Joshua A. Zeichner, MD; Rita V. Patel, MD; Miriam B. Birge, MD, both from Mount Sinai Medical Center, New York, New York
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Basal cell carcinoma is the most common form of nonmelanoma skin cancer in the United States. Treatment modalities include both surgical, medical, or combination therapy. In the following case, the authors report the successful treatment of a basal cell carcinoma on the nose with curettage followed by topical imiquimod 3.75% cream.
(J Clin Aesthet Dermatol. 2011;4(5):39–43.)
Basal cell carcinoma (BCC) is the most common form of nonmelanoma skin cancer in the United States.[1] Treatment modalities include surgical excision, electrodessication and curettage, cryotherapy, intra-lesional interferon, and topical imiquimod 5% cream. Clearance rates vary from 80 to 99 percent depending on the tumor size, anatomical location, and treatment modality employed.[2] Surgical treatments have high cure rates, but may carry significant morbidity and, in some cases, poor cosmetic outcomes. An effective and cosmetically acceptable medical treatment for BCC is of interest to both patients and practitioners.[3]
Imiquimod 5% cream has been used successfully in combination with curettage for the treatment of nodular and superficial BCC (sBCC).[4] Rigel et al[4] demonstrated complete clearance without recurrence of BCC over the course of one year with cosmetic results superior to electrodessication and curettage, which frequently results in hypertrophic scarring.[4,5] Another study evaluating curettage followed by imiquimod 5% cream showed a histological clearance rate of 94 percent of superficial and nodular BCCs after 6 to 10 weeks of therapy.[6] A third, larger study evaluating 90 patients resulted in 96-percent clearance after 36 months post-treatment with curettage followed by six weeks of imiquimod 5% cream application.[7]
In March 2010, imiquimod 3.75% cream was approved by the United States Food and Drug Administration (FDA) for the treatment of actinic keratoses.[8] In the following report, the authors describe a case of the use of imiquimod 3.75% in combination with curettage for the successful treatment of sBCC on the face.
Case Report
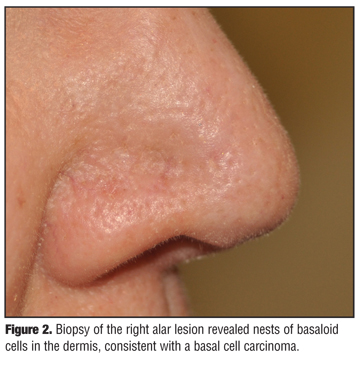
A 58-year-old woman presented to the office for evaluation of a 4mm, pearly papule of the right alar crease and ala (Figure 1). The lesion had increased in size over the past several months. She was otherwise healthy, and her past medical history was significant only for previous biopsies of benign nevi on the trunk. Biopsy of the right alar lesion revealed nests of basaloid cells in the dermis, consistent with a BCC (Figure 2). The patient expressed concerns with surgical excision so the decision was made to use a combination of curettage followed by imiquimod 3.75% cream. Figure 3 illustrates the appearance of the lesion two weeks after initial biopsy, and Figure 4 illustrates the appearance after curettage. One week after curettage, the patient applied imiquimod 3.75% to the area nightly for four weeks. Each morning, the cream was removed by washing with mild soap and water. After one month of imiquimod treatment, the patient developed a robust inflammatory reaction in the treatment area (Figure 5). She reported developing the reaction only in the last week of treatment. Clinically, she had an erythematous, crusted plaque on her nare. The patient discontinued imiquimod 3.75% cream and applied desoximetasone 0.25% ointment to the area for one week. After one week, the skin on the nare significantly improved (Figure 6). A repeat biopsy at that time revealed horizontally oriented collagen and confirmed clearance of the BCC with presence of a scar (Figure 7). After one month the nare remained clinically clear of BCC (Figure 8) and has remained clinically clear nine months after treatment.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
Imiquimod cream is an immune-response modifier that exerts its action through toll-like receptor 7 (TLR-7).[9,10] Stimulation of a type 1 helper T-cell (Th1) immune response and cytotoxic T-cells leads to recognition and destruction of virally infected cells and those that have undergone malignant transformation.[10–12] Imiquimod 5% cream is FDA approved for the treatment of actinic keratoses, external genital warts, and sBCC.[13] Imiquimod 3.75% cream is approved by the FDA for the treatment of actinic keratoses only.[8]
At a lower concentration, imiquimod 3.75% has a different dosing regimen than imiquimod 5% for actinic keratoses. Imiquimod 5% cream is applied twice weekly for 16 weeks to treat actinic keratoses. Studies evaluating attempts to shorten duration of treatment with more frequent applications have been poorly tolerated by patients.[14] At a lower concentration of 3.75%, however, imiquimod has been found to be effective and well tolerated using a regimen consisting of two weeks on, two weeks off, then two weeks on again.[15,16]
Imiquimod 5% cream is approved for the treatment of sBCC with application five times per week for six weeks.[13] In the pivotal trial for imiquimod 5% cream, 28 percent of patients experienced application-site reactions when applying the medicine five times per week for six weeks. Tolerability of imiquimod 5% continues to decline with increased dosing frequency when treating sBCC.[3,17] In developing a regimen to treat sBCC using imiquimod 3.75% cream, the authors used the same rationale as that used for the dosing regimen in the treatment of actinic keratoses. The patient used more frequent application of a lower concentration imiquimod cream and applied imiquimod 3.75% seven days per week for four weeks.
Combination therapy for BCC using imiquimod cream along with surgical treatments is more effective than the individual therapies alone. This has been demonstrated using imiquimod 5% cream in combination with Mohs surgery[18] as well as with curettage.[4,6,7] Several studies have shown that curettage followed by imiquimod 5% cream has given clearance rates ranging from 94 to 100 percent.[4,6,7] When evaluating curettage alone, the 15-year recurrence rate of BCC has been shown to be 10.5 percent.[19] Another study showed that 15.9 percent of BCC left residual cancer after aggressive curettage.20 Imiquimod 5% cream, when used alone (applied 5 times per week for 6 weeks), has been demonstrated to clear 82 percent of patients.21 Sustained clearance of BCC after imiquimod 5% cream lies in the range of 73 to 87.1 percent of patients.[22,23]
The use of imiquimod cream as an adjuvant therapy after curettage of sBCC has two main purposes. First, it may improve the cosmetic result and reduce the risk of keloid scar formation.[24] Secondly, imiquimod use causes inflammation in the skin, which itself may aid in clearing the lesion.[6,7,25]
This report represents only a single case of clearance of sBCC treated with curettage plus imiquimod 3.75% cream, and large studies must be performed to assess safety, efficacy, and sustained clearance. However, imiquimod 3.75% cream may be effective in treating sBCC using a dosing regimen appropriate for its concentration, similar to the regimen designed for the treatment of actinic keratoses. Future studies will be needed to evaluate the ideal dosing regimen. The patient described in this case developed a significant local adverse event in the fourth week of therapy, so the authors suggest both a four-week and a three-week dosing regimen, with seven-days-per-week application after curettage of the lesion.
Conclusion
The authors report a single case of effective treatment of sBCC through the use of curettage followed by imiquimod 3.75% with an excellent cosmetic result. Future studies will be needed to validate this result and assess safety, efficacy, the appropriate dosing regimen, and sustained clearance rates.
References
1. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med. 2005;353(21):2262–2269.
2. Surgical management of local disease. In: Miller SJ, Maloney ME, eds. Cutaneous Oncology: Pathophysiology, Diagnosis, and Management. Malden, MA: Blackwell Science; 1997:672–675.
3. Beutner KR, Geisse JK, Helman D, et al. Therapeutic response of basal cell carcinoma to the immune response modifier imiquimod 5% cream. J Am Acad Dermatol. 1999;41:1002–1007.
4. Rigel DS, Torres AM, Ely H. Imiquimod 5% cream following curettage without electrodesiccation for basal cell carcinoma: preliminary report. J Drugs Dermatol. 2008;7(1 Suppl 1): S15–S16.
5. Chren MM, Sahay AP, Sands LP, et al. Variation in care for nonmelanoma skin cancer in a private practice and veterans affairs clinic. Med Care. 2004;42:1019–1026.
6. Wu JK, Oh C, Strutton G, Siller G. An open-label, pilot study examining the efficacy of curettage followed by imiquimod 5% cream for the treatment of primary nodular basal cell carcinoma. Australas J Dermatol. 2006;47(1):46–48.
7. Tillman DK Jr, Carroll MT. A 36-month clinical experience of the effectiveness of curettage and imiquimod 5% cream in the treatment of basal cell carcinoma. J Drugs Dermatol. 2008;7(1 Suppl 1):S7–S14.
8. Zyclara [package insert]. Bristol, TN: Graceway Pharmaceuticals; 2010.
9. Hemmi H, Kaisho T, Takeuchi O, et al. Small anti-viral compounds activate immune cells via the TLR7 MyD88-dependent signaling pathway. Nat Immunol. 2002;3(2): 196–200.
10. Gibson SJ, Lindh JM, Riter TR, et al. Plasmacytoid dendritic cells produce cytokines and mature in response to the TLR7 agonists, imiquimod and resiquimod. Cell Immunol. 2002;218(1–2):74–86.
11. Miller RL, Gerster JF, Owens ML, Slade HB, Toami MA. Imiquimod applied topically: a novel immune response modifier and new class of drug. Int J Immunopharmacol. 1992(21):1–14.
12. Harison CJ, Miller RL, Bernstein DI. Imiquimod applied topically: a novel immune response modifier and new class of drug. Int J Immunopharmacol. 1999;21(1):1–14.
13. Aldara [package insert]. Bristol, TN: Graceway Pharmaceuticals; 2009.
14. Gebauer K, Shumack S, Cowen PSJ. Effect of dosing frequency on the safety and efficacy of imiquimod 5% cream for treatment of actinic keratosis on the forearms and hands: a phase II, placebo-controlled study. Br J Dermatol. 2009;161:897–903.
15. Hanke CW, Beer KR, Stockfleth E, et al. Imiquimod 2.5% and 3.75% for the treatment of actinic keratoses: results of two placebo-controlled studies of daily application to the face and balding scalp for two 3-week cycles. J Am Acad Dermatol. 2010;62(4):573–581.
16. Swanson N, Abramovits W, Berman B, et al. Imiquimod 2.5% and 3.75% for the treatment of actinic keratoses: results of two placebo-controlled studies of daily application to the face and balding scalp for two 2-week cycles. J Am Acad Dermatol. 2010;62(4):582–590.
17. Shumack S, Robinson J, Kossard S, et al. Efficacy of topical 5% imiquimod cream for the treatment of nodular basal cell carcinoma: comparison of dosing regimens. Arch Dermatol. 2002;138(9):1165–1171.
18. Torres A, Niemeyer A, Berkes B, et al. 5% imiquimod cream and reflectance-mode confocal microscopy as adjunct modalities to Mohs micrographic surgery for treatment of basal cell carcinoma. Derm Surg. 2004;30:1462–1469.
19. Reymann F. 15 years’ experience with treatment of basal cell carcinomas of the skin with curettage. Acta Derm Venereol Suppl (Stockh). 1985;120:56–59.
20. Johnson T, Tromovitch T, Swanson N. Combined curettage and excision: a treatment method for primary basal cell carcinoma. J Am Acad Dermatol. 1991;24:613–617.
21. Geisse J, Caro I, Lindholm J, et al. Imiquimod 5% cream for the treatment of superficial basal cell carcinoma: results from two phase III, randomized, vehicle-controlled studies. J Am Acad Dermatol. 2004;50(5):722–733.
22. Gollnick H, Barona CG, Frank RGJ. Recurrence rate of superficial basal cell carcinoma following treatment with imiquimod 5% cream: conclusion of a 5-year long-term follow-up study in Europe. Eur J Dermatol. 2008;18(6): 677–682.
23. Lien MH, Sondak VK. Nonsurgical treatment options for basal cell carcinoma. J Skin Cancer. 2011;2011:571734. Epub 2011 Jan 9.
24. Malhotra AK, Gupta S, Khaitan BK, Sharma VK. Imiquimod 5% cream for the prevention of recurrence after excision of presternal keloids. Dermatology. 2007;215:63–65.
25. Spencer JM. Pilot study of imiquimod 5% cream as adjunctive therapy to curettage and electrodesiccation for nodular basal cell carcinoma. Dermatol Surg. 2006;32(1):63–69.