Roger Ceilley, MD, University of Iowa, Department of Dermatology, Iowa City, Iowa
Andrew Eisenthal, BS, Bucknell University, Lewisburg, Pennsylvania
Abstract
Objective: To demonstrate a real-life correlation that after the US Food and Drug Administration introduced a boxed warning concerning malignancies to the labeling for topical calcineurin inhibitors, reluctance to use topical calcineurin inhibitors has led to their substitution with other therapies that have their own risks. Participants: An anonymous survey of attendees of the 2007 Fall Clinical Dermatology conference in Las Vegas, Nevada, from October 17–19, 2007. More than 95 percent of attendees were dermatologists; a small number of mid-level practitioners attended as well. Of nearly 700 attendees, the first 504 who agreed to complete the survey were included. Results: More than 40 percent of dermatologists surveyed claimed that more than 20 percent of their atopic dermatitis patients are not adequately controlled since the introduction of the boxed warning. Forty-eight percent claim that more than 20 percent of those patients were adequately controlled with topical calcineurin inhibitors as part of their regimens. Eighty percent of dermatologists surveyed agree that more than 10 percent of those patients were adequately controlled with topical calcineurin inhibitors in their regimens. Conclusion: While caution is usually prudent, the introduction of a boxed warning in the case of topical calcineurin inhibitors has led to the use of treatments that often have greater risks than the topical calcineurin inhibitors that they replaced. (J Clin Aesthetic Dermatol. 2009;2(9):33–39.)
The US Food and Drug Administration (FDA) introduced a boxed warning label in 2005 for the topical calcineurin inhibitors (TCIs) pimecrolimus and tacrolimus. Since that time, there has been a dramatic reduction in the prescriptions written for these drugs. According to the Code of Federal Regulations, a boxed warning is defined and utilized as:
Special problems, particularly those that may lead to death or serious injury, may be required by the Food and Drug Admin-istration to be placed in a prominently displayed box. The boxed warning ordinarily shall be based on clinical data, but serious animal toxicity may also be the basis of a boxed warning in the absence of clinical data. If a boxed warning is required, its location will be specified by the Food and Drug Administration. The frequency of these serious adverse reactions and, if known, the approximate mortality and morbidity rates for patients sustaining the reaction, which are important to safe and effective use of the drug, shall be expressed as provided under the “Adverse Reactions” section of the labeling.[1]
The boxed warning represents the FDA’s highest risk level for prescription medications; however, no written guidelines exist that delineate what events prompt the FDA to issue such a warning.[2,3] Pediatricians began using pimecrolimus and tacrolimus in patients under two years of age despite the fact there had been no clinical trials for infants. On February 15, 2005, the FDA pediatric committee proposed a boxed warning for tacrolimus and pimecrolimus based on the rationale that systemic immunosuppressives are associated with an increased risk of lymphoma and of squamous cell carcinoma (SCC); therefore, topical immunosuppresives may predispose to malignancy. This concern was based on the fact that oral tacrolimus, when used as a transplant drug, was associated with a 10-fold increase in skin cancers and lymphomas, a rise in creatinine levels indicating kidney damage, and an increase in blood pressure. The boxed warning label was implemented based on data relating to oral and not topical tacrolimus or pimecrolimus, the drugs being prescribed for atopic dermatitis.
Methods
The methodology for the survey that developed these questions and subsequent answers and results were reviewed and approved by the Mount Sinai Institutional Review Board.
The data was attained through an anonymous survey of 504 attendees of the 2007 Fall Clinical Dermatology conference in Las Vegas, Nevada, from October 17–19, 2007. More than 95 percent of attendees were dermatologists; a small number of nurse practitioners and physicians assistants attended as well. The survey was distributed and collected prior to the meeting. Of nearly 700 attendees, the first 504 who agreed to complete the survey were included.
In addition to demographic data, the following questions were asked in the survey:
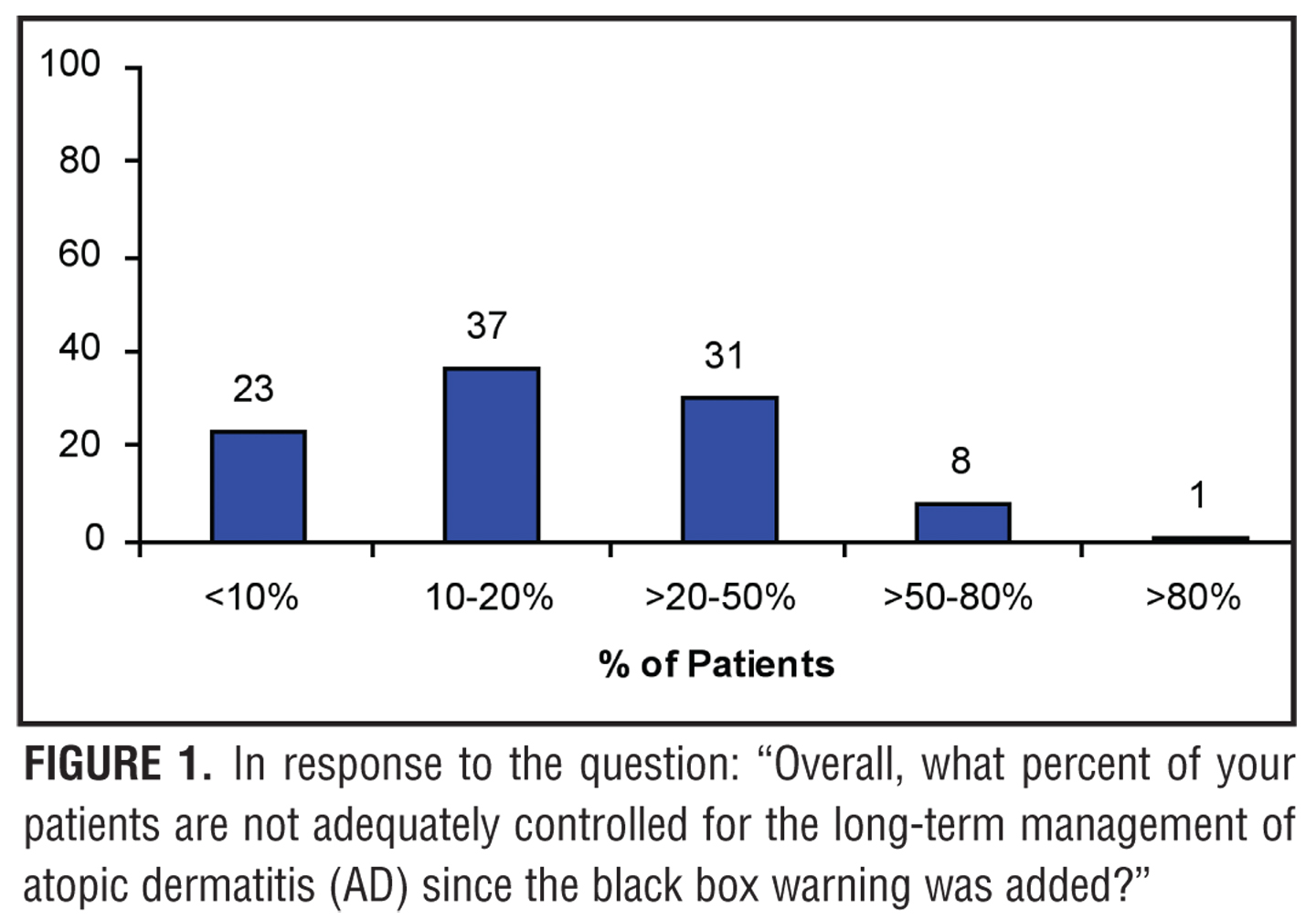
1. Overall, what percent of your patients are not adequately controlled for the long-term management of atopic dermatitis (AD) since the blackbox warning was added?
a) <10%
b) 10–20%
c) >20–50%
d) >50–80%
e) >80%
2. Of those patients who are not adequately controlled, what percent were adequately controlled with topical calcineurin inhibitors (TCIs) as part of their regimens?
a) <10%
b) 10–20%
c) >20–50%
d) >50–80%
e) >80%
3. When treating a typical patient with AD, what treatment regimens have replaced your TCI use? (more than one answer can be circled)
a) Intermittent topical corticosteroids
b) Chronic topical corticosteroids
c) Emollients and other noncorticosteroids
d) Systemic corticosteroids
e) Cyclosporine
f) Mycophenolate mofetil, azathioprine, or other
systemic immunosuppressive agents
g) UVB or PUVA
h) Other
4. When treating a difficult-to-control patient who was previously doing well on a TCI, but now has stopped therapy and as a result cannot be controlled with topical medications, what therapeutic options are you using? (more than one answer can be circled)
a) Intermittent topical corticosteroids
b) Chronic topical corticosteroids
c) Emollients and other noncorticosteroids
d) Systemic corticosteroids—if so, have
you needed more than one course? How many?
e) Cyclosporine
f) Mycophenolate mofetil, azathioprine, or other
systemic immunosuppressive agents
g) UVB or PUVA
h) Other
Results
Of the dermatologists who responded to the survey, 15 percent have been practicing for 1 to 5 years, 21 percent for 6 to 10 years, 13 percent for 11 to 15 years, 26 percent for 16 to 25 years, and 25 percent for 26 or more years. Forty percent have a solo practice, 37 percent are in a private dermatology group, 13 percent are involved in a private multispecialty group, six percent are associated with academic medicine or research, and four percent participate in a health maintenance organization (HMO) or military medical setting. Six percent see less than 50 patients per week, 20 percent see 51 to 100 patients per week, 37 percent see 101 to 150 patients per week, 23 percent see 151 to 200 patients per week, and 14 percent see 201 or more patients per week. Two percent see patients for 10 hours or less per week, two percent for 11 to 15 hours per week, five percent for 16 to 20 hours per week, 21 percent for 21 to 30 hours per week, 50 percent for 31 to 40 hours per week, 15 percent for 41 to 50 hours per week, four percent for 51 to 60 hours per week, and less than one percent see patients for 61 hours or more per week. Sixteen percent of the physicians live in the northeastern United States, 16 percent live in the midwestern United States, 12 percent live in the southeastern United States, 26 percent live in the southwestern United States, seven percent live in the northwestern United States, 18 percent live on the Pacific coast of the United States, three percent live in Canada, and two percent practice outside of Canada or the United States.
In response to the question: “Overall, what percent of your patients are not adequately controlled for the long-term management of atopic dermatitis (AD) since the black box warning was added?”, 23 percent of dermatologists surveyed said less than 10 percent of their patients, 37 percent said 10 to 20 percent of their patients, 31 percent said >20 to 50 percent of their patients, eight percent said >50 to 80 percent of their patients, and less than one percent of dermatologists said >80 percent of their patients (Figure 1).
{kind=link}
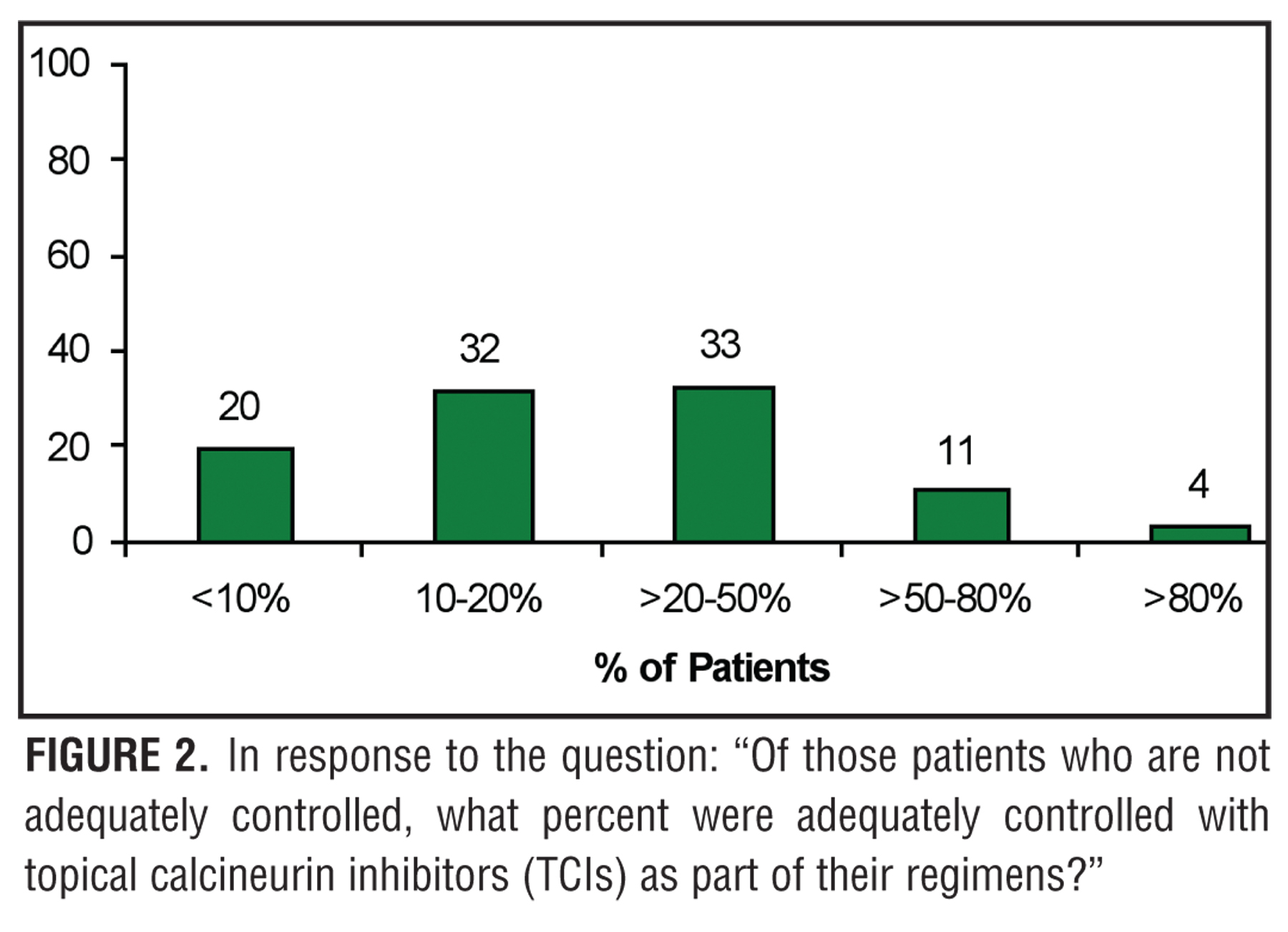
In response to the question: “Of those patients who are not adequately controlled, what percent were adequately controlled with topical calcineurin inhibitors (TCIs) as part of their regimens?”, 20 percent of dermatologists surveyed said less than 10 percent of their patients, 32 percent said 10 to 20 percent of their patients, 33 percent said >20 to 50 percent of their patients, 11 percent said >50 to 80 percent of their patients, and four percent of dermatologists said >80 percent of their patients (Figure 2).
{kind=link}
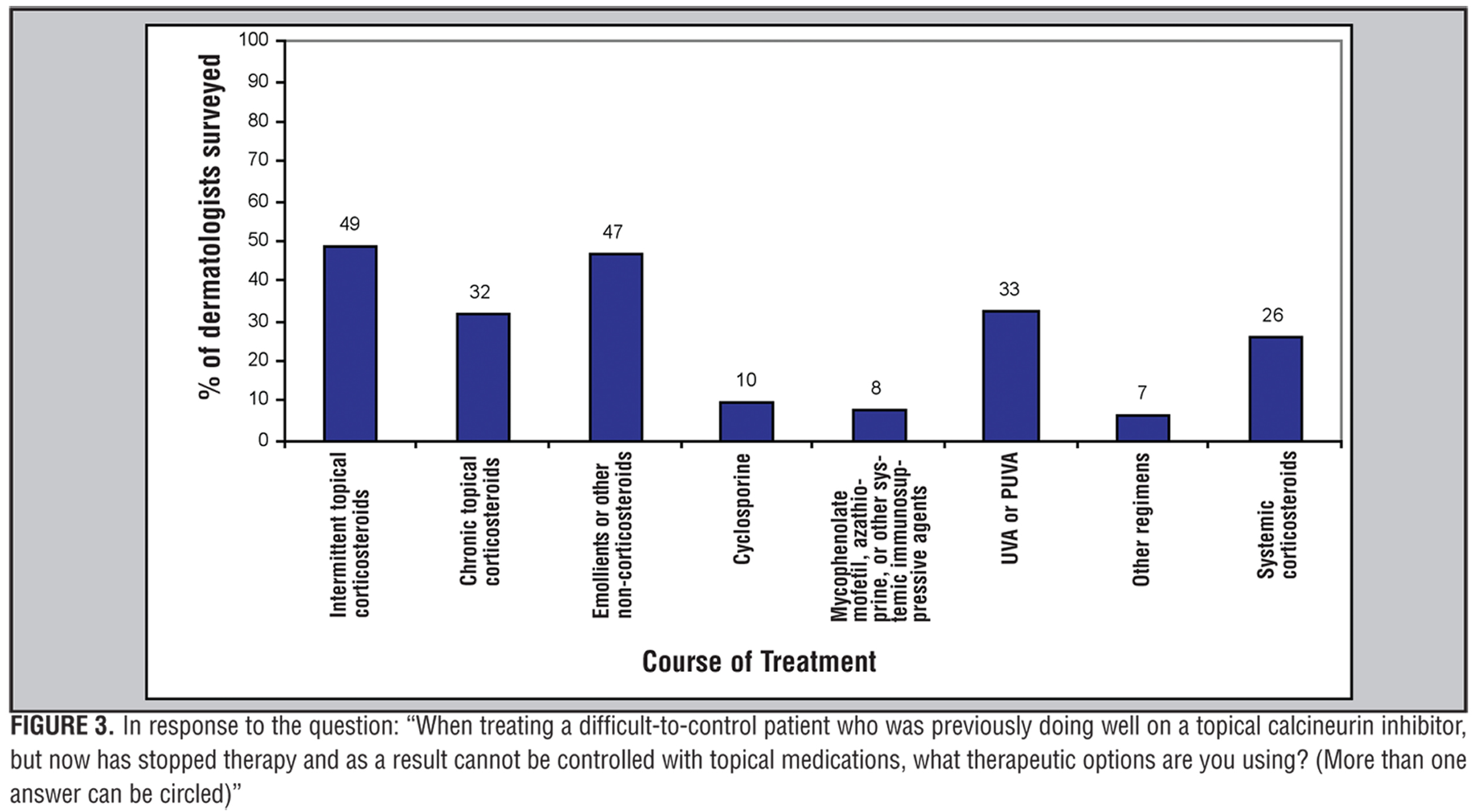
Responses to the question: “When treating a difficult-to-control patient who was previously doing well on a TCI, but now has stopped therapy and as a result cannot be controlled with topical medications, what therapeutic options are you using? (more than one answer can be circled)” are shown in Figure 3. Of the 26 percent who said they prescribed systemic corticosteroids (Figure 3), eight doctors (1.6%) said they prescribed one course, 20 (4%) prescribed two courses, 14 (2.8%) prescribed three courses, one (0.2%) prescribed four courses, one (0.2%) prescribed five courses, and one (0.2%) dermatologist surveyed prescribed >10 courses.
{kind=link}
Discussion
The FDA boxed warning for TCIs states that: “Although a causal relationship has not been established, rare cases of malignancy (e.g., skin and lymphoma) have been reported in patients treated with topical calcineurin inhibitors …” Because of the stringent requirements associated with the addition of boxed warnings, the response of news media and the public was one of great alarm. For example, the headline at www.CNN.com on January 19, 2006, read, “Want to Treat Eczema? Beware of Cancer.”[6] The impact on patient care was dramatic as reflected not only in the reduction in prescriptions of the two TCIs, but also in the results of this survey presented herein.
Atopic dermatitis is a chronic condition that can have severe impact on quality of life. Control of atopic dermatitis can be challenging. More than 40 percent of dermatologists surveyed claimed that more than 20 percent of their atopic dermatitis patients are not adequately controlled since the introduction of the boxed warning. Forty-eight percent claim that more than 20 percent of those patients were adequately controlled with TCIs as part of their regimens. Eighty percent of dermatologists surveyed agree that more than 10 percent of those patients were adequately controlled with TCIs in their regimens.
Because patients and parents of patients are frightened by the literature accompanying TCIs, dermatologists have had to resort to alternative therapies that carry risks that are in some cases theoretically more dangerous. Of those surveyed, 35 percent said they prescribed chronic topical corticosteroids; 12 percent said they prescribed systemic corticosteroids; four percent said they prescribed cyclosporine; four percent said they prescribed mycophenolate mofetil, azathioprine or other systemic immunosuppressive agents; and 20 percent said they prescribed ultraviolet B (UVB) or psoralen plus UVA (PUVA) in place of TCIs for atopic dermatitis (Figure 4).
{kind=link}
Since the boxed warning has resulted in a shift in therapies from TCIs to serious systemic therapies or phototherapy, does available evidence support the addition of a boxed warning to the package labels for topical tacrolimus ointment and pimecrolimus cream?
At the FDA hearings, substantial data was presented.[7] It took 258 times the maximum human exposure of pimecrolimus administered orally before lymphoma was detected in a mouse model. When tacrolimus and pimecrolimus were dissolved in an ethanol vehicle that enhanced penetration through the skin in rodent models, lymphomas were detected at 26 times the maximum human exposure of tacrolimus and 47 times the maximum human exposure of pimecrolimus. In a monkey model at more than 35 times the maximum human exposure of oral pimecrolimus, immune-related lymphoproliferative disease was detected.
In the new drug applications for topical tacrolimus and pimecrolimus, photocarcinogenesis studies demonstrating an increase in skin cancers were submitted, but both studies were flawed because the vehicles alone accelerated carcinogenesis. Additional data was presented that dimethylbenzanthracene, a tumor initiator, and 12-O-tetradecanoylphorbol-13-acetate (TPA), a tumor promoter, markedly increase skin tumor formation in the presence of tacrolimus. However, most of the tumors were papillomas, which are uncommon in humans and are benign. Eight and a half percent of the tumors were, however, SCCs and these were increased in mice exposed to tacrolimus along with the carcinogens.[8] Conversely, Tran et al demonstrated that TCIs filter UVB and decrease production of UVB-induced thymine dimers in hairless mice.[9] In human studies, Naylor et al examined data from 9,813 adult and pediatric patients with atopic dermatitis who applied tacrolimus ointment twice daily for a mean of 208 days and a maximum observation period of 1,479 days. Thirteen were diagnosed with nonmelanoma skin cancer, and of the 13, 12 were over the age of 40 and one was 26 years of age. Ten of the 13 were diagnosed within 90 days of starting tacrolimus ointment, suggesting that the skin cancer was not caused by the tacrolimus, but unmasked by it. Seven of the 13 skin cancers occurred on sites where the tacrolimus ointment had not been applied. Most of the patients who developed skin cancers had other risk factors. All were Caucasian. Seven of the skin cancers occurred in areas of sun exposure, such as the face, neck, and hands. Seven of the patients had previously had nonmelanoma skin cancers and two had other risk factors such as methotrexate, phototherapy, and oral cyclosporine. When compared to large databases of patients, the frequency of skin cancer found in this study was not increased over that which would have been expected.[10]
In terms of the numbers of patients studied and the duration of studies, TCIs have also proven to be safe. Koo et al reported the results of tacrolimus ointment treatment in 8,000 patients.[11] Hanifin et al studied patients for up to four years.[12] In clinical trials of tacrolimus ointment involving more than 19,000 patients including 7,600 pediatric patients, there was no increased risk of systemic infection, no increased risk of malignancy, and no impairment of systemic immune response demonstrated. Similarly, pimecrolimus has been studied in 1,133 infants for up to two years.[13] In a review of double-blind, placebo-controlled trials, 19,000 treated patients were compared to 4,000 controls.[7] The frequency of malignancy was higher in the control group than in the patients treated with pimecrolimus.
Over the past three decades, it has become clear in transplant populations that oral calcineurin inhibitors are safer than oral systemic steroids. It is therefore interesting that the majority of dermatologists and other healthcare providers surveyed have substituted TCIs with topical corticosteroids. Logically, one should then ask which active ingredient is absorbed more. In a study comparing absorption of topical pimecrolimus and tacrolimus to topical betamethasone valerate, clobetasol propionate, and diflucortolone-valerate, the corticosteroids were absorbed 10 times more than tacrolimus ointment and 70 to 100 times more than pimecrolimus cream.[14] Arellano et al looked at the risk of lymphoma following exposure to calcineurin inhibitors and steroids in patients with atopic dermatitis. Oral corticosteroids were associated with a 1.5 odds ratio for the development of lymphoma. The odds ratio for superpotent topical corticosteroids was 1.2 and for low potency topical corticosteroids 1.1. The odds ratio for pimecrolimus cream or tacrolimus ointment was 0.8 and for those using concomitant topical corticosteroids, pimecrolimus and tacrolimus the odds ratio was 1.0.[15]
In summary, there is little evidence that TCIs cause systemic effects. Absorption is infrequent, at low levels, and not sustained. Studies have failed to demonstrate an increase in blood pressure or elevations of blood urea nitrogen or creatinine, which would be signs of systemic effects of calcineurin inhibitors. There has not been a demonstration of increased malignancy with TCIs although increased skin cancer and lymphomas certainly occur in patients treated with oral calcineurin inhibitors.[16]
Boxed warnings for TCIs were not based on the extensive clinical data available for those agents.[17] Introduction of the boxed warning has been followed by substitution of TCIs with topical corticosteroids and even systemic corticosteroids, systemic calcineurin inhibitors, other immunosuppressive agents, or phototherapy. While caution is usually prudent, the introduction of a boxed warning in the case of TCIs has led to the use of treatments that often have greater risks than the TCIs that they replaced. Simply stated, evidence clearly shows that there is not a risk of cancer with TCIs. Because of the black box warning, patients have been switched from safer treatments (TCIs) to treatments that are more likely to cause cancer.
References
1. Code of Federal Regulations. Title 21: Food and Drugs. Volume 4, Part 201.57(e). http://a257.g.akamaitech. net/7/257/2422/14mar20010800/edocket.access.gpo.gov/cfr_2002/aprqtr/pdf/21cfr201.57.pdf. Accessed December 9, 2007.
2. Beach JE, Faich GA, Bormel FG, et al. Boxed warnings in prescription drug labeling: results of a survey of 206 drugs. Food Drug Law J. 1998;53:403–411.
3. Wagner AK, Chan KA, Dashevsky I, et al. FDA drug prescribing warnings: is the boxed warning half empty or half full? Pharmacoepidemilo Drug Saf. Epub 18 Nov 2005. http://www3.interscience.wiley.com/cgi-bin/fulltext/ 112141666/PDFSTART. Accessed December 9, 2007.
4. Berg D, Otley CC. Skin cancer in organ transplant recipients: epidemiology, pathogenesis, and management. J Am Acad Dermatol. 2002;47(1):1–17.
5. Boubenider S, Hiesse C, Goupy C, et al. Incidence and consequences of post-transplantation lymphoproliferative disorders. J Nephrol. 1997; 10(3):136–145.
6. Want to Treat Eczema? Beware of Cancer. www.CNN.com. Accessed January 19, 2006.
7. Anonymous. New warnings for two eczema drugs. www.fda.gov/fdac/departs/2006/206_ipd.html#eczema. Accessed April 2, 2006.
8. Niwa Y, Terashima T, Sumi H. Topical application of the immunosuppressant tacrolimus accelerates carcinogenesis in mouse skin. Br J Dermatol. 2003;149(5):960–967.
9. Tran C, Lübbe J, Sorg O, et al. Topical calcineurin inhibitors decrease the production of UVB-induced thymine dimers from hairless mouse epidermis. Dermatology. 2005;211(4):341–347.
10. Naylor M, Elmets C, Jaracz E, et al. Non-melanoma skin cancer in patients with atopic dermatitis treated with topical tacrolimus. J Dermatolog Treat. 2005;16(3):149–153.
11. Koo JY, Fleischer AB Jr, Abramovits W, et al. Tacrolimus ointment is safe and effective in the treatment of atopic dermatitis: results in 8000 patients. J Am Acad Dermatol. 2005;53(2 Suppl 2):S195–S205.
12. Hanifin JM, Paller AS, Eichenfield L, et al. US Tacrolimus Ointment Study Group. Efficacy and safety of tacrolimus ointment treatment for up to four years in patients with atopic dermatitis. J Am Acad Dermatol. 2005;53(2 Suppl 2):S186–S194.
13. Paul C, Cork M, Rossi AB, et al. Safety and tolerability of 1% pimecrolimus cream among infants: experience with 1133 patients treated for up to 2 years. Pediatrics. 2006;117(1):e118–e128.
14. Billich A, Aschauer H, Aszódi A, et al. Percutaneous absorption of drugs used in atopic eczema: pimecrolimus permeates less through skin than corticosteroids and
tacrolimus. Int J Pharm. 2004;269(1):29–35.
15. Arellano FM, Wentworth CE, Arana A, et al. Risk of lymphoma following exposure to calcineurin inhibitors and topical steroids in patients with atopic dermatitis. J Invest Dermatol. 2007;127(4):808–816.
16. Opelz G, Döhler B. Lymphomas after solid organ transplantation: a collaborative transplant study report. Am J Transplant. 2004;4(2):222–230.
17. Langley RG, Luger TA, Cork MJ, et al. An update on the safety and tolerability of pimecrolimus cream 1%: evidence from clinical trials and post-marketing surveillance. Dermatology. 2007;215(Suppl 1):27–44.