Mark S. Nestor, MD, PhD, Center for Clinical and Cosmetic Research, Aventura, Florida; Glynis R. Ablon, MD, Ablon Skin Institute, Manhattan Beach, California; Mark A. Stillman, PhD, Center for Clinical and Cosmetic Research, Aventura, Florida
Disclosure: Dr. Nestor has received research grant support from and is a consultant and speaker for Medicis. Dr. Ablon has been a consultant for Medicis. Dr. Stillman reports no relevant conflicts of interest. This study was funded by an unrestricted educational grant from ThermoTek. The product used in this study was supplied by Medicis Aesthetics Incorporated.
Abstract
Objectives. Consensus guidelines developed for the use of hyaluronic acid dermal fillers describe the use of cooling the skin to reduce patient discomfort during injection. The vasoconstrictive effects of cold may provide reduced ecchymosis and swelling at the site. However, the effect of applying ice or cooled air is unpredictable because these modalities do not deliver precise temperature, which may result in cold burn or insufficient effect to targeted areas. This open-label, randomized, single-blinded, split-face trial was conducted to measure the extent to which applying a spot cooling device reduces patient discomfort and ecchymoses in the clinical setting in patients undergoing a dermal filler procedure. Subjects. Twenty male and female subjects of any race, ages 35 to 65 years, with moderate and severe nasolabial folds were included in this study. Seven (35%) subjects had received previous small gel particle hyaluronic acid injections. Methods. Prior to injection, the topical cooling system was set at 35°F and a cooled applicator was applied for 20 seconds on one nasolabial fold. A control using a noncooled applicator was applied for 20 seconds on the other nasolabial fold. Postprocedure ice packs were prohibited so as not to confound the subject’s perception of procedure-related pain. Subjects (using visual analog pain scales) and blinded investigators rated pain and ecchymosis using predetermined scales and satisfaction surveys. Results. Use of the cooling system was associated with mean pain reduction of 61, 70, and 42 percent compared to control, as measured by visual analog pain scales, immediately following and one hour and three hours post small gel particle hyaluronic acid injection. Additionally, use of the cooling system was associated with mean ecchymosis reduction of 88, 89, 80, and 66 percent compared to control immediately following injection, one hour, three hours, and next-day postinjection. Conclusion. The cooling system provided adequate pain management (both subjectively and objectively through blinded evaluations) during and after small gel particle hyaluronic acid dermal filler injections for the correction of moderate nasolabial folds. Furthermore, results demonstrate that the cooling system is associated with decreased ecchymosis. Future studies are needed comparing the use of topical anesthetics to a cooling system for the reduction of pain and ecchymosis associated with the use of dermal filler injections.
(J Clin Aesthetic Dermatol. 2010;3(3):29–34.)
The number of aesthetic procedures requiring the use of needle-based injections is progressively increasing due to their widely successful and effective results.[1] Of these injections, botulinum toxins and injectable hyaluronic acid dermal fillers are most often used. According to the American Society for Aesthetic Plastic Surgery, hyaluronic acid gels account for approximately 80 percent of the nearly two million soft tissue filler injections performed in 2006.[1] The most commonly utilized soft tissue filler is Restylane® (Medicis Aesthetics Inc., Scottsdale, Arizona), a small gel particle hyaluronic acid (SGP-HA) that is indicated for mid-to-deep dermal implantation for the correction of moderate-to-severe facial wrinkles and folds, such as nasolabial folds.[2] All injections may cause some discomfort to the patient as well as postinjection ecchymosis and swelling. Topical anesthetics and ice are the most often employed methods for limiting the degree of pain, ecchymoses, or swelling.
Much research has been devoted to the development of effective topical anesthetics of the skin to minimize or eliminate the discomfort experienced by the patient during the procedure.[3] Many studies exist that scrutinize the efficacy of topical anesthetics for dermatological procedures,[4] and several studies specifically have investigated mixing 2% lidocaine with HA prior to injection.[5,6] Effective anesthesia via topical administration is difficult to achieve on keratinized or nontraumatized skin due to limited transepidermal absorption. Various creams, ointments, and gels have been used for this; however, their efficacy has been less than ideal and complications have occurred. While a variety of topical anesthetics are currently available, their use is limited by variable efficacy, lengthy application times, and often elaborate and time-consuming techniques for occlusion and removal of the anesthetic. Consequently, there has been an increased need for safe, more effective, and expedient topical anesthesia.
Recently, research has turned toward alternative methods of topical anesthesia when injecting dermal fillers, such as skin cooling through the use of ice or cooled air. The use of cold to relieve pain has been employed since Hippocrates in the 4th century BC.[7] Cooling the tissue also induces vasoconstriction, which may decrease swelling and ecchymosis.[8] The Restylane Consensus Group published its proceedings, which included the use of patient comfort techniques, such as the use of icing before, during, and after treatment with HA.[8] Half of the panel members assert that icing after treatment achieves the most benefit, yet another 40 percent of members use ice before, during, and after treatment. The American Society for Dermatologic Surgery (ASDS) Guidelines recommend several mechanisms to diminish dermal filler injection pain including preinjection application of ice.[9] Unfortunately, the effect of applying ice or cooled air is often unpredictable because these modalities cannot be delivered accurately and precisely to targeted areas. Also, applying ice and cooled air directly to the site of injection may be associated with risks to the patient because the temperature is imprecise and cannot be controlled.
The ArTek Spot® (ThermoTek, Inc., Flower Mound, Texas), a commercially available spot contact cooling system, has been used to control pain associated with hair and tattoo removal procedures. It also has been used to prevent pain and discomfort associated with dermal fillers and other injectables as an alternative to ice cubes, ointments, and chemical sprays.[10] To date, however, no randomized, controlled trials have assessed its safety and efficacy for prevention of pain and ecchymosis in subjects receiving dermal filler injections.
The purpose of this study was to assess the efficacy, safety, and subject satisfaction of a contact topical cooling system on the reduction of subjective and objective pain and ecchymosis when applied prior to HA gel injections for correction of nasolabial folds.
Methods
Subjects. This study received full institutional review board approval by US IRB, Inc. prior to commencement (U.S.IRB2009CCCR/01). The study was conducted as an open-label, randomized, split-face, two-center, investigator-blinded trial involving male and female subjects ages 35 to 65 years with moderate nasolabial folds. Subjects were excluded if they had used aspirin, nonsteroidal anti-inflammatory drugs (NSAIDS), anticoagulants, St. John’s Wort, or high doses of Vitamin E within two weeks prior to screening/treatment. Any subject who had received dermal fillers within 12 months was also excluded.
Twenty subjects were enrolled at two sites in the United States. At the Screening visit, written, informed consent was obtained from each subject. If the subject agreed to participate, he or she was assigned the next sequentially available subject number. In addition, each subject’s medical history, demographic information, and previous and concomitant medications were collected and reported. The subject was asked to return to the investigative site on a scheduled visit (Day of Injection).
On the Day of Injection, blinded investigators utilized a randomization scheme for assigning each subject a side of the face for application of the cooling system. Prior to injection, the topical cooling system was set at 35°F and a cooled applicator was applied for 20 seconds on one nasolabial fold. A control using a noncooled applicator was applied for 20 seconds on the other nasolabial fold. The physician assistant applied the applicator without the investigator knowing whether it was cooled or noncooled. Postprocedure ice packs were prohibited so as not to confound the subject’s perception of procedure-related pain.
Investigators injected the SGP-HA using a linear threading technique, injecting the fold from top to bottom in a retrograde fashion, beginning with the right nasolabial fold. Investigators made every attempt to inject the SGP-HA into the skin with a uniform speed to cause slow, gentle distention of the dermis. At the discretion of the investigator and in an effort to achieve appropriate cosmetic results, a crosshatching technique was allowed as long as the process was utilized for both nasolabial folds. Investigators used the 30-gauge needle provided with the syringe and did not change to a different needle during the procedure. The investigators used a similar injection technique on both nasolabial folds, injecting similar amounts of SGP-HA with the same number of injections. Dosage was limited to one syringe per nasolabial fold. Patients received a similar number of injections and amounts of SGP-HA.
Upon first needle stick and upon completion of the injections at each treatment site, the subject assessed the amount of pain associated with the procedure by completing the visual analog pain scale (VAS) (see outcome measures) for the respective injection time. Thereafter, the blinded investigator, who was blinded as to which side of the face the cooled versus noncooled applicator was applied, also assessed the perceived degree of anesthesia the application provided for the subject. Following this initial pain assessment, the investigator continued the SGP-HA injections into the other nasolabial fold. The initial time of injection, volume of the SGP-HA used, time to completion, and the total number of injections for each treatment area were collected and recorded.
Outcome Measures
Visual analog pain scale. The subject was asked to evaluate the pain experienced at first needle stick, immediately postinjection, and then one and three hours after the procedure by responding to the VAS. Subjects were prompted by the investigator when it was time to rate their pain through the VAS. The subject completed the VAS by drawing a single vertical line through a 10cm horizontal line labeled “no pain” at the left end and “the worst pain you can imagine” at the right end. Following completion of the study, the distance from the furthest left vertical axis of the scale (no pain) and the patient’s VAS mark was measured in millimeters using a ruler.
Blinded investigator ratings. The blinded investigator scored the degree of perceived subject pain experienced during the procedure using a Likert scale. The Likert scale ranged from “no perceived pain” (0) to “severe pain” (3). In addition, for each treatment area, the investigator evaluated his/her overall assessment of the efficacy of the cooling system by responding to the following question: Did the cooling system provide adequate anesthesia for the dermal filler procedure?
Immediately after the cooling system applicators were removed from the subject’s skin and just prior to the HA injections, the investigator examined the areas for ecchymosis. Ecchymosis was graded on a scale from 0 (none) to 4 (severe) immediately postinjection and then one hour after and three hours after the procedure. This assessment was also conducted the day after treatment.
Subject satisfaction surveys. After completing the pain assessment one hour post-treatment, subjects were asked to complete a satisfaction survey addressing their assessment of the pain management options utilized. The survey consisted of two parts, one that assessed subjects’ impressions with pain management at each treatment site and another that assessed subjects’ overall impression (Appendix A).
Statistical Evaluation
All analyses were performed with SPSS version 13.0 (SPSS, Inc., Chicago, Illinois). Differences among the mean pain levels, as measured by the VAS, were analyzed using two-tailed, paired, independent sample t-tests (cooled vs. noncooled—immediate, 1 hour, 3 hours). Differences in the proportions of the blinded investigators’ ratings of perceived pain were compared using a 2X3 chi-square analysis (cooled vs. noncooled—no pain vs. slight pain vs. moderate pain). Proportions of the blinded investigators ratings of the overall efficacy of the cooling system were analyzed using a 2X2 chi-square analysis (cooled vs. noncooled—satisfied vs. nonsatisfied). Differences among the mean levels of ecchymosis were analyzed using two-tailed, paired, independent sample t-tests (cooled vs. noncooled—immediate, 1 hour, 3 hours, next day). Lastly, differences in the proportions subject’s ratings of pain were compared using a 2X4 chi-square analysis (cooled vs. noncooled—no pain vs. minimal pain vs. mild pain vs. moderate pain).
Results
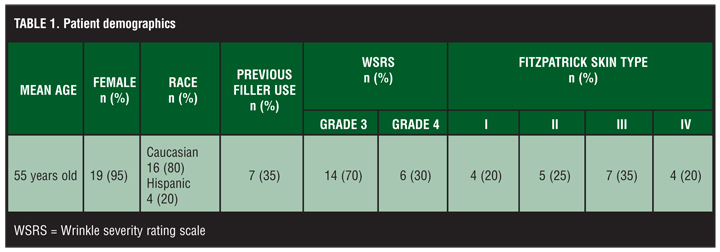
There were 20 subjects enrolled in this study, 19 (95%) of whom were female. The mean age was 55 years old (Table 1). Thirty-five percent of the subjects (n=7) had received previous treatment with Restylane into their nasolabial folds prior to this study, and 65 percent (n=13) were naïve to treatment with a dermal filler.
{kind=link}
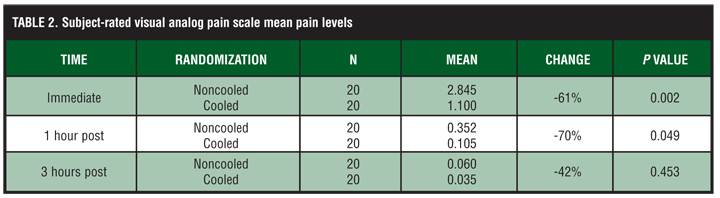
Statistically significant differences (P<0.05) were found in the mean pain levels, as measured by the VAS, on the side of the face where the cooled applicator was applied versus the side of the face where the noncooled applicator was applied (Table 2). Specifically, subjects expressed significantly less pain (61%) immediately following SGP-HA injections on the side of the face that was randomly assigned to the cooled applicator [t(20) = -3.266, P=0.002]. Likewise, subjects expressed significantly less pain (70%) on the cooled side of the face as compared to the noncooled side at one hour postinjection [t(20)=-2.034, P=0.049]. Three hours postinjection, even though pain levels were much lower, the mean VAS pain levels were 42-percent less on the cooled side. The results were not statistically significant [t(38) = -0.758, P=0.453] based on the low VAS scores at three hours.
{kind=link}
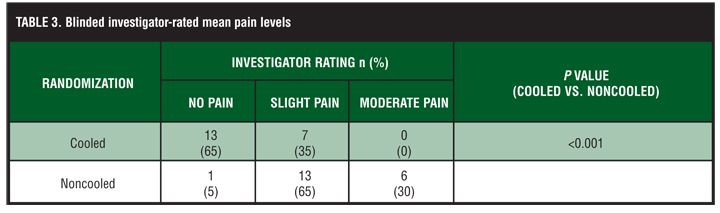
Statistically significant differences (P<0.05) were found in the blinded investigators ratings of perceived pain on the side of the face where the cooled applicator was applied versus the side of the face where the noncooled applicator was applied. Specifically, the blinded investigators reported a greater proportion of severe and moderate pain ratings to the side of the face where the noncooled applicator was used; whereas, a greater proportion of no pain and slight pain ratings were given to the side of the face where the cooled applicator was utilized [x2 (2, N=40) = 18.086, P<0.001] (Table 3).
{kind=link}
Likewise, statistically significant differences (P<0.05) were again found in the blinded investigators ratings of the overall assessment of the efficacy of the cooling system. Specifically, the blinded investigators’ responses indicated that the cooled applicator provided effective anesthesia for the dermal filling procedure [x2 (1, N=40) = 40.00, P<0.001].
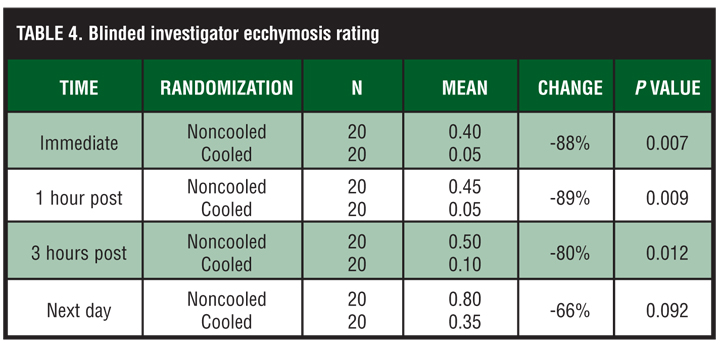
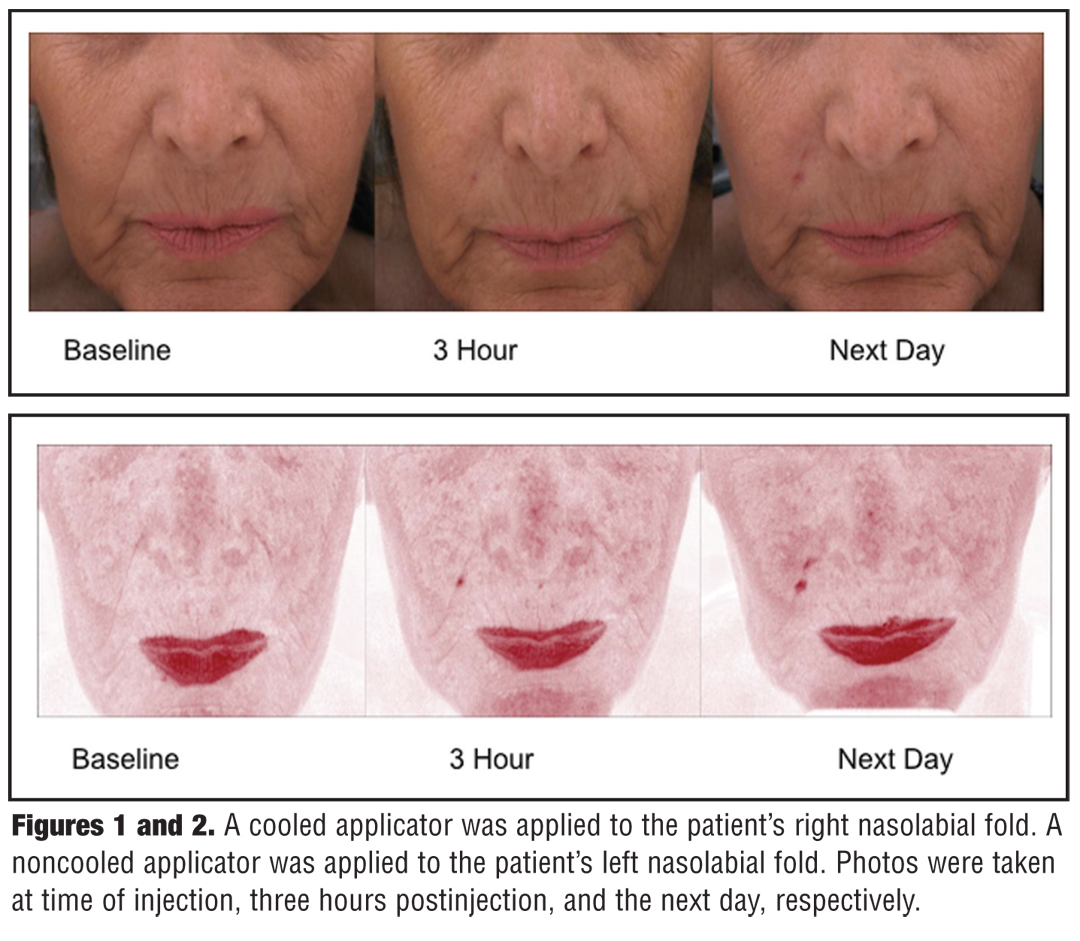
There was a statistically significant reduction in ecchymoses on the sides of the face using the cooled applicator versus the sides using the noncooled applicator immediately following injection (88%, P=0.007], one-hour postinjection [89%, P=0.009], and three hours postinjection [80%, P=0.012]. There was a 66-percent mean reduction in ecchymosis the day following injection on the side of the face where the cooled applicator was utilized [66%, P=0.092] (Table 4, Figures 1 and 2).
{kind=link}
{kind=link}
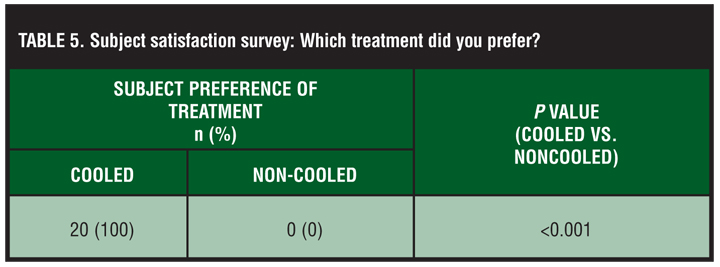
Results obtained from subject satisfaction data revealed a significant preference for the cooling system. Specifically, 20 out of 20 subjects reported that they preferred the anesthetic properties of the cooled applicator as compared to the noncooled applicator [x2 (1, N=40) = 40.00, P<0.001] (Table 5). Moreover, trends toward greater proportions of “no pain” and “slight pain” ratings emerged in the subjects’ ratings of pain on the side of the face where the cooled applicator was applied [x2 (3, N=40) = 6.743, P=0.081]. One hundred percent (100%) of the subjects indicated that they would consider having the procedure done again and would recommend it to a friend or family member.
{kind=link}
Discussion
Patient comfort is an important consideration during aesthetic procedures. In fact, minimal pain ranked third in importance only bested by cosmetic outcome and communication in determining patient satisfaction and willingness to undergo skin rejuvenation treatments.[11] Topical anesthetics are, hence, invaluable tools for dermatologists. Many local anesthetics, however, do not provide effective anesthesia due to their inability to penetrate the skin and may cause a variety of complications, such as allergic reactions and toxicities.[12] In a review of the topical anesthetics used in cosmetic and laser dermatology, Amin and Goldberg[3] noted that in some patients, local anesthetics may be associated with a narrow margin of safety.[4]
Patients may manifest minor signs and symptoms of anesthetic toxicity such as tinnitus, perioral tingling, or metallic taste.[3] In addition, the use of topical anesthetics may require increased time involvement for the patient, practitioner, and staff, as topical anesthetics must be applied 10 to 15 minutes prior to the procedure.
As alternatives to local anesthetics, various other methods have undergone research. Specifically, the analgesic effect of vibration in minimizing pain in patients undergoing a variety of cosmetic procedures was studied. However, results indicate that while vibration anesthesia may increase the tolerability of the procedures, it does not eliminate the pain completely.[13]
Subsequent research in alternative analgesic methods given prior to botulinum toxin type A (BoNT-A) injections has dem-onstrated that pain, bruising, hematoma, and ecchymosis can be prevented by cooling the skin prior to and following BoNT-A injections.[14] Bechara et al[15] studied the effect of skin cooling on pain during BoNT-A injections and found that application of both ice and cooled air significantly result in decreased pain.[15] Other researchers have demonstrated the effect of the cooling properties of transparent hydrogel pads on patients undergoing nonablative laser surgery and have reported that patients experience less discomfort when using this method of anesthesia.16 Other cooling tech-niques, such as forced air analgesia, have been reported to decrease the discomfort associated with fractional photothermolysis treatment.[17] More-over, significant reduction in injection pain by as much as 25 percent has been demonstrated via the use of cryopreparation by local ice application immediately prior to injection.[18]
Overall, the present study demonstrated that subjects ex-perienced a 61-percent mean reduction in immediate pain and between 66- and 89-percent mean reduction in ecchymosis when a cooling system was applied prior to SGP-HA injections in the nasolabial fold versus placebo. This finding may be of significance given the relative ease and safety of a cooling system applied to the skin prior to a cosmetic procedure as compared with a topical or an injectable product that may present a variety of complications and challenges, such as allergic reactions, skin-sensitivity concerns, and quantity and dosage control.
Results obtained from ecchymosis assessments are also of special interest, given that ecchymosis severity was significantly less on the side of the face where the cooled applicator was applied. Due to cold-induced vasoconstriction, it is feasible to posit that the cooling system may result in decreased postinjection bruising. This may be an added benefit to the practitioner if telephone calls from patients concerned about bruising appearing the day after the procedure are decreased or eliminated.
One hundred percent of subjects indicated that they would consider having the procedure done again and would recommend it to a friend or family member. Increasing patient comfort may encourage development of routine regimens of hyaluronic acid dermal filler treatments that have been shown to be beneficial due to collagen production.[20] Results from a long-term study designed to determine longevity of Restylane treatment suggested that early retreatment, scheduled at 4.5 months after the initial treatment, may halt or slow deterioration of the initial treatment as well as result in a continued response for at least one year without additional treatment.[21]
Based on the results of this study, the cooling system provided adequate pain management (both subjectively and on an objective, blinded evaluation) during and after SGP-HA dermal filler injections for the correction of nasolabial folds. Furthermore, results demonstrate that the cooling system is associated with decreased ecchymosis. Although this study only examined the use of the cooling system with SGP-HA dermal filler injections, the findings may apply to other aesthetic injectables, such as botulinum toxin type A and other dermal filler injection procedures. Future studies are needed comparing the use of topical anesthetics to a cooling system for the prevention of discomfort and ecchymoses due to the use of aesthetic injections.
Acknowledgment
The authors wish to acknowledge Anne Gentry, PharmD, for her assistance with the writing of this manuscript. Her fees were paid for by Medicis.
References
1. American Society for Aesthetic Plastic Surgery. Cosmetic Surgery National Data Bank: 2006 Statistics. http://www. surgery.org/download/2006stats.pdf. Accessed on February 17, 2010.
2. Seo DW, Hong JP. The use of topical skin cooling device to achieve pain relief of injection induced pain. Plas Reconstruc Surg. 2009;123:111e–112e.
3. Amin SP, Goldberg DJ. Topical anesthetics for cosmetic and laser dermatology. J Drugs Dermatol. 2005;4:455–461.
4. Huang W, Vidimos A. Topical anesthetics in dermatology. J Am Acad Dermatol. 2000;43:286–298.
5. Weinkle SH. A technique for mixing hyaluronic acid filler with lidocaine to reduce pain in the treatment of nasolabial folds. Poster presented at: Winter Clinical Dermatology Conference; January 16, 2009; Kohala Coast, HI.
6. Swetman G, Lupo MP, Waller W. Comparison of the efficacy and tolerability of non-animal stabilized hyaluronic acid filler with and without lidocaine HCl 2% for the correction of nasolabial folds. Poster presented at: Fall Clinical Dermatology Conference; October 2009; Las Vegas, NV.
7. Physical methods for treatment of pain. In: Auerbach: Wilderness Medicine, 5th ed. Available online. Mosby, An Imprint of Elsevier; 2007.
8. Matarasso SL, Carruthers JD, Jewell ML, et al. Consensus recommendations for soft-tissue augmentation with nonanimal stabilized hyaluronic acid (Restylane). Plast Reconstr Surg. 2006;117:3S–34S.
9. Alam M, Gladstone H, Kramer EM, et al. ASDS guidelines of care: injectable fillers. Dermatol Surg. 2008;34:S115-S148.
10. ArTec Spot [product information]. Flower Mound, TX: ThermoTek, Inc.; 2009.
11. Rosenthal KJ. Anesthesia for skin rejuvenation. Ophthalmol Clin North Am. 1998;11:207–217.
12. Leopold CS, Maibach HI. Percutaneous penetration of local anesthetic bases: pharmacodynamic measurements. J Invest Dermatol. 1999;113:304–307.
13. Smith KC, Comite SL, Balasubramanian S, Carver A, Liu JF. Vibration anesthesia: a noninvasive method of reducing discomfort prior to dermatologic procedures. Dermatology Online Journal. 2004;10(2):1.
14. Wollina U, Konrad H. Managing adverse events associated with botulinum toxin type A: a focus on cometic procedures. Am J Clin Dermatol. 2005;6:141–150.
15. Bechara FG, Sand M, Altmeyer P, Sand D, Hoffman K. Skin cooling for botulinum toxin A injection in patients with focal axillary hyperhidrosis: a prospective, randomized, controlled study. Ann Plast Surg. 2007;58:299–302.
16. Cassuto D, Mollia JF, Scrimali L, Sirago P. Right-left comparison of hydrogel pad versus transparant fluid gel in patients with dermo-cosmetic lesions undergoing non-ablative laser therapy. J Cosmetic Laser Ther. 2009;11:45–51.
17. Fisher GH, Kim KH, Bernstein LJ, Geronemus RG. Concurrent use of a handheld forced cold air device minimizes patient discomfort during fractional photothermolysis. Dermatologic Surg. 2005;31:1242–1244.
18. Goel S, Chang B, Bahn K, El-Hindi N, Koli S. “Cryoanalgesic preparation” before local anesthetic injection for lid surgery. Orbit. 2006;25:107–110.
19. Elibol O, Ozkan B, Hekimhan PK, Caglar Y. Efficacy of skin cooling and EMLA cream application for pain relief of periocular botulinum toxin injection. Ophthalmic Plast Reconstr Surg. 2007;23:130–133.
20. Wang F, Garza LA, et al. In-vivo stimulation of de novo collagen production caused by cross-linked hyaluronic acid dermal filler injections in photo-damaged skin. Arch Dermatol. 2007;143:155–163.
21. Narins RS, Dayan SH, Brandt FS, Baldwin EK. Persistence and improvement of nasolabial fold correction with nonanimal-stabilized hyaluronic acid 100,000 gel particles/mL filler on two retreatment schedules: results up to 18 months on two retreatment schedules. Dermatol Surg. 2008;34:S2–S8.