Resident’s Forum
Section Editor: Jerry Tan, MD, FRCPC: Adjunct Professor, University of Western Ontario, London, Ontario; President, Windsor Clinical Research Inc., Windsor, Ontario; and Consultant, Windsor Regional Hospital, Windsor, Ontario, Canada. He is also in private practice.
Resident Section Editors: Sanjay Bhambri, DO, and Joshua Zeichner, MD
Sanjay Bhambri, DO: Chief Dermatology Resident, Valley Hospital Medical Center, Las Vegas, Nevada; Avani Bhambri, MD: 3rd Year Dermatology Resident, UCLA Department of Dermatology, Los Angeles,California; James Q. Del Rosso, DO Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada, Touro University College of Osteopathic Medicine, Henderson, Nevada; Clinical Associate Professor, Dermatology, University of Nevada School of Medicine, Las Vegas and Henderson, Nevada.
Abstract
Sclerotic fibroma is a rare skin neoplasm that can be seen sporadically or in association with disorders such as Cowden’s disease. We present a case of solitary sclerotic fibroma that presented as an asymptomatic nodule in a 40-year-old man with no evidence of Cowden’s disease. Histopathologically, the lesion was consistent with a sclerotic fibroma displaying hypocellular collagen bundles with clefts.
Introduction
Sclerotic fibroma is an uncommon skin tumor associated with Cowden’s disease (multiple hamartoma syndrome). Solitary sclerotic fibroma can be seen in patients without a personal or family history of Cowden’s disease. It is characterized histologically by a well-circumscribed, nonencapsulated, dermal nodule comprising hypocellular sclerotic collagen bundles with prominent clefts. The authors present a case of solitary sclerotic fibroma in a patient with no evidence of Cowden’s disease.
Case Report
A 40-year-old man presented to the authors’ office for an evaluation of a lesion located on the right temporal scalp. During the physical examination, he was noted as having a 1.5cm, soft, flesh-colored, waxy plaque (Figure 1) on the right temporal scalp. The patient stated the lesion had been present for 20 years, but has increased in size over the past three years. The patient denied any symptoms from the lesion. A 6mm punch biopsy was performed through the lesion.
{kind=link}
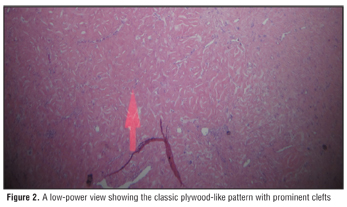
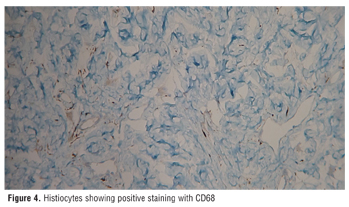
Histopathology revealed fusiform cellular proliferation and collagenous change in papillary and reticular connective tissue (Figure 2 and Figure 3) with some histiocytes that stained positive with CD68 (Figure 4).
{kind=link}
{kind=link}
{kind=link}
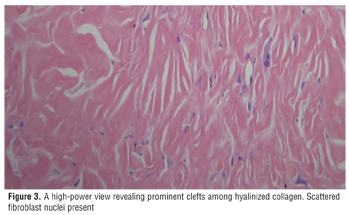
Prominent clefts were noted among hyalinized eosinophilic collagen bundles arranged in a plywood-like pattern (Figure 3). There was no architectural or cytological atypia and the epidermis was without any pathologic alteration. The lesion was S-100 negative. The histopathological pattern was consistent with that of a benign storiform collagenoma.
Given the benign nature of the lesion, the patient was reassured that treatment was not necessary. However, the lesion was subsequently excised per the patient’s request.
Discussion
Sclerotic fibroma or storiform collagenoma is an uncommon cutaneous neoplasm that was first reported in 1972 by Weary et al in a biopsy of a lesion from the tongue of a patient with Cowden’s disease.[1] Sclerotic fibromas may occur as a solitary sporadic tumor or in multiple numbers as part of the cutaneous manifestation of Cowden’s disease, a genodermatoses that is acquired in an autosomal dominant manner. It is unclear whether sclerotic fibroma represents a hamartoma or a true fibrocystic neoplasm.[2,3]
Rapini and Golitz coined the term “sclerotic fibroma” when they reported 11 cases of solitary lesions in patients without any evidence of Cowden’s disease.[5] The average patient age was 40 years with a range from 7 to 62. There was no preferential location; however, 5 of 11 lesions were located in the head and neck region. The lesion was more common in females (8 of 11). The average lesion size was 5.5mm with a range of 2 to 9mm. Similar reports of solitary sclerotic fibroma not associated with Cowden’s disease have also been described and reported by other authors.[6]
Clinically, the lesion usually presents as asymptomatic, flesh-colored, white, translucent, waxy papules and can occur on any location. Solitary sclerotic fibroma is a benign lesion and no treatment is usually required. The lesion can, however, be removed through a simple excision as was done in our patient.
Histopathology
Histopathologically, a well-circumscribed, nonencapsulated, and sharply demarcated dermal nodule comprising hyalinized thick bands of collagen is noted. The nodule is usually hypocellular or acellular. The thick collagen bundles were arranged in a whorled or plywood-like pattern with prominent clefts between collagen bundles.
Immunohistochemistry
Sclerotic fibroma usually stains positive for vimentin and CD34, but negative for neurofilaments, S-100, neuron-specific enolase (NSE), carcinogenic embryonic antigen (CEA), embryonic membrane antigen (EMA), high molecular weight keratin, and cytokeratin.[3,6,10,11] A factor 13a stain shows positivity for scattered dendritic cells. This can be useful in differentiating sclerotic fibroma from a dermatofibroma, which shows diffuse positivity in the entire lesion. Bodian stain is usually negative.[9] It has been suggested that the lesion is an actively growing fibroblastic neoplasm with abnormal regulation of type I collagen production and processing.[4] Fibronectin deposition within clefts, detected by immunofluorescence, has been reported.[7] Proliferation of spindle cells with myoid features resulting in collagen production was recently seen under ultrastructural examination.[8]
Conclusion
In summary, the authors present a case of solitary sclerotic fibroma in a patient with no evidence of Cowden’s disease. Sclerotic fibroma, when present in multiple numbers, serves as a clue for the presence of multiple hamartoma syndrome. When present as solitary, a sclerotic fibroma lesion is benign and treatment is usually not warranted.
References
1. Weary PE, Gorlin RJ, Gentry WC, et al. Multiple hamartoma syndrome (Cowden’s disease). Arch Dermatol. 1972;106:682.
2. Donati P, Amantea A, Carducci M, et al. Sclerotic (hypocellular) fibromas of the skin. Br J Dermatol. 1991;124(4):395–396.
3. Lo WL, Wong CK. Solitary sclerotic fibroma. J Cutan Pathol. 1990;17(5):269–273.
4. Shitabata PK, Crouch EC, Fitzgibbon JF, et al. Cutaneous sclerotic fibroma. Immuno-histochemical evidence of a fibroblastic neoplasm with ongoing type I collagen synthesis. Am J Dermatopathol. 1995;17(4):339–343.
5. Rapini RP, Golitz LE. Sclerotic fibromas of the skin. J Am Acad Dermatol. 1989;20(2 Pt 1):266–271.
6. Metcalf JS, Maize JC, LeBoit PE. Circumscribed storiform collagenoma (sclerosing fibroma). Am J Dermatopathol. 1991;13(2):122–129.
7. Nogita T, Akiyoshi E, Kawashima M, et al. Deposits of fibronectin in sclerotic fibromas of the skin. J Dermatol. 1993;20(2):125–126.
8. Nakashima K, Yamada N, Adachi K, et al. Solitary sclerotic fibroma of the skin: morphological characterization of the ‘plywood-like pattern’. J Cutan Pathol. 2008;35(Suppl 1):74–79.
9. Furue M, Harada S. Sclerotic fibroma of the skin arising on the nasal ala. J Dermatol. 1993;20(4): 252–253.
10. Hanft VN, Shea CR, McNutt NS, et al. Expression of CD34 in sclerotic (“plywood”) fibromas. Am J Dermatopathol. 2000;22(1):17–21.
11. Cohen PR, Tschen JA, Abaya-Blas R, et al. Recurrent sclerotic fibroma of the skin. Am J Dermatopathol. 1999;21(6):571–574.