Various formulations of tretinoin (gel, liquid, cream) have been reported to be unstable on the skin under bright artificial light or sunlight. This photodegradation can potentially influence treatment regimens and possibly modify efficacy. The maximum light energy absorption of tretinoin is in the ultraviolet A region. Objective: To compare the photostability of a micronized formulation of tretinoin (0.05%) aqueos gel with tretinoin (0.025%) gel following exposure to ultraviolet A light for eight hours. Methods: Micronized tretinoin (0.05%) gel and tretinoin (0.025%) gel were then exposed to ultraviolet A light with an integrated intensity from 315 to 400nm of 22watt/m2. Samples of both products were prepared and analyzed for tretinoin and its degradation products using a high-performance liquid chromatography method. Additional duplicate samples were similarly prepared and analyzed after 2,4,6, and 8 hours. Results: There was a nine-percent degradation of micronized tretinoin in the 0.05% aqueous gel compared to 72-percent degradation of tretinoin in the 0.025% gel following eight-hour ultraviolet A light exposure. The small increase in tretinoin degradation products with micronized tretinoin (0.05%) aqueous gel remained below six percent of the labeled concentration compared to a marked increase in tretinoin degradation products with tretinoin 0.025% gel at two hours that increased to over 66-percent labeled concentration at eight hours. Conclusion: Micronized tretinoin (0.05%) aqueous gel showed less than 10-percent degradation when exposed to eight hours of ultraviolet A light, while tretinoin (0.025%) gel showed significant tretinoin degradation. (J Clin Aesthet Dermatol. 2012;5(1):27–29.)
Tretinoin is a widely used retinoid in the topical treatment of various dermatological diseases, especially acne and photoaging. In the management of acne, tretinoin exhibits several modes of action that lead to a reduction in comedones, microcomedones, and inflammatory lesions. A common approach to acne care is the application of a topical retinoid at night. This bedtime application has been preferred with tretinoin as it is light sensitive.[1]
Vehicle formulation has been shown to impact the photostability of tretinoin. Investigation into the photodegradation of tretinoin in creams prepared with various oils revealed that tretinoin is far more stable in the cream formulations than in the respective oils alone. However, in this study it was not clear whether this was due to the formulation or due to a different irradiation technique.[2] In addition, combination therapy in acne is commonplace as multiple medications are used to target as many points in the pathogenesis of the disease as possible. The ability for a patient to apply the recommended topical therapies in a single “application session,” with the time of day determined by the patient, provides convenience that can often translate into better long-term adherence with therapy.[3]
New formulations continue to be developed that might minimize photodegradation. An in-vitro light stability study compared a simple gel and microsphere-based formulation containing tretinoin. Under ambient (fluorescent) light, incandescent light, or darkness, tretinoin decomposed. The microsphere gel tretinoin preparation was found to be more stable in the presence of light than the conventional gel.[4] After 24 hours of exposure to fluorescent light, 98 percent of the initial tretinoin in the microsphere (0.1%) gel formulation remained unchanged in contrast to a 69-percent degradation of tretinoin in the conventional (0.025%) gel.[4] This significant degradation of tretinoin in the 0.025% gel had been reported in earlier studies and is clinically significant given the initial low dose of tretinoin.[5] A more recent study by the same group reported 84 percent of the initial tretinoin in the microsphere (0.1%) gel remained unchanged following six hours of simulated solar ultraviolet (UV) irradiation compared to only 10 percent with tretinoin gel (0.025%), suggesting that photostability might be related to the light conditions. It has been suggested that the stability under the irradiation by a different light source or daylight was predictable if the total irradiation intensity per second could be measured under that condition.[6–8] Studies have demonstrated that the UVA component of light is a major contributor to the photodegradation of tretinoin, and, in some cases, the wavelength of 420nm has been implicated.[9,10]
A micronized aqueous gel formulation of tretinoin (0.05%) gel has recently become available. Clinical studies have shown significantly (P<0.001) improved cutaneous tolerability over tretinoin microsphere (0.1%) gel, especially over the first few weeks of therapy and comparable efficacy.[11,12] However, the potential for photodegradation of the micronized formulation of tretinoin aqueous gel (0.05%) has not been previously studied. This study compares the photodegradation of micronized tretinoin (0.05%) aqueous gel with tretinoin (0.025%) gel by UVA light.
METHODS
Micronized tretinoin aqueous gel (0.05%, Atralin® Gel, Coria Laboratories) and tretinoin (0.025%) gel were exposed to UVA light with an integrated intensity from 315 to 400nm of 22 watt/m2. This spectral region was selected to provide a more energetic exposure than visible light and is consistent with the International Conference on Harmonization (ICH) guidelines for photostability testing.
Equal amounts of each gel were placed in clear polypropylene syringes and exposed to UVA light. Duplicate 2g samples were delivered into individual 50mL volumetric flasks and dissolved in 25mL of phosphate buffer (pH 3.0). Each flask was filled to volume with tetrahydrofuran. A portion of each sample solution was filtered through a 0.45µm polyvinylidene fluoride filter and assayed by high-performance liquid chromatography (HPLC) immediately after preparation. Additional duplicate samples were similarly prepared and analyzed after 2, 4, 6, and 8 hours of exposure to UVA light. Each sample was analyzed for tretinoin based on percentage of labeled concentration (%LC) and degradation product content.
RESULTS
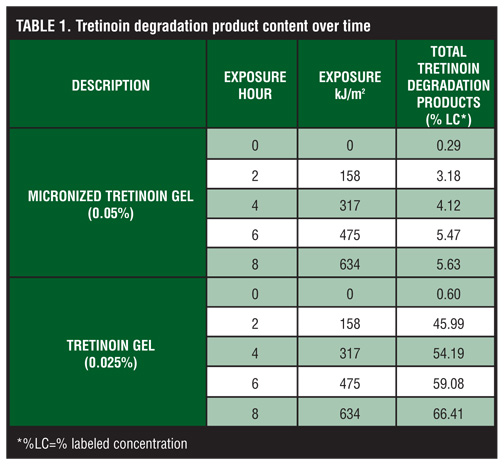
When exposed to UVA light for eight hours, there was a nine-percent degradation of micronized tretinoin in the (0.05%) aqueous gel as compared to a 72-percent degradation of tretinoin in the (0.025%) gel (Figure 1). Although there was a small increase in tretinoin degradation products with micronized tretinoin (0.05%) aqueous gel, this remained below the six percent of LC at all time points (Table 1). There was a marked increase in tretinoin degradation products with tretinoin (0.025%) gel at two hours, and this continued to increase to over 66 percent of LC at eight hours.
{kind=link}
{kind=link}
DISCUSSION
Photodegradation of tretinoin has been reported previously.[4,5] It appears to correlate with specific light conditions and vehicle formulation[.7–9] The degradation results seen with tretinoin (0.025%) gel in this study may be relevant clinically due to the magnitude of degradation, and the results are consistent with those reported by other investigators.[4–6]
New formulations of tretinoin have been developed to potentially reduce the impact of photodegradation and have been studied under a variety of light conditions. For example, tretinoin microsphere (0.1%) gel showed minimal (<3%) degradation following exposure to fluorescent or incandescent light over 24 hours, but more degradation (16%) following exposure to simulated solar UV irradiation over six hours[.4,6]
UVA is an important component of UV solar radiation and its impact is related to geography, altitude, time of year and day, weather conditions, and reflection. It penetrates deeper than UVB light into the skin due to its longer wavelength and can interact with both epidermal and dermal cells.[13] It does not cause burning unless the skin is photosensitive or excessive doses are used. UVA penetrates glass so windows do not offer protection. Indoor solar UVA irradiances represent about 25 percent of the outdoor irradiances and are about 60 times greater than fluorescent light irradiances.[14]
In this study, UVA light (spectral range 315–400nm) was chosen because studies have demonstrated that the UVA component of light is a major contributor to the photodegradation of tretinoin and to be consistent with components of the ICH guidelines for photostability testing.[9] Under these conditions, photodegradation of a micronized aqueous gel formulation of tretinoin (0.05%) was minimal after eight hours. The nine-percent degradation seen in this study was lower than that observed by others with tretinoin microsphere (0.1%) gel exposed to a simulated solar UV light source for a shorter period of time.[6]
These data are significant based on peak absorption characteristics of tretinoin, UVA skin penetration characteristics, and our overall knowledge about day-to-day levels of indoor and outdoor UVA exposure. Further work is underway to look at the impact of other wavelengths of light to fully evaluate this important area of research.
ACKNOWLEDGMENT
The authors acknowledge Brian Bulley, MSc, of Inergy Limited for medical writing support. Coria Laboratories, a wholly owned subsidiary of Valeant Pharmaceuticals North America, funded the writing assistance activities of Inergy pertaining to this manuscript.
references
1. Shroot B. Further light is shed on topical therapy. J Invest Dermatol. 2003;121(3):xiii–xiv.
2. Brisaert M, Plaizier-Vercammen JA. Investigation on the photostability of tretinoin in creams. Int J Pharm. 2007;334(1–2):56–61.
3. Del Rosso JQ, Pillai R, Moore R. Absence of degradation of tretinoin when benzoyl peroxide is combined with an optimized formulation of tretinoin gel (0.05%). J Clin Aesthet Dermatol. 2010;3(10):26–28.
4. Nyirady J, Lucas C, Yusuf M, Mignone P, Wisniewski S. The stability of tretinoin in tretinoin gel microsphere 0.1%. Cutis. 2002;70(5):295–298.
5. Martin B, Meunier C, Montels D, et al. Chemical stability of adapalene and tretinoin when combined with benzoyl peroxide in presence and in absence of visible light and ultra- violet radiation. Br J Dermatol. 1998;139(Suppl 52):8–11.
6. Nighland M, Yusuf M, Wisniewski S, Huddleston K, Nyirady J. The effect of simulated solar UV irradiation on tretinoin in tretinoin gel microsphere 0.1% and tretinoin gel 0.025%. Cutis. 2006;77(5):313–316.
7. Brisaert MG, Everaerts I, Plaizier-Vercammen JA. Chemical stability of tretinoin in dermatological preparation. Pharm Acta Helv. 1995;70:161–166.
8. Brisaert M, Plaizier-Vercammen J. Investigation on the photostability of a tretinoin lotion and stabilization with additives. Int J Pharm. 2000;199:49–57.
9. Tashtoush BM, Jacobson EL, Jacobson MK. UVA is the major contributor to the photodegradation of tretinoin and isotretinoin: implications for development of improved pharmaceutical formulations. Int J Pharm. 2008;352: 123–128.
10. Teraoka R, Konishi Y, Matsuda Y. Photochemical and oxidative degradation of the solid-state tretinoin tocoferil. Chem Pharm Bull. 2001;49(4):368–372.
11. Webster G, Cargill I, Quiring J, Vogelson CT, Slade HB. A combined analysis of two randomized clinical studies of tretinoin gel 0.05% for the treatment of acne. Cutis. 2009;83:146–154.
12. Lucky AW, Sugarman JL. Comparison of micronized tretinoin gel (0.05%) and tretinoin gel microsphere (0.1%) in subjects aged 10–14 years: a post-hoc analysis of efficacy and tolerability data from two randomized controlled clinical trials. Cutis. 2011. In press.
13. Huang XX, Bernerd F, Halliday GM. Ultraviolet A within sunlight induces mutations in the epidermal basal layer of engineered human skin. Am J Pathol. 2009;174:1534–1543.
14. Godar DE, Landry RJ, Lucas AD. Increased UVA exposures and decreased cutaneous Vitamin D(3) levels may be responsible for the increasing incidence of melanoma. Med Hypotheses. 2009;72(4):434–443.