Peter Saitta, DO, Department of Dermatology, Oakwood Southshore Medical Center, Detroit, Michigan; David E. Cohen, MD, MPH, Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, New York; Darrell Rigel, MD, Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, New York; Steven K. Grekin, DO, Department of Dermatology, Oakwood Southshore Medical Center, Detroit, Michigan; and Ronald Brancaccio, MD, Ronald O. Perelman Department of Dermatology, New York University School of Medicine, New York, New York.
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Purpose: Mortalities due to skin cancer are escalating, but early detection via skin examinations can be beneficial. To date, dermatologists have not been isolated as a high-risk population for developing skin cancer, although some evidence suggests that they are a high-risk group. Therefore, the specific aims of this study were to measure the frequency at which dermatologists perform self-skin examination and receive full-body skin examination. Patients and methods: A sample of 476 respondents provided data for this cross-sectional, nine-item survey, which was e-mailed to all registered members in the American Society for Dermatologic Surgery. The initial invitation was sent in the summer of 2007, with reminders sent at four and eight weeks. E-mails contained a unique identifier, and each member could only respond once to the survey sent to that particular e-mail address. Results: 71.7 percent of the respondents reported that they routinely gave themselves a self-skin examination, 25.4 percent reported a monthly exam, 24.5 percent every six months, 17.2 percent once per year, and 4.6 percent every five years. Performing a self-skin examination was not related to age, gender, or history of skin malignancy. Seventy-six percent of all respondents never had a full-body skin examination conducted by another dermatologist, which persisted when analyzed by age (p=0.0490) and gender (p=0.0184). Conclusion: Dermatologists are more likely to perform self-skin examination rather than visit another dermatologist for a full-body skin examination. (J Clin Aesthet Dermatol. 2011;4(6):20–24.)
The incidence of skin cancer is rising with more than one million new cases reported per year,[1] making it the most common malignancy in the United States.[2] In 2005, there were an estimated 59,580 reports of malignant melanoma (MM) and 10,590 deaths.[1,3] The remaining cases are attributed to basal cell carcinomas (BCC) and squamous cell carcinomas (SCC), which have been implicated as a risk factor for developing MM. In a case control study, Marghoob et al[4] found that individuals with BCC or SCC have an increased relative risk for developing MM, a conclusion supported by previous studies.[5–8] It is clear that the rising incidence of skin cancer warrants attention.
Recognizing changes in skin growths or the appearance of new growths is one way to detect skin cancer early. Early detection may decrease mortality and morbidity, lessen possible physical disfigurement, and prevent extensive treatment costs.[9] Since 1985, the American Academy of Dermatology (AAD) has provided free skin cancer screenings as part of its National Melanoma/Skin Cancer Screening program, thereby stressing the importance of early detection. It has been demonstrated that early detection via full-body skin examination (FBSE) results in a high five-year survival rate in those diagnosed with MM.[10–14]
To date, dermatologists have not been isolated as a high-risk population for developing skin cancer, although some evidence suggests that they may be a high-risk group.[4,15–31] Therefore, the authors studied the frequency of skin cancer as well as the rate of self-skin examination (SSE) and FBSE in dermatologists.
Methods
Design and participants. The sample of this cross-sectional e-mail survey comprised members of the American Society for Dermatologic Surgery (ASDS), including dermatologists from the United States and Canada, as well as dermatology residents and fellows. Names and e-mail addresses of 2,845 eligible physicians were obtained from the 2007 ASDS e-mail roster. Ethical clearance for this study was obtained from the New York University School of Medicine investigational review board (approval #06-595 and approved on 8-17-06).
Survey instrument. The final survey instrument was vetted by several dermatologists for clarity and ease of navigation and ultimately resulted in nine questions. Six of these questions requested participants report the following: 1) how frequently they received FBSE from other dermatologists; 2) how frequently they practiced SSE; 3) their personal history, if any, of precancerous and cancerous skin lesions; 4) the types of patient-education materials that they routinely used in their own practices; 5) how frequently they volunteered in skin cancer screening programs; and 6) what they perceived to be the biggest barriers to participation in such programs. SSE (self exam) and FBSE (exam by another dermatologist) were defined as examinations of the entire integument from head to toe, including the oral mucosa.
Basic demographic data including gender, age group, and the first three numbers of zip code were collected. Demographic variables were categorized as follows: gender (male, female) and age (25–35, 36–45, 46–55, 56–65, 66–75, other).
Data collection. An invitation to participate in this nine-item survey was e-mailed to all registered members of the ASDS with e-mail addresses. The e-mail contained a hyperlink to access the web page housing the survey instrument, which was developed by web designers and computer technicians. The initial invitation was sent in the summer of 2007, with reminders sent at Weeks 4 and 8. E-mails contained a unique identifier, and each member could only respond once to the survey sent to that particular e-mail. Participation was on a volunteer basis, and no incentives were offered for completion of the survey.
Statistical analysis. All statistical analyses were performed using the Statistical Package for the Social Science version 10.0. Standard descriptive statistics including percentages were computed. Chi square tests were used to examine the relationships between response variables. P values of less than 0.05 were considered significant.
RESULTS
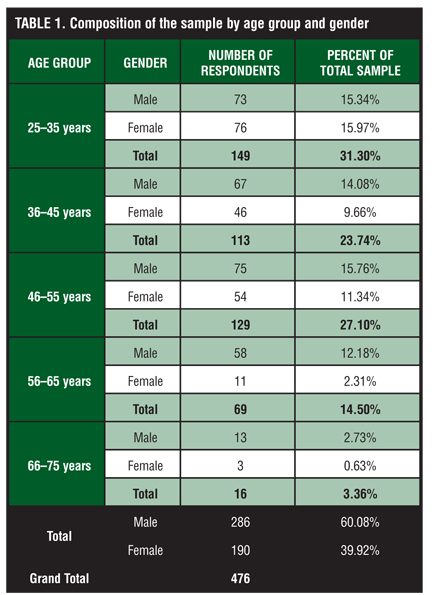
Of 2,845 survey invitations sent, 476 responses were received, resulting in a response rate of 16.73 percent. Of the 476 respondents, 39.8 percent (190) were female and 60.2 percent (286) were male. The sample was relatively evenly spread over the three younger age groups, with fewer respondents representing the two older groups. The demographic characteristics of the sample are outlined in Table 1.
{kind=link}
Of the respondents, 71.7 percent reported that they gave themselves a SSE on a routine basis. Response rates were relatively uniform for all time intervals with 25.4 percent reporting they did a monthly self exam, 24.5 percent every six months, 17.2 percent once per year, and 4.6 percent every five years. Of all respondents, 67.1 percent performed SSE on at least a yearly interval. The likelihood that a respondent would report performing a SSE was not significantly related to age, gender, or history of skin premalignancy/malignancy.
Of respondents who had their skin examined by another dermatologist, 24 percent reported the following frequencies: 1.9 percent had an exam every six months, 10.5 percent went for a yearly exam, and 11.1 percent reported having an exam every five years. This relationship held true when data was analyzed by age (p=0.0490) and gender (p=0.0184). Males were roughly twice as likely as females to visit another doctor for a yearly FBSE (13.29% of males compared to 6.32% of females). There was no age correlation with the use of FBSE.
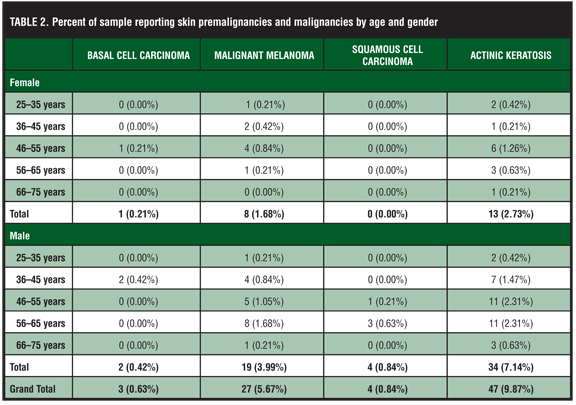
Overall, 17 percent of respondents reported that they had either a history of precancerous or cancerous lesions and this was significantly associated with age (p=0.0002). Study respondents reported the following rates of cancer and precancerous growths: 9.87 percent reported actinic keratoses (AK), 0.63 percent BCC, 0.84 percent SCC, and 5.67 percent MM (Table 2).
{kind=link}
DISCUSSION
In this study, 67.1 percent of participants performed a SSE on at least a yearly basis. In comparison, one Australian community study demonstrated that 48 percent of randomly selected subjects claimed to undergo SSE regularly,[32] while another Australian inquiry showed that only 13 percent of participants performed SSE at least six times throughout a one-year timespan.[33] A US study showed that only six percent of new dermatology patients complied with monthly SSE in an outpatient office setting.[31,34] Dermatologists as a group are more educated on the health issues surrounding skin cancer and, therefore, may be more apt to practice preventative SSE.
Additionally, there are many predictors associated with the increased likelihood of performing a SSE, which include having a partner younger than 59 years of age, believing there is a personal risk for skin cancer development, maintaining a positive attitude toward SSE, and having a previous dermatology visit that resulted in the biopsy or removal of either a suspicious lesion or skin cancer.[35] One of the strongest correlates is the level of confidence an individual has in performing a SSE, which may explain the increased likelihood toward SSE in dermatologists.[35]
Although studies show a greater tendency for women and older individuals to perform SSE,[36–41] no significant difference based on gender or age was observed in this study. The authors had a small proportion of older respondents, which may account for the lack of relationship based on age. Finally, in this study, the rate of SSE was not affected by having a history of precancerous or cancerous lesions. This contrasts with a previous investigation, which demonstrates that a positive history motivates the performance of SSE.[35]
This study is the first to use an e-mail survey to report on the rate of FBSE as completed by dermatologists specifically. In the general population, the frequency of adults in the United States receiving a FBSE has been reported and compared between the years of 1992, 1998, and 2000. A sample of civilian noninstitutionalized participants older than 18 years of age within the United States served as the population for this study, with 12,035 people interviewed in 1992, 32,440 in 1998, and 32,374 in 2000. The participants were interviewed on a host of health-related issues as well as FBSE and were particularly asked if a dermatologist or primary care physician performed the exam. The data was not separated based on the type of physician executing the FBSE. In 1992, 20.6 percent of adults underwent a FBSE, 20.9 percent in 1998, and 14.5 percent in 2000.[39] In another study of 426 patients, 20 percent of patients reported receiving a FBSE from their primary care physician.[40] In this investigation, 24 percent of the dermatologists complied with routine examinations, which is consistent with the current data. When we consider this fact in conjunction with the increased likelihood of a dermatologist to perform SSE, we might conclude that dermatologists are more likely to give themselves an exam than they are to have another doctor perform it.
In 2003, the AAD reported that 30 percent of screened individuals had a presumptive diagnosis of either precancer or cancer. Of the sample, 23 percent of the diagnoses were AK, nine percent were BCC, one percent were SCC, and 0.8 percent were MM. Rates rose steadily with age.[31] In this study, the rate of cancerous or precancerous lesions reported by dermatologists was 17 percent, with diagnosis rates showing a meaningful increase with age. Of the sample, 9.87 percent reported AK, 0.63 percent reported BCC, 0.84 percent reported SCC, and 5.67 percent reported MM. In comparison, this data suggests that dermatologists may have appreciably lower diagnosis rates of precancerous lesions or nonmelanoma skin cancer (NMSC) when compared to the AAD data on screened individuals. The demographic characteristics of the AAD population were as follows: 95 percent were Caucasian/non-Hispanic, 61 percent were women, the highest educational level completed by 41 percent was high school, and the largest group of respondents ranged from 51 to 65 years of age (28%).
The majority of the respondents in the study ranged in age from 25 to 35 years, which may account for the lower frequencies of precancer and NMSC. An increased level of ease using computer and internet technologies may explain the higher number of younger participants.
Dermatologists may possess compounding risk factors for MM, which is one explanation for the frequency seen in our study. These factors could include the high rate of Caucasian physicians in this group, their increased socioeconomic status, their higher educational status, and vacation habits.[15–31] In addition, dermatologists with a history of MM may be more likely to respond, therefore skewing the data.
The limitations of this study include the following: 1) the data could have been affected by telescoping, which is the under-reporting of time between screening exams (telescoping has been described in validation studies on screening[41]; although telescoping has not been specifically associated or applied to skin cancer screenings, it may have potentially played a role in this study); 2) the knowledge of skin cancer prevention harbored by all dermatologists could have biased the data; and 3) there was a low response rate.
To date, the literature has given little attention to studying the means by which dermatologists screen themselves for skin cancer. The authors found that dermatologists perform SSE more frequently than receiving FBSE by another dermatologist. Therefore, SSE appears to be the primary screening tool used by dermatologists for the personal detection of skin cancer.
References
1. American Cancer Society. Cancer Facts and Figures 2005. Atlanta: American Cancer Society; 2005.
2. Jemal A, Murray T, Samuels A, et al. Cancer statistics, 2003. CA Cancer J Clin. 2003;53:5–26.
3. Datamonitor. Drugs of Tomorrow: Cancer Overview. http://www.datamonitor.com/industries/news/article/?pid=0D032CE4-78E7-4DB5-A18B-21FD24830F29&type=Research Wire. Accessed on: October 5, 2008.
4. Marghoob A, Slade J, Salopek T, et al. Basal cell and squamous cell carcinomas are important risk factors for cutaneous malignant melanoma. Cancer. 1995;75(Supp):707–714.
5. Green A. Sun exposure and the risk of melanoma. Aust J Dermatol. 1984;25:99–102.
6. Green A, O’Rourke MGE. Cutaneous malignant melanoma and indicators of total accumulated exposure to the sun: an analysis separating histogenetic types. J Natl Cancer Inst. 1984;74:977–980.
7. Dubin N, Moseson M, Pasternack BS. Epidemiology of malignant melanoma: pigmentary traits, ultraviolet radiation, and the identification of high-risk populations. In: Gallagher RP, ed. Epdiemiology of Malignant Melanoma. Berlin: Springer-Verlag; 1986:56–75.
8. Lindelof B, Sigurgeirsson B, Wallberg P, Ekmund G. Occurrence of other malignancies in 1973 patients with basal cell carcinoma. J Am Acad Dermatol. 1991;25:245–248.
9. Kopf A, Salopek T, Slade J, Marghoob A, Bart R. Techniques of cutaneous examination for the detection of skin cancer. Cancer. 1995;75:684–690.
10. Koh HK. Cutaneous melanoma. N Engl J Med. 1991;325: 171–182.
11. Friedman RJ, Rigel DS, Silverman MK, Kopf A, Vossaert K. Malignant melanoma in the 1990’s: the continued importance of early detection and the role of the physician examination and self-examination of the skin. CA Cancer J Clin. 1991;41: 201–226.
12. Elwood JM. Recent developments in melanoma epidemiology, 1993. Melanoma Res. 1993;3:149–156.
13. Moore D, Martin K, Schneider J. Aggressive awareness campaign can reduce melanoma mortality. Melanoma Res. 1993;3(Suppl):55.
14. Reynolds P, Austin DF. Epidemiologic-based screening strategies for malignant melanoma of the skin. Prog Clin Biol Res. 1984;156:245–254.
15. Ries LAG, Harkins D, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975- 2003. Bethesda, MD: National Cancer Institute. http://seer.cancer.gov/csr/1975_2003/. Based on November 2005 SEER data submission, posted to the SEER website, 2006.
16. Pion I, Rigel D, Garfinkel L, Silverman M, Kopt AW. Occupation and the risk of malignant melanoma. Cancer. 1995;707–714.
17. Viola MV, Houghton A. Melanoma in Connecticut. Conn Med. 1978;42:268–269.
18. Williams RR, Horn JW. Association of cancer sites with tobacco and alcohol consumption and socioeconomic status of patients: interview study from the Third National Cancer Survey. J Natl Cancer Inst. 1977;59:1147–1185.
19. Graham S, Marshall J, Haughey B. An inquiry into the epidemiology of melanoma. Am J Epidemiol. 1985;122: 606–619.
20. Gallagher RP, Elwood JM, Threlfall WJ, et al. Socioeconomic status, sunlight exposure and risk of malignant melanoma: the Western Canada Melanoma Study. J Natl Cancer Inst. 1990;46:1–4.
21. Kirkpatrick CS, Lee JAH, Emily W. Melanoma risk by age and socioeconomic status. Int J Cancer. 1990;46:1–4.
22. Lee PY, Silverman MK, Rigel DS, et al. Level of education and the risk of malignant melanoma. J Am Acad Dermatol. 1992;26:59–63.
23. Krain LS. Malignant melanoma of the skin in California, 1942–1969: epidemiologic and survival considerations. Cutis. 1973;11:350–357.
24. Eklund G, Malec E. Sunlight and the incidence of cutaneous malignant melanoma: effect of latitude and domicile in Sweden. Scand J Plast Reconstr Surg. 1978;12:231–241.
25. Lee JAH, Strickland D. Malignant melanoma, social status and outdoor work. Br J Cancer. 1980;41:757–763.
26. Cooke KR, Skegg DCG, Fraser J. Socioeconomic status, indoor and outdoor work, and malignant melanoma. Int J Cancer. 1984;34:57–62.
27. Online Survey. http://swz.salary.com/salarywizard/layouthtmls/ swzl_co-mpresult_natio nal_HC07000221.html. Accessed September 2009.
28. Elwood JM, Gallagher RP, Hill GB, Pearson JCG. Cutaneous melanoma in relation to intermittent and constant sun exposure—the Western Canada Melanoma Study. Int J Cancer. 1985;35:427–433.
29. Vagero D, Ringback G, Kiviranta H. Melanoma and other tumours of the skin among office, other indoor and outdoor workers in Sweden 1961–1979. Br J Cancer. 1986;53: 507–512.
30. Lew RA, Sober AJ, Cook N, Marvell R, Fitzpatrick TB. Sun exposure habits in patients with cutaneous melanoma: a case control study. J Dermatol Surg Oncol. 1983;9:981–986.
31. Geller A, Zhang Z, Sober A, et al. The first 15 years of the American Academy of Dermatology skin cancer screening programs: 1985–1999. J Am Acad Dermatolol. 2003;48: 34–41.
32. Girgis A, Campbell E, Redman S, et al. Screening for melanoma: a community survey of prevalence and predictors. Med J Aust. 1991;154:338–343.
33. Hill D, White V, Borland R. Cancer-related beliefs and behaviors in Australia. Aust J Public Health. 1991;15:14–23.
34. Lee G, Massa M, Welykyj S, et al. Yield from total skin examination and effetiveness of skin cancer awareness program: findings in 874 new dermatology patients. Cancer. 1991;67:202–205.
35. Robinson J, Fisher S, Turrisi, et al. Predictors of skin self-examination. Cancer. 2002;95:135–146.
36. Robinson J, Rigel D, Amonette R. What promotes self skin-examination? J Am Acad Dermatol. 1998;38:752–757.
37. Weinstock M, Martin R, Riscia P, et al. Thorough skin examination for the early detection of melanoma. Am J Prev Med. 1999;17:169–175.
38. Robinson J, Fisher S, Turrisi R, et al. Predictors of skin self-examination. Cancer. 2002;95:135–146.
39. Saraiya M, Hall I, Thompson T, et al. Skin cancer screening among U.S. adults from 1992, 1998, 2000 national health interview surveys. Am J Prev Med. 2004;39:308– 314.
40. Rodriquez G, Fangchao M, Federman D, et al. Predictors of skin cancer screening practice and attitudes in primary care. J Am Acad Dermatol. 2007;57(5):775–781.
41. Newell S, Girigis A, Sanson-Fisher R, et al. The accuracy of self-reported health behaviors and risk factors relating to cancer and cardiovascular disease in the general population: a critical review. Am J Prev Med. 1999;17:211–229.