Jerry K. L. Tan, MD, FRCPC; Jing Tang, MSc
Dr. Tan is Adjunct Professor, University of Western Ontario and Windsor Clinical Research Inc., Windsor, Ontario, Canada. Jing Tang is Statistician, Windsor Clinical Research Inc., Windsor, Ontario, Canada (currently with Fraser Health Authority, Vancouver, British Columbia, Canada)
Dr. Tan is the patent holder of this invention. He has served as an advisor, trialist, and/or speaker in acne for Bayer, Cipher, Galderma, GSK/Stiefel, and Photocure. Ms. Tang reports no relevant conflicts of interest.
Abstract
Background: The scientific integrity of outcome measurements is dependent upon reproducibility and accuracy. In acne assessments, there is no current gold standard for accuracy in lesion counting and global grading. Purpose: The purpose of this study was to create facial acne replicas for use in acne training and for evaluation of rater accuracy. Methods: Two full-sized, three-dimensional, silicone-based, facial replicas with predetermined acne lesion type and number were created. Their teaching value was evaluated by dermatologists and clinical coordinators undergoing training in acne evaluations. A questionnaire after the training session addressed realism, preferences, and ease of assessments with the facial replicas compared to live subjects. Results: Of 55 potential respondents, 32 questionnaires were completed and analyzable. Of these, 23 were from dermatologists and nine were from clinical research coordinators performing acne assessments. The facial replicas were considered sufficiently realistic for acne lesion counting by 91 percent (29/32) and for global grading by 94 percent (30/32). Of these, 66 percent preferred to have both real subjects and replicas for training (21/32), 31 percent preferred real subjects only (9/32), and one preferred replicas only. Replicas were considered easier to evaluate for noninflammatory and inflammatory lesions (p=0.002 and p=0.013, respectively) and equivalent to live models for global grading (p=0.001). Limitations: Shortcomings include the limited spectrum of acne that could be represented due to production of only two prototypes, the relative paucity of secondary lesions, and production time and cost. Conclusion: These facial replicas provide a realistic and practical method for teaching and evaluating raters in acne outcome measures as they provide a gold standard for acne lesion counts. Furthermore, their use may obviate some of the shortcomings inherent in recruitment of human acne volunteers for acne training sessions. (J Clin Aesthetic Dermatol. 2010;3(6):35–38.)
Acne global severity grading and lesion counting are critical outcome parameters for establishing the efficacy of treatments in clinical trials for acne.[1] The scientific credibility of such measurements is dependent on their reproducibility and accuracy. While two previous studies have evaluated the reliability of raters in acne lesion counting and severity grading, accuracy is undetermined as no gold standard exists.[2,3]
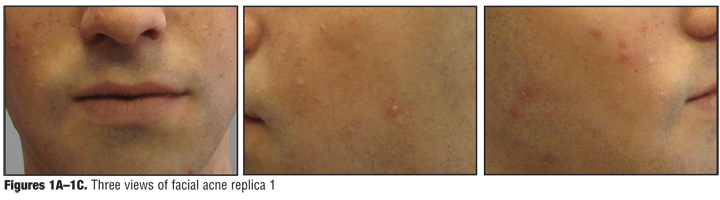
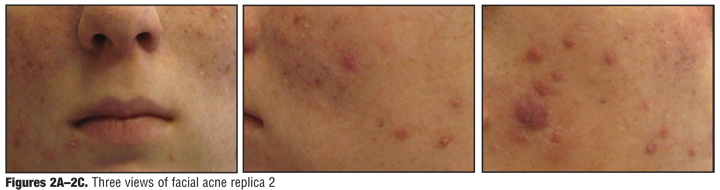
In the history of dermatology, anatomical figures for representation and teaching of skin diseases have been available since the 18th century. The art of constructing such life-sized, three-dimensional replicas with wax casts (moulages) peaked in the early and mid-19th century during which time unusual cases, representations of common conditions including acne, and research findings were portrayed.[4,5] Based on the three-dimensional, full-sized representations of moulages, the authors’ objective was to modernize this concept with contemporary materials by creating full-sized, silicone-based, facial replicas. These were constructed with predetermined type, number, and distribution of primary acne lesions. In this study, we evaluated the value of the first two of these facial silicone prototypes in acne lesion counting and severity grading.
Methods
Dermatologists and clinical trial coordinators attending investigator meetings for an international interventional acne study underwent a 30-minute presentation on acne lesion counting and severity grading. Subsequently, they performed acne evaluations on up to five human volunteers with acne and on the two facial acne replicas. A survey of attendees regarding rater perceptions on replica realism, preferences, and ease of evaluations were recorded anonymously after the training session. The survey was conducted and data collated by a third party to avoid the potential for bias.
Construction of facial silicone replicas. The construction of the facial silicone replicas involved two human subjects for facial mask casting to obtain negative impressions. Subsequently, clay positive impressions were obtained, resculpted, and clay negative impressions were produced. From the latter, silicone templates were generated. Subsequently, intrinsic complexion coloring and hair prostheses were added. Finally, predetermined numbers and types of primary acne lesions were applied to specific facial locations (as disclosed in pending Canadian Patent application number 2,668,241).
Statistics. Responses for preferences of raters for replicas versus live subjects and realism of replicas were evaluated with the Chi-square test. Responses for ease of evaluations using replicas versus live subjects for lesion counts and for global severity grading was performed with the Kruskal-Wallis test. Stratification of responses was also performed, based on prior experience in acne evaluations: no experience, a little experience (up to 3 acne trials), and quite experienced (more than 3 acne trials). All other associations were evaluated by Fisher’s exact test. All statistical analyses were performed with SPSS software (SPSS Inc, Version 17) and significance was established at the five percent level.
Results
Of 55 questionnaires, 32 were fully completed (58% response rate) and included in this analysis. Of these, 78 percent were obtained from dermatologists (25/32) and 22 percent from clinical research coordinators performing acne evaluations (7/32). Excluded from further analysis were incomplete questionnaires, those from coordinators who would not be performing acne evaluations, and those whose role was not specified.
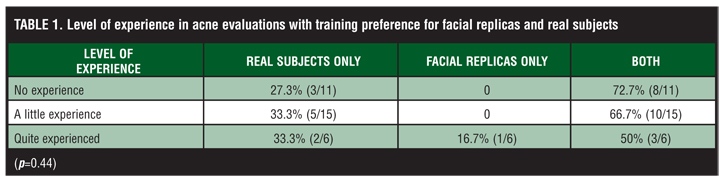
The facial replicas (Figure 1 and Figure 2) were considered to be sufficiently realistic for acne lesion counting by 91 percent (29/32) and for global grading by 94 percent (30/32). For the purpose of training, 66 percent preferred to have both real subjects and replicas (21/32) and 31 percent preferred real subjects only (10/32). One person preferred the replicas only. These preferences did not differ with respect to prior experience in acne evaluations (Table 1) (Chi-square, p=0.44).
{kind=link}
{kind=link}
{kind=link}
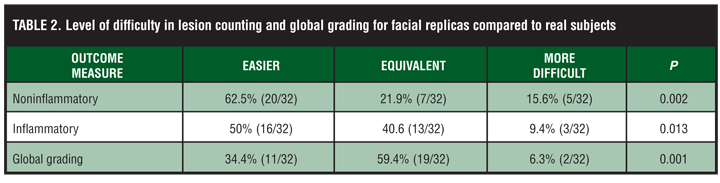
The comparative ease or difficulty of acne evaluations using the replicas is shown in Table 2. Lesion counting with replicas was considered easier for noninflammatory lesions by 63 percent and for inflammatory lesions by 50 percent (p=0.002 and p=0.013, respectively) compared to real subjects. Assessment of global severity was considered to be easier by 34 percent and equivalent by 59 percent (p=0.001). While there was a trend for more experienced investigators to indicate that counting noninflammatory lesions and global assessments were easier to perform on replicas compared to real subjects, the difference was not statistically significant.
{kind=link}
Discussion
The scientific basis of interventional studies promotes trial designs that minimize the risk of sampling error. Correspondingly, to enhance the validity of drawing inferences from these studies, outcome measures in such trials should be designed to minimize measurement error. Thus, the accurate (absence of systematic error) and reproducible (absence of random error) assessment of disease is essential in evaluating the effect of therapeutic interventions. For acne vulgaris, evaluation of treatment efficacy has been largely based on lesion counting and physician global assessments.[1] While prior studies have evaluated the precision of raters in lesion counting, none have assessed accuracy.[2,3]
Wax moulages provided a historical means of representing skin disease and were used for teaching purposes. However, there were important limitations in wax media that would preclude their current application in dermatological modeling: inadequate representation of fine surface details, inadequate spectrum of colors to realistically portray the subtle variations in human skin, and the risk of wax denaturation with temperature and humidity fluctuations.[4] In contrast, the use of silicone in construction of skin replicas can facilitate reproduction of surface skin detail in a resilient material resistant to natural degradation. Furthermore, this material can be gently palpated by examiners as part of the cutaneous examination process without risk of deterioration. A recent study using silicone-based replicas of skin lesions has demonstrated the value of this approach in teaching in dermatology to medical students.[6] The authors extended this concept by developing full-sized, three-dimensional, facial replicas upon which primary acne lesions were created.
The authors highlight the following findings from this study on the value of these facial acne silicone replicas in acne outcome training. The majority (>90%) of raters indicated that the facial replicas were sufficiently realistic for acne lesion counts and global grading. Furthermore, 72 percent preferred using the replicas during the evaluation session, either with or without real subjects. These preferences did not vary with prior experience in acne studies.
The limitations of this study are due to the small number of replicas available and those inherent to prototypes including the relative paucity of secondary acne lesions (scarring, staining, dyspigmentation) and darker skin phototypes. Future replicas will include these variations to expand the spectrum of presentations. Additionally, while primary lesions may present in an array of morphologies, final decisions on lesion details were provided by a single dermatologist (JT). Finally, the time and cost for construction of these replicas is likely to limit their widespread application in training.
There are multiple limitations in the use of human volunteers for evaluation of acne lesions in training sessions, including recruitment of patient volunteers with adequate spectrum of disease severity, their inattendance during the day of the meeting, and variation in lesion appearance over time with repeated palpation by raters and heat generated from lighting sources. These issues are compounded when multiple meetings are held for international studies. The use of facial replicas can ameliorate many of these issues and provide a standardized means for evaluating rater accuracy in acne assessments.
In summary, these facial silicone replicas represent a means by which art can support science. In particular, they provide a realistic and practical method for teaching acne outcome measures. By predetermination of lesion types and numbers for each replica, they can provide a gold standard for accuracy in acne lesion counting. The absence of such a standard has been a vexatious issue for which there was no adequate prior solution. Their use can enhance the training of evaluators in acne assessments and provide a means for their evaluation in establishing accuracy and reliability. Furthermore, their use may reduce the shortcomings inherent in the recruitment of human acne volunteers for acne training sessions.
Acknowledgment
The authors would like to acknowledge CJ Goldman for casting and constructing the facial replicas and Pascale Soto of Galderma for allowing the use of these prototypes in acne training sessions. This work was partially presented at the 2009 American Acne and Rosacea Society Meeting in San Francisco, California.
References
1. U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER). Guidance for Industry; AcneVulgaris: Developing Drugs for Treatment; September 2005.
2. Lucky AW, Barber BL, Girman CJ, et al. A multirater validation study to assess the reliability of acne lesion counting. J Am Acad Dermatol. 1996;35:559–565.
3. Tan JK, Fung K, Bulger L. Reliability of dermatologists in acne lesion counts and global assessments. J Cutan Med Surg. 2006,10:160–165.
4. Worm AM, Hadjivassiliou H, Katsambas A. The Greek moulages: a picture of skin diseases in former times. J Eur Acad Dermatol Venereol. 2007;21:515–519.
5. Geiges ML. Traces of Marion B. Sulzberger in the Museum of Wax Moulages in Zurich and their importance for the history of dermatology. J Am Acad Dermatol. 2009;60:980–984.
6. Garg A, Haley HL, Hatem D. Modern moulage: evaluating the use of 3-dimensional prosthetic mimics in a dermatology teaching program for second-year medical students. Arch Derm. 2010;146(2):143–146.