Mark S. Nestor, MD, PhD; Voluntary Associate Professor, Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, Florida; Director of the Center for Clinical and Cosmetic Research and the Center for Cosmetic Enhancement, Aventura, Florida; Matthew B. Zarraga, DO, Dermatology Fellow, The Center for Clinical and Cosmetic Research, Aventura, Florida
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Background: Incidence of nonmelanoma skin cancer and actinic keratoses appears to be increasing worldwide due to increasing levels of ultraviolet radiation, lifestyle changes, and an aging population. Because of its demographics and geographic location, the population of South Florida is at risk for high rates of nonmelanoma skin cancer and actinic keratoses. Objective: To determine the incidence of nonmelanoma skin cancer and actinic keratoses in two populations in South Florida by measuring treatments by dermatologists in health maintenance organization gatekeeper populations. Methods: The incidence of nonmelanoma skin cancer and actinic keratoses in South Florida was determined by evaluating the number of nonmelanoma skin cancers and actinic keratoses treated by dermatologists (Current Procedural Terminology [CPT] Code Analysis) in two health maintenance organization populations; “commercial” (age 0–65, mean 27) and Medicare (age 65+, mean 68) in the calendar year 1996. Results: The incidence of treatment of nonmelanoma skin cancer was 466.5 per 100,000 people per year in the “commercial” (age 0 to 65) population and 10,689.8 per 100,000 people per year in the Medicare age population. The incidence of treated actinic keratoses was 4,464.6 per 100,000 people per year and 110,450.3 in each population respectively. Conclusion: The studied populations in South Florida appear to have some of the highest incidence rates of nonmelanoma skin cancer in the world and extremely high rates of actinic keratoses. The findings suggest that there is an epidemic of nonmelanoma skin cancer in the South Florida community, which has significant implications for the future medical needs of both “commercial” and Medicare-age populations.
(J Clin Aesthet Dermatol. 2012;5(4):20–24.)
Nonmelanoma skin cancers (NMSC), including basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and squamous cell carcinoma in situ (SCC IS), are the most common forms of cancer in the United States.[1–3] The most recent, peer-reviewed, published, national estimate was done in 2006. It was estimated that the total number of NMSCs in the United States population in 2006 was 3,507,693, while the total number of persons in the United States treated for NMSC was 2,152,500.[1,2] The exact incidence of NMSC is unknown since the condition is not usually reported to cancer registries; however, over the last 20 years, a number of studies indicate a dramatic worldwide increase in the numbers of cases of NMSC.[1–6] This increase is thought to be in large part associated with increased levels of ultraviolet radiation (UVR) caused by the depletion of the world’s ozone layers7 as well as lifestyle changes.[8] These risk factors are particularly relevant in the case of SCC where increasing incidence appears to be more closely associated with UVR exposure and an aging population.[9,10] This may be best exemplified by the highest incidence of NMSC documented that has been observed in Australia.[11]
Because of the increased relative risk of NMSC associated with geographic locations, such as Florida,[12] it is vital that we clarify how multiple risk factors including age and geographic location affect incidence of NMSCs as well as AKs. The incidence of AKs is important to study because of the documented conversion of AK to SCC coupled with the increased incidence of SCC and SCC IS.[13] This study looks at one measure of incidence of NMSCs and AKs, those specifically that were treated by dermatologists in gatekeeper health maintenance organization (HMO) populations.
Methods
The incidence data for both NMSC and AK are derived from treatment data from two stable HMO populations located in Dade, Broward, and Palm Beach Counties in South Florida. During a two-year period from late 1995 through mid 1997, a dermatology Independent Practice Association (IPA) was responsible for providing and adjudicating dermatology services for two capitated HMO populations.
The first patient population was a “commercial” gatekeeper HMO population with an age range of 0 to 65 years and an average age of 27 years. During the period from January through December 1996, the overall HMO population averaged 110,000 patients. Approximately 90 percent of individuals in the HMO were covered either through employment or family members’ arrangements. A gatekeeper model was employed such that all patients had to be seen by their primary care physicians (PCP) before being referred to dermatologists. They were referred for specific problems and their referral periods ranged from one visit to a period of up to 3 to 6 months. Patients could be followed up during that time without obtaining further authorization from the PCP. The patient had a copayment associated with the office visit, but there was no additional copayment paid by the patient for biopsies or any other surgical procedures. Because of the gatekeeper system, suspicious lesions were initially assessed by the PCP before referral to dermatologists or other specialists for evaluation and treatment. These patients did not have a point-of-service option with this plan and it is assumed that 90 percent of the total care was supplied by network physicians.
The second population studied was a Medicare gatekeeper HMO population. The age range was generally 65 and older; however, approximately eight percent were considered Medicare disabled and as a result, were less than age 65. The average age in this population was approximately 68 years. In the study period between January and December 1996, there was an average of 12,000 HMO members and 100 percent of these were covered as Medicare HMO patients. The gatekeeper system used was the same as with the “commercial” HMO population; the patients did not have any point-of-service option, and there was no copayment associated with either visits or surgical procedures. It was assumed that 95 percent of all medical care was delivered through this plan.
The dermatology physician panel consisted of 54 board-certified dermatologists situated throughout the tri-county area and included five Fellowship-trained Mohs micrographic surgeons. All dermatopathology specimens were sent for interpretation to a single national lab, whereby 90 to 95 percent of them were evaluated by a Fellowship-trained dermatopathologist.
This study investigates the incidence of NMSC based on CPT code evaluations of procedures performed by network dermatologists. Treated NMSCs included BCC, SCC, and SCC IS. Treatment incidence was based on CPT codes in use in 1996 that included malignant lesion excision codes 11200 through 11240, malignant lesion destruction codes 12500 through 12670, and Mohs micrographic surgery code 12304. Each month, the network compiled the total number of skin cancers removed or destroyed in each population by all of the dermatologists in the network. In this way, incidence figures dated represent the total numbers of treated skin cancers rather than the number of individuals in the population with NMSC. The data included only NMSCs treated by network dermatologists and did not include those that were biopsied but not treated, treated by PCPs or other specialists in the network, or treated out of network.
The frequency of specific types of NMSCs, those being SCC, BCC, and SCC IS, was evaluated in order to determine the relative frequencies within the given populations. Unfortunately, because of problems with the national laboratory computer system, the authors were not able to obtain overall data from the entire HMO population. Therefore, they looked at the breakdown of specific numbers of BCC, SCC, and SCC IS for two physicians in the plan as representative of the population. They evaluated the dermatopathology diagnoses for all biopsy-proven and treated skin cancers in both the “commercial” and “Medicare” HMO insurance plans for the 12 months included in 1996. The numbers were then extrapolated in order to estimate the individual types of tumors that comprised NMSCs.
The incidence of AKs in this study is defined as the numbers of AKs destroyed or removed by network dermatologists based on CPT code evaluations. The AMA CPT destruction codes 17000 through 17002 linked to a diagnosis of 702.0 were evaluated. This did not include those AKs that were biopsied but not treated, treated by PCPs or other specialists in the network, or treated out of network.
Each month the total number of NMSCs and AKs that were treated were tallied. The population incidence was calculated each month based on the exact HMO population for that month and this was averaged over the 12 months in 1996. The incidence rate for both NMSCs and AKs was then mathematically extrapolated to yield incidence per 100,000 people per year.
Results
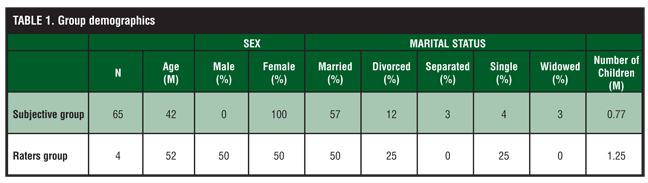
The results of the estimated incidence of NMSCs in South Florida in 1996 are outlined in Table 1. As noted, this was divided into the two populations of “commercial” HMO patients (age 0–65) and Medicare HMO patients, who for the most part were 65 years or older. The incidence data for NMSCs including BCCs, SCCs, and SCCs IS is 466.5 per 100,000 people per year in the “commercial” HMO population and 10,689.8 per 100,000 people per year in the Medicare age population.
{kind=link}
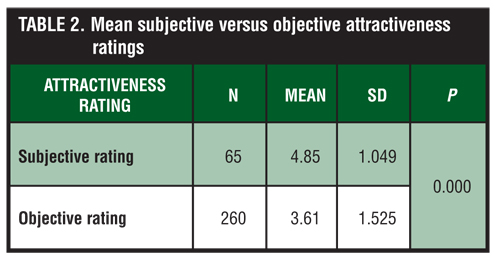
The estimated incidence of AKs treated in this population is outlined in Table 2. Based on the treatment codes, 17000 series, the number of AKs treated in the “commercial” HMO population (ages 0 to 65) was 4,764.6 per 100,000 people per year and in the Medicare HMO population, this was 110,450.3 per year.
{kind=link}
The specific frequencies of the three types of NMSCs are shown in Figure 1. Approximately 28 percent of the tumors in the sample were BCCs, 35.5 percent were SCCs, and 36.7 percent were SCCs IS.
Discussion
The results of this study indicate that the estimated incidence of NMSCs and AKs in South Florida may be among the highest recorded incidences in the world. Even though the data was based on treatment of diagnosed NMSC in 1996, the number of treated NMSC has increased in subsequent years based on CMS data.[2] Although this study only takes into account those NMSCs that were treated by dermatologists under HMO network conditions, the results are meaningful for a number of reasons. First, the study was based on a stable known HMO population rather than on a global population statistic. Population statistics can be difficult to interpret and may be confounded by unknowns, such as immigration and migration of the population.[14] Reliability of the stable HMO population is critical in that each month the exact numbers of individual members within a given plan were known and the vast majority of their care was being provided by the HMO. While there are few studies comparing the demographic makeups of HMO populations to the population at large, it is thought that the patient population of HMOs, especially Medicare HMOs, where patients have a clear choice of healthcare services, tends to be healthier than the population at large.[15] The cause of this is twofold: First, sicker patients feel they need more choice and do not wish to switch individual physicians, and second, there may be some selection pressures from the HMO. It is not clear whether this has any implication on the incidence of NMSCs in the HMO population versus the population at large, but it may favor the exclusion of patients from HMOs who have severe actinic damage and/or large numbers of skin cancers. If this were the case, it would tend to cause an underestimation of the actual numbers of NMSCs. Additionally, there is a significant advantage in having a stable number of network dermatologists serving an HMO through an IPA. IPA physicians actively participate in quality assurance and utilization reviews, which may promote appropriate utilization of procedures and dissuade inappropriate utilization of services.[16]
While rates of both NMSCs and AKs in this study appear to be some of the highest in the world, it is important to note that these rates do not include those NMSCs or AKs that were biopsied and not treated, treated by physicians other than dermatologists including PCPs and other specialists, and those treated outside the network. These exclusions imply that the true incidence of NMSC is significantly higher than this study shows. Furthermore, even though the sample was small, the fact that the vast majority of tumors were SCCs or SCCs IS may indicate that this population has long-term high UVR exposure and damage leading to a higher incidence of SCC type tumors.[9,10] The results suggest that because of the extreme and constant amounts of UVB and UVA exposure and sun damage, South Florida populations may be experiencing damage similar to that seen in psoralen + UVA (PUVA) patients and thereby have a significant increased risk of SCC type tumors.[17,18]
It is often difficult to compare incidence studies derived from databases and population-based studies in the United States and around the world. The problems with comparisons include differences in the inherent population and methods in calculating incidence data as well as effects such as immigration and migration.[13] Surveillance, epidemiology, and end results (SEER) statistics, while indicative of certain melanoma skin cancer rates, do not include statistics for NMSC.[2,19] Other studies compare age-standardized incidence rates, deriving data from populations with varied age groups. Studies of populations in Rochester, Minnesota, reveal an age standardized incidence of 38.8 per 100,000 people per year with the incidence of SCC increasing significantly as the population aged.[20] An earlier study conducted in New Hampshire and Vermont showed that the overall age-adjusted incidence rates of NMSC (including SCC and BCC) were 191 per 100,000 for men and 95 per 100,000 for women.[21] The authors acknowledged that these rates were significantly lower than rates for NMSC for populations residing in southern latitudes in the United States.[21,22] In fact, a study conducted between 1998 and 1999 in New Mexico by Athas et al[23] estimated the age-adjusted incidence rate of SCCs and BCCs to be 1,922.4 per 100,000 people per year.
Worldwide incidence rates for NMSC vary from 136.3 per 100,000 people in the Southeast Netherlands[24] to 102.1 per 100,000 people in South Wales, United Kingdom.[25] The highest recorded rates of NMSCs outside the United States appear to occur in Australia. The adjusted rates of NMSC in Australia, which include SCC and BCC, range from 1,560 per 100,000 people per year in a population of 40- to 60-year old men and women in Western Australia,[26] to a study of populations in Queensland, Australia, which demonstrated rates of 122 and 100 for men and women, respectively, in populations under 40 years of age, 5,861 for men and 3,008 for women in age ranges of 60 to 69 years, and 12,931 for men and 5,120 for women in patients who were 80 years of age.[27] A study conducted between December 1996 and December 1997, in Townsville, Australia, with a population of only 127,000 people, found that age-standardized incidence rates per 100,000 people of BCC were 2,058.3 for men and 1,194.5 for women, while the incidence rates for SCC were 1,332.3 for men and 754.8 for women.[28] Another Australian study conducted by Staples et al[29] in 2002 revealed that the age-standardized rate per 100,000 people for NMSC was 1,170, for BCC was 884, and for SCC was 387.
Based on the differences of populations as well as in the type of NMSC evaluated, it is difficult to draw absolute comparisons to this and worldwide incidence studies. It is apparent, however, that incidence of NMSC in this study indicates that South Florida has one of the highest rates of NMSC in the world, despite the potential of underreporting in this study. Furthermore, as evident from the New Mexico study, the incidence of NMSC in South Florida is much higher than other locations in the United States that have lower latitudes and also experience extensive sun exposure,[23] which clearly gives credence to the emergence of an epidemic of NMSC in South Florida. This may be due in part to differences in behavior and attitude toward tanning or in population demographics.
There have not been any population-based estimates of the frequencies of AKs in the United States. Studies of prevalence have been attempted in Australia and AKs have been estimated to be present on 40 to 50 percent of the population 40 years of age and older.[30–32]
This may be one of the first studies looking at incidence of AKs treated by dermatologists and certainly demonstrates a very high incidence of these premalignant lesions. The data may indicate that although some studies theorize that as few as 1 AK in 1,000 may evolve into a SCC,[31] in populations associated with high levels of UVR exposure, the evolution may be greatly accelerated.
This study gives significant weight to aggressive treatment of early NMSC and premalignant AK lesions in patients in South Florida, which is especially crucial in Medicare age populations that appear to have some of the highest rates of NMSC in the world. The data also supports the recent publication stressing that AK should be treated in order to prevent conversion into SCCs.[33–35] Treatment of AKs as well as the treatment of small, early NMSC greatly reduces morbidity and possibly mortality and certainly proves to be cost-effective. Overall, this study suggests an epidemic of NMSCs and AKs in the South Florida community and may have significant implications for the future dermatological needs of both “commercial” and Medicare age populations.
References
1. American Cancer Society. Cancer Facts and Figures 2011. http://www.cancer.org/Research/CancerFactsFigures/CancerFactsFigures/cancer-facts-figures-2011. Accessed October 3, 2011.
2. Rogers HW, Weinstock MA, Harris AR, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146(3):283–287.
3. Silverberg E, Boring CC, Squires TS. Cancer statistics, 1990. CA Cancer J Clin. 1990;40(1):9–26.
4. Glass AG, Hoover RN. The emerging epidemic of melanoma and squamous cell skin cancer. JAMA. 1989;262(15): 2097–2100.
5. Kaldor J, Shuff D, Young B, Dwyer T, Wang YG. Nonmelanoma skin cancer: ten years of cancer-registry-based surveillance. Int J Cancer. 1993;53(6):886–891.
6. Marks R. The epidemiology of nonmelanoma skin cancer; who, why and what we can do about it. J Dermatol. 1995;22(11):853–857.
7. Urbach F. Causes and effects of stratospheric ozone reduction; an update. J Am Acad Dermatol. 1982;7(2): 271–273.
8. Weinstock M. The epidemic of squamous cell carcinoma. JAMA. 1989;262(15):2138–2140.
9. Green A, Battistutta D. Incidence and determinants of skin cancer in a high risk Australian population. Int J Cancer. 1990;46(3):356–361.
10. Serrano H, Scotto J, Shornick G, Fears TR, Greenberg ER. Incidence of nonmelanoma skin cancer in New Hampshire and Vermont. J Am Acad Dermatol. 1991;24(4):574–579.
11. Leiter U, Garbe C. Epidemiology of melanoma and nonmelanoma skin cancer—the role of sunlight. Adv Exp Med Biol. 2008;624:89–103.
12. Grodstein F, Speizer FE, Hunter DJ. A prospective study of incident squamous call carcinoma of the skin in the nurses’ health study. J Natl Cancer Inst. 1995;87(14):1061–1066.
13. Goldberg LH, Mamelak AJ. Review of actinic keratosis. Part I: etiology, epidemiology and clinical presentation. J Drugs Dermatol. 2010;9(9):1125–1132.
14. Glass AG, Hoover RH. The emerging epidemic of melanoma and squamous cell cancer. JAMA. 1989;262(15):2097–2100.
15. Hellinger FJ. Selection bias in HMOs and PPOs: a review of the evidence. Inquiry. 1995;32(2):135–142.
16. Nestor MS. Dermatology independent practice associations. Arch Dermatol. 1996;132(9):1099–1101.
17. Maier H, Schemper M, Ortel B, Binder M, Tanew A, Honigsmann H. Skin tumors in photochemotherapy for psoriasis: a single-center follow-up of 496 patients. Dermatology. 1996;193(3):185–191.
18. Lever LR, Farr PM. Skin cancers or premalignant lesions occur in half of high-dose PUVA patients. Br J Dermatol. 1994;131(2):215–219.
19. Young JL, Percy CL, Asire AJ. Surveillance, epidemiology and end results; incidence and mortality date, 1973–1977. Natl Cancer Inst Monogr. 1981;(57):1–1082.
20. Chuang TY, Popescu NA, Su WP, Chute CG. Squamous cell carcinoma. A population based incidence study in Rochester, Minn. Arch Dermatol. 1990;126(2):185–188.
21. Serrano H, Scotto J, Shornick G, Fears, T, Greenberg ER. Incidence of nonmelanoma skin cancer in New Hampshire and Vermont. J Am Acad Dermatol. 1991;24(4):574–579.
22. Eide MJ, Weinstock MA. Epidemiology of skin cancer. In: Rigel DS et al, eds. Cancer of the Skin. Saunders; 2011:44–55.
23. Athas WF, Hunt WC, Key CR. Changes in nonmelanoma skin cancer incidence between 1977–1978 and 1998-1999 in Northcentral New Mexico. Cancer Epidemiol Biomarkers Prev. 2003;12(10):1105–1108.
24. Coebergh JWW, Neumann HAM, Vrints LW, et al. Trends in the incidence of nonmelanoma skin cancer in the SE Netherlands 1975–1988: a registry-based study. Br J Dermatol. 1991;125(4):353–359.
25. Roberts DL. Incidence of nonmelanoma skin cancers in West Glamorgan, South Wales. Br J Dermatol. 1990;122(3): 399–403.
26. Kricker A, English DR, Randell PL, et al. Skin cancer in Geraldton, Western Australia: a survey of incidence of prevalence. Med J Aust. 1990;152(8):399–407.
27. Stenbeck KS, Balanda KP, Williams MJ, et al. Patterns of treated nonmelanoma skin cancer in Queensland—the region with the highest incidence of rates in the world. Med J Aust. 1990;153(9):511–515.
28. Buettner PG, Raasch BA. Incidence rates of skin cancer in Townsville, Australia. Int J Cancer. 1998;78(5):587–593.
29. Staples MP, Elwood M, Burton RC, et al. Non-melanoma skin cancer in Australia: the 2002 national survey and trends since 1985. Med J Aust. 2006;184(1):6–10.
30. Marks R, Julley D, Dorevitch AP, Selwood TS. The incidence of nonmelanocytic skin cancer in an Australian population: results of a five year prospective study. Med J Aust. 1989;150(9):475–478.
31. Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma in the skin: a prospective study. Lancet. 1988;1:795–807.
32. Schwartz R, Bridges T, Butani A, et al. Actinic keratosis: an occupational and environmental disorder. J Eur Acad Deramatol Venereol. 2008;22:606–615.
33. Callan JP, Bickers DR, Moy RL. Actinic keratoses. J Am Acad Dermatol. 1997;36(4):650–653.
34. Holmes C, Foley P, Freeman M, Chong AH. Solar keratosis: epidemiology, pathogenesis, presentation and treatment. Australas J Dermatol. 2007;48(2):67–74; quiz 75–76.
35. Takata M, Saida T. Early cancers of the skin: clinical, histopathological, and molecular characteristics. Int J Clin Oncol. 2005;10(6):391–397.