Jo-Ann Latkowski, MD, New York University School of Medicine, New York, New York; Peter Heald, MD, Yale University School of Medicine, New Haven, Connecticut
Abstract
In this article, the management of cutaneous T-cell lymphoma will be presented in terms of the strategies that guide treatment. With the strategies and goals in mind, treatment options to achieve a measurable goal will be presented. The treatments presented in this article are those utilized to reliably achieve a remission. If remission is not achieved, a patient’s management plan must be changed. The landmarks that help guide the therapy plan will be discussed.
(J Clin Aesthetic Dermatol. 2009;2(6):22–27.)
There are two distinctly different goals when choosing a treatment for a patient with cutaneous T-cell lymphoma (CTCL): remission or palliation. Remission is measured by tumor burden and palliation is measured by quality of life. Parameters of remission and palliation have been validated in clinical trials, and these can be utilized in the management of patients outside of clinical trials.[1] Defining the goal of therapy is a decision the physician must make with the patient. Many variables influence this decision. Age and stage of disease are two important variables. For example, a 90-year-old patient with widespread patch/plaque disease might have a different goal than a 20-year-old patient with the same clinical presentation; the former choosing palliation and the latter choosing remission. Once the goal of therapy is defined, the therapeutic modality can be selected. This article focuses on treatment options for CTCL that are remittive—agents that can achieve remissions in more than 50 percent of patients treated.
Selecting a Goal for the CTCL Patient: Remission
Remission is defined as the absence of disease in a patient with a chronic disease. In the case of CTCL, remission is achieved when the tumor burden is zero. Numerous studies document cures in CTCL. Most long-term therapy trials define cure as eight years disease free while off all therapy. The first step to cure is a complete remission. When remission is the goal, any compromise of quality of life is endured en route to disease clearance. In addition, to achieve a remission, the physician needs to balance the remission rate with potential complications from comorbid conditions.
Bexarotene Gel
Bexarotene gel is typically used in patients with less than 15-percent body surface area (BSA) involvement. The gel is commercially available at 1% so that dose intensity is varied by the frequency of application. Patients initiate therapy with daily application of bexarotene gel, placing a generous coat on the surface of the lesions. After one week, the frequency is increased to twice daily, then thrice daily after the second week. Topical bexarotene can be used up to four times daily, if tolerated.
A patient using bexarotene gel should be cautioned that an irritant dermatitis can occur at the application site. Complete clearance of lesions will usually occur after 12 to 16 weeks of therapy.[2] The patient should discontinue topical bexarotene 2 to 4 weeks before the next office visit, allowing time for the irritation to resolve so that residual disease can be evaluated. As shown in Figures 1a and 1b , localized areas of involvement can be cleared with bexarotene gel, but the assessment must be done at least four weeks after stopping application (and hence the irritant response). If a partial, but significant, objective response is seen, continuing topical bexarotene for another treatment cycle may be beneficial. The irritant response can be managed by decreasing the frequency of application or by the concomitant use of topical corticosteroids. Successful topical bexarotene therapy requires a compliant patient willing to endure the irritating properties of this vitamin-A derivative. As a retinoid, there is no cumulative toxicity with regard to cutaneous carcinogenesis or structural damage. In fact, the retinoids typically have activities that counter the effects of the mutagens.
{kind=link}
Topical bexarotene is an effective treatment for localized CTCL. The endpoints of therapy are irritant dermatitis and complete clearance of lesions. There is no maintenance therapy with bexarotene, and since there is no cumulative toxicity, treatment can be repeated.
Topical bis-chloroethyl-nitrourea
Topical bis-chloroethyl-nitrourea (BCNU), an alkylating agent, was initially used in the treatment of CTCL in the form of an alcohol-based solution, but is now used in an ointment vehicle. The ointment preparation is compounded by a pharmacy at concentrations ranging from 20mg% to 40mg% and is stable indefinitely at room temperature. The patient only applies the ointment to the affected areas daily or twice daily depending on the cutaneous side effects. The time to maximal response is 8 to 16 weeks.
The side effects of BCNU are primarily cutaneous, including contact hypersensitivity, erythema, skin burning, telangiectasia, and hyperpigmentation. The erythema is prominent in the intertrigenous areas and can occur 2 to 4 weeks after starting therapy. The cutaneous side effects, especially the telangiectasia, can persist after discontinuation of BCNU, but rarely results in permanent changes. Systemic toxicity can occur with BCNU. Bone marrow suppression, most commonly leukopenia and thrombocytopenia, has been reported and thus monitoring with complete blood counts every two weeks during therapy is necessary.[3] Delayed hematopoietic toxicity can also occur, so a complete blood count one month after discontinuing therapy is prudent.[4] The incidence of mild bone marrow suppression is less than 10 percent and dose dependent. A limitation of topical BCNU therapy is systemic toxicity. Therefore, it is primarily used for limited (<15%) BSA.
BCNU is an effective topical treatment for localized CTCL. The endpoints of therapy are severe irritant reaction, bone marrow depression, and complete clearance of lesions. There is no maintenance therapy with BCNU, and patients can expect to undergo repeated courses. It is necessary to have reliable and compliant patients for this therapy to succeed.
Topical Mechlorethamine Hydrochloride, Nitrogen Mustard
Similar to BCNU, nitrogen mustard (NM) was initially used as a freshly prepared solution, but now an ointment formulation is favored. NM is compounded by the pharmacist at 10mg% in Aquaphor (Beiersdorf) or white petrolatum and is stable at room temperature for long periods of time. In the past few years, NM has been difficult to obtain in certain geographic areas. NM ointment can be compounded at most medical center or specialty pharmacies.
The patient applies the NM ointment daily to the entire body. The time to response for NM is approximately 16 weeks. By being one of the first regimens of skin-directed therapy for CTCL, there is excellent long-term follow up of NM-treated patients. Ninety percent of patients with limited CTCL treated with topical NM therapy obtained remission; 67 percent were maintained in a disease-free state for a short follow-up period.[5] In a large series, disease-free intervals of more than three years have been achieved in 13 percent of patients. However, following cessation of therapy, some of these individuals relapsed. Thus, the use of more long-term maintenance regimens seems prudent, but there is no consensus on tapering regimen to maintenance therapy.
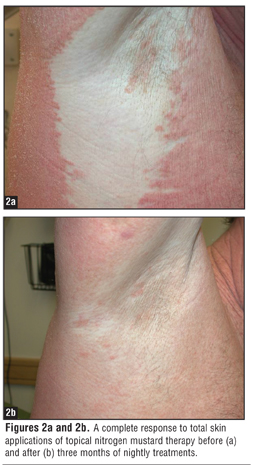
The most common side effect of topical NM is cutaneous hypersensitivity, which occurs readily with the aqueous preparation.[6] The ointment-based NM is less sensitizing than the solution with similar efficacy.[7] Other side effects from NM therapy include a primary irritant reaction, development of second cutaneous malignancies, and hypo- and hyperpigmentation, especially in intertrigenous areas. As shown in Figures 2a and 2b , lesions can often clear with no long-term scarring. Cutaneous malignancies in sun-protected areas of patients treated with NM have also been documented.[8] To minimize the carcinogen effect of NM, discontinue maintenance therapy after six months, educate patients on sun protection and sun avoidance while using NM, and follow patients closely with particular surveillance for skin cancer.
{kind=link}
NM is a safe, effective, self-administered therapy for patients with early stage CTCL but daily total body application is required. The endpoints of therapy are severe contact hypersensitivity reaction and complete clearance of lesions. Maintenance therapy is necessary once remission is induced. Patients should be warned that retreatment may be necessary since relapses are not uncommon. NM maintenance therapy is also utilized to maintain remissions induced by radiotherapy.
Spot Radiation and Total Skin Body
Electron Beam Therapy
Radiation therapy can reliably clear isolated lesions of MF with response rates greater than 90 percent.[9] Superficial and orthovoltage x-rays are given in doses between 20 to 36Gy at individual fractions of 1 to 2Gy per session. However, for the treatment of large surface areas, it is necessary to use electron beam radiation, which is often in the form of total skin body electron beam therapy (TSEBT). TSEBT is an excellent option for CTCL patients who are refractory to other treatment modalities. With a six-field technique, it is possible to administer 1Gy per treatment session as a mean dose over the course of nine weeks, accumulating a total of 36Gy, for example. Those areas not well exposed with the six-field approach need additional therapy, including soles, scalp, perineum, and flexural areas in obese patients. Individual tumors can be spot treated in the midst of TSEBT with 1 to 3Gy fractions for 5 to 10 treatment sessions. Eye and nail shields minimize toxicity in these areas.
Since electrons penetrate only the upper dermis, electron beam therapy may be used without systemic effect. The presumed mechanism of action is the lympholytic effects of ionizing radiation. The total dose of irradiation is important, and a dose of 30Gy or more gives better complete remission rates and disease-free survival than do lower doses. Local cutaneous side effects may include alopecia, atrophy of sweat glands and skin, radiation dermatitis, and edema. When the total dose is highly fractionated, these complications are minimized and sometimes avoided. The question then arises as to the maximum radiation tolerance of the skin. Using the highly fractionated approach, patients can receive a second course of 36Gy electron beam to re-induce a remission. As the total radiation dose increases, so does the risk of squamous cell carcinoma and radiation dermatitis.
TSEBT brings about complete remission in 60 to 95 percent of patients, and the response is stage dependent. The relapse rate is highest in more advanced stages of CTCL (i.e., in those patients with tumors, lymphadenopathy, and visceral involvement). Most relapses occur within the first year after completion of therapy and are relatively rare after three years. The median disease-free interval was greater than three years in the limited plaque group, approximately one year for patients with generalized plaque or erythrodermic disease, and less than six months for patients with cutaneous tumors.[10]
TSEBT can induce a remission in CTCL patients more reliably and quickly than other modalities. The limitations of this therapy are the length of time needed to complete TSEBT (up to three months), the need for a specialized facility for this technically challenging modality, and the finite length of possible treatment. Recent studies, however, have documented that a course of highly fractionated electron beam therapy can be repeated. In one study, 12 patients tolerated a second course and five tolerated a third remission induction.[11] While TSEBT is not amenable to maintenance therapy, both NM and psoralen plus ultraviolet A (PUVA) have been used as maintenance following radiation.
Phototherapy
Phototherapy has been used extensively in CTCL. PUVA photochemotherapy involves UVA activation of orally ingested psoralen in the epidermis and dermis at doses that are cytotoxic to lymphocytes, but not to the structural elements of the skin. The use of the oral photosensitizer incurs several risks for patients, including gastrointestinal intolerance, not reaching therapeutic levels of psoralen (particularly in obese patients), and photosensitivity of the eyes and skin lasting for up to 24 hours after therapy. Presumably, phototherapy works by the toxic effects of UV light on lymphocytes.
PUVA provides complete remissions in patch/plaque CTCL in the majority of patients.[12,13] In thick plaques and tumors, PUVA may be only partially remittive as a monotherapy and is often used with adjuncts. PUVA must be regarded as both a remittive and a maintenance therapy. For inducing a remission, treatments should begin at three times per week with dose escalation at each treatment. It is best to be aggressive with PUVA using maximal doses of both psoralen and UVA. It is important to observe phototoxicity with PUVA to ensure the patient is adequately absorbing psoralen. If poor absorption is suspected, the oral psoralen dose should be increased. After most of the lesions have cleared, the frequency can be decreased to twice weekly until the patient has achieved a complete remission. It is important to maintain the multiple treatments-per-week schedule for a minimum of three and a maximum of six months. By this time, if the patient is not clear, there are several options to boost the therapeutic response, including oral retinoids or interferon (IFN) alpha, both of which can enhance the response to PUVA.
IFN alpha dosed ranging from 3 to 18M units subcutaneously three times weekly can act synergistically with PUVA to clear refractory disease.[14] For those who cannot tolerate IFN, or for those who prefer an alternative, retinoid-PUVA therapy can also be successful. Oral bexarotene at doses of 150 to 450mg/d have been used in conjunction with phototherapy to achieve remission.[15] Once remission is achieved, PUVA alone can usually maintain the remission after the adjunct is discontinued.
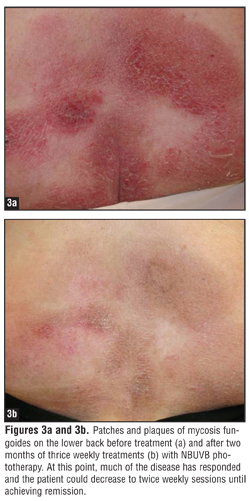
The dependence of PUVA on an oral agent that often causes nausea and necessitates the use of eye protection has led to the use of ultraviolet B (UVB) phototherapy as a technically easier and more acceptable therapy. UVB is administered as either broadband or narrowband, depending on the light source. Narrowband has been shown to be more effective than broadband. Treatment frequency is typically three times per week with dose escalation per treatment until the patient clears. At that point, the patient is slowly weaned off the UVB treatment by gradually decreasing frequency of treatment to maintain remission. UVB phototherapy, whether it be broadband or narrowband, is more convenient and has fewer side effects than PUVA. UVB is less efficacious than PUVA phototherapy. UVB can elicit remissions, but requires more frequent dosing to obtain clearance and to maintain clearance than does PUVA.[16,17] Ideal patients are those with patch disease since UVB penetrates much less deeply than UVA wavelengths. As shown in Figures 3a and 3b , once clearing is well underway with UVB, the frequency can be decreased from three to two sessions per week until clear. Home phototherapy with UVB is another option; however, this requires an extremely well-informed and diligent patient.[18]
{kind=link}
With all of the phototherapies, the most easily exposed lesions clear rapidly. Lesions that may persist deep in the groin, on the ankles, buttock crease, and the eyelids do not represent therapy failure; rather, they represent a sanctuary from the skin-directed therapy. These lesions often require adjunctive therapy, such as topical bexarotene, BCNU, or radiation therapy. If patients do not clear with phototherapy, an adjunct therapy should be considered, such as oral bexarotene or IFN alpha.
The side-effect profile of phototherapy is similar for PUVA and UVB. The most common side effects are photosensitivity and phototoxicity, including photoaging and increased risk of skin cancer. With PUVA, nausea and cataract formation are additional limiting toxicities.
Bone Marrow Transplantation
Another treatment modality for CTCL is the use of allogeneic bone marrow transplantation. There are several reports of long-term complete remissions in CTCL patients with advanced disease who have received ablative doses of chemotherapy followed by restoration of the marrow precursors.[19] The current method is to use a reduced intensity allogeneic stem cell transplant, preferably from a matched sibling.[20] With this strategy, the goal is to initiate graft-versus-host (GVH) disease in the form of graft versus lymphoma to control the CTCL. With reduced intensity preparation, there is often residual disease in the skin at the time of transplantation. In the peri-transplant period, patients are exposed to systemic immunosuppressants to help control the GVH. Immunosuppression can accelerate CTCL so most patients will need adjunctive therapy that does not compromise their fledgling bone marrow. Oral bexarotene, phototherapy, and radiation therapy have all been used to get patients through the peri-transplant period. The role of allogeneic bone marrow transplantation is still being delineated in CTCL. It is currently considered only in patients who are less than 60 years old with a low probability of remission.
Maintaining Remission
Once the patient’s tumor burden is zero, the physician’s main focus is how to maintain remission. For most of the remittive therapies, this entails a slow wean off of the therapeutic. For example, PUVA is initially administered at once-weekly frequencies until one year has passed. At this point, one week can be added between treatments and a total of 25 sessions over one year will be needed. Should the patient still be in remission at this point, the same addition is carried out over two more years so that eventually patients are receiving 12 sessions per year for at least two years. At this point, the patient should have been in remission for five years. Once a patient has achieved complete control with 12 sessions per year, the continued use of maintenance is balanced against evidence of phototoxicity, photocarcinogenesis, and the possibility that a relapse may necessitate a return to multiple-sessions-per-week therapy. Long-term side effects include atrophy and dryness of the skin, cataracts, and skin cancer. The latter is of concern in CTCL patients who may also have been exposed to mutagens of previous x-ray or topical chemotherapy.[21]
Summary
Therapies used to achieve remission in CTCL are defined as successful if the tumor burden measures fail to reflect residual disease. As discussed in this paper, these therapies often compromise quality of life if they interrupt daily activities (phototherapy), require tedious whole body applications (NM), cause alopecia (radiotherapy), induce irritant dermatitis (bexarotene gel), or are associated with a significant risk of mortality (allotransplantation). When these features are combined with refractory disease, the therapy strategy often shifts to a palliative mode.
References
1. Heald P. Clinical trials and efficacy assessment in the therapy of cutaneous T cell lymphoma. Ann NY Acad Sci. 2001;941:155–165.
2. Heald P, Mehlmauer M, Martin AG, et al. Topical bexarotene therapy for patients with refractory or persistent early-stage cutaneous T-cell lymphoma: results of the phase III clinical trial. J Am Acad Dermatol. 2003;49:801–815.
3. Zackheim HS, Epstein EH, Crain WR. Topical carmustine (BCNU) for cutaneous T cell lymphoma: A 15-year experience in 143 patients. J Am Acad Dermatol. 1990;22: 802–810.
4. Zackheim HS, Epstein E, McNutt NA, et al. Topical carmustine for mycosis fungoides and related disorders: A 10 year experience. J Am Acad Dermatol. 1983;9:363–372.
5. Vonderheid EC, Tan ET, Cantor AF, et al. Long-term efficacy, curative potential, and carcinogenicity of topical mechlorethamine chemotherapy and cutaneous T cell lymphoma. J Am Acad Dermatol. 1989;20:416–428.
6. Ramsay DL, Halperin PS, Zeleniuch Jacquotte A. Topical mechlorethamine therapy for early stage mycosis fungoides. J Am Acad Dermatol. 1988;19:684–691.
7. Price NM, Hoppe RT, Deneau G. Ointment-based mechlor-ethamine treatment for mycosis fungoides. Cancer. 1983;52:2214–2219.
8. Lee LA, Fritz KA, Golitz L, et al. Second cutaneous malignancies in patients with mycosis fungoides treated with topical nitrogen mustard. J Am Acad Dermatol. 1982;7:590–598.
9. Wilson LD, Kacinski BM, Jones GW. Local superficial radiotherapy in the management of minimal stage IA cutaneous T-cell lymphoma (mycosis fungoides). Int J Radiat Oncol Biol Phys. 1998;40:109–115.
10. Jones G, Wilson LD, Fox-Goguen L. Total skin electron beam radiotherapy for patients who have mycosis fungoides. Hem Onc Clin NA. 2003;17:1421–1434.
11. Wilson LD, Quiros PA, Kolenik SA, et al. Additional courses of total skin electron beam therapy in the retreatment of patients with cutaneous T-cell lymphoma. J Am Acad Dermatol. 1996;35:69–73.
12. Diederen PV, Van Weelden H, Sanders CJ, Van Vloten WA. Narrowband UVB and psoralen-UVA in the treatment of early stage mycosis fungoides: a retrospective study. J Am Acad Dermatol. 2003;48:215–219.
13. Herrmann JJ, Roenigk HH Jr, Hurria A, et al. Treatment of mycosis fungoides with photochemotherapy (PUVA): long-term follow-up. J Am Acad Dermatol. 1995;33:234–342.
14. Mostow EN, Neckel SL, Oberhelman L, et al. Complete remissions in psoralen and UVA (PUVA)-refractory mycosis fungoides-type cutaneous T-cell lymphoma with combined interferon alfa and PUVA. Arch Dermatol. 1993;129: 47–762.
15. Singh F, Lebwohl MF. Cutaneous T cell lymphoma treatment using bexarotene and PUVA: a case series. J Am Acad Dermatol. 2004;51:570–573.
16. Ramsay DL, Lish KM, Yalowitz CB, Soter NA. Ultraviolet-B phototherapy for early-stage cutaneous T-cell lymphoma. Arch Dermatol. 1992;128:931–933.
17. Hofer A, Cerroni L, Kerl H, Wolf P. Narrowband (311-nm) UVB therapy for small plaque parapsoriasis and early-stage mycosis fungoides. Arch Dermatol. 1999;135:1377–1380.
18. Resnik KS, Vonderheid EC. Home UV phototherapy of early mycosis fungoides: long-term follow-up observations in thirty-one patients. J Am Acad Dermatol. 1993;29:73–77.
19. Molina A, Zain J, Arber DA, et al. Durable clinical, cytogenetic and molecular remissions after allogeneic hematopoietic cell transplantation for refractory Sezary syndrome and mycosis fungoides. J Clin Oncol. 2005; 6163–6171.
20. Herbert KE, Spencer A, Grigg A, et al. Graft-versus-lymphoma effect in refractory cutaneous T cell lymphoma after reduced intensity HLA matched sibling allogeneic stem cell transplantation. Bone Marrow Trans. 2004;34: 521–525.
21. Abel EA, Sendagorta E, Hoppe RT. Cutaneous malignancies and metastatic squamous cell carcinoma following topical therapies for mycosis fungoides. J Am Acad Dermatol. 1986;14:1029–1038.