A discussion of data from clinical studies with a gel formulation of clindamycin
phosphate 1.2% and tretinoin 0.025%
by James Q. Del Rosso, DO, FAOCD
Tretinoin, a commonly prescribed topical retinoid for the treatment of acne that has been used for more than 30 years, is recognized as an effective treatment that normalizes follicular desquamation of the epithelium.[1] The original hydroalcoholic formulation of tretinoin (0.05%) was frequently associated with significant cutaneous irritation, with up to 20 percent of patients developing new papules and pustules during the first few weeks of treatment.[2] This “acne flaring” was considered a potential problem that limited the use of tretinoin.1 Since the initial development of tretinoin, newer vehicle formulations have emerged, which are associated with less cutaneous irritation, and other topical retinoids have evolved, such as tazarotene and adapalene.[3,4] These latter compounds have been shown to effectively treat acne vulgaris, and similar to tretinoin, reduce the number of both inflammatory and non-inflammatory acne lesions.[1,5]
Although most dermatologists appreciate that topical retinoids exhibit anti-inflammatory activity, many still have concerns about using a topical retinoid in the early stages of treating a patient with inflammatory acne due to fear of an acne flare.[2] Unfortunately, prior to the development of a combination aqueous gel containing clindamycin phosphate 1.2% and tretinoin 0.025%, the issue regarding initial acne flaring after starting topical retinoid therapy has not been prospectively evaluated.
What are the characteristics of clindamycin phosphate 1.2%/tretinoin 0.025% gel?
A gel containing clindamycin phosphate 1.2% in combination with tretinoin 0.025% was approved by the Food and Drug Administration (FDA) in November, 2006. Within the gel vehicle, clindamycin phosphate exists in solution. However, tretinoin exists partially in solution, with the remainder present in crystalline form in suspension. The crystalline particle size is controlled to allow for optimal follicular penetration. Tretinoin release from the crystalline state is not immediate, and tretinoin delivery is slower than from a solution; thus, resulting in a lower potential for skin irritation.[6]
What clinical trials have been conducted on the combination gel formulation of clindamycin phosphate 1.2% and tretinoin 0.025%?
Three multicenter, double-blind, randomized trials assessed the effects of three topical treatments compared to a vehicle gel on incidence rates of acne flares. The clinical trials for this combination therapy evaluated patients after two weeks of treatment to determine whether a flare in inflammatory lesions occurred in those treated with tretinoin 0.025% alone versus those treated with the clindamycin/tretinoin combination or with clindamycin alone.
What were the study designs and methods?
Three multicenter, double-blind, randomized, Phase 3 trials compared the effect of topical treatments on incidence rates of acne flares following the initial two weeks of treatment.[6] In two of the trials, subjects were randomly assigned to one of four study groups, including (1) clindamycin phosphate 1.2% gel plus tretinoin 0.025% gel (CLIN/RA), (2) tretinoin 0.025% gel (RA), (3) clindamycin phosphate 1.2% gel (CLIN), or (4) gel vehicle alone (VEH).[6] The third trial randomized subjects to either CLIN/RA or CLIN.[6]
Eligibility criteria for the three studies were (1) 20 to 100 noninflammatory lesions, (2) 20 to 50 inflammatory lesions, and (3) two or fewer nodules.[6] Conventional mandatory washout periods were required for all topical and systemic treatments. Acne severity was established for each subject at baseline as mild, moderate, or severe based on investigators’ ratings on the Evaluator’s Global Severity Scale (EGSS). The investigators were blinded to patients’ baseline EGSS scores.[6] Two measures of flaring (>10% and >20% increase in inflammatory lesions) were obtained at two weeks post-treatment to determine the degree of flaring in response to the different regimens.
What were the study results?
A total of 4,550 subjects were randomly assigned to treatment groups in the three trials.[6] Patients in the three studies ranged in age from 11 to 59 years (mean, 18.98 years) with no significant differences between patients with respect to age, gender, or race. Of the 4,550 subjects, 74% (n=3,355) were considered to have moderate acne at baseline. No significant differences between the three studies existed with respect to the distribution of EGSS scores, and there were comparable numbers of inflammatory lesions, noninflammatory lesions, and total acne lesions in all treatment groups in the three studies at baseline. Within each treatment group, there were a mean of 29 inflammatory lesions per patient (range, 4–63), 49 noninflammatory lesions (range, 9–141), and 78 total acne lesions (range, 21–195).[6]
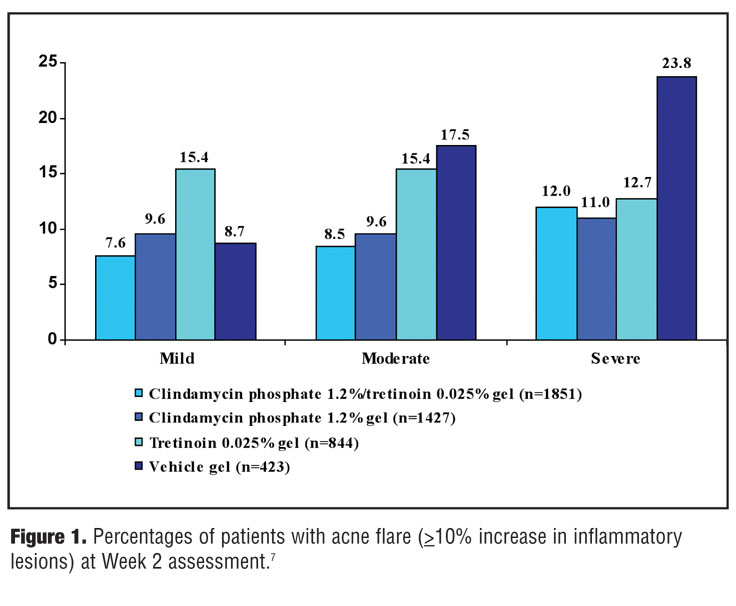
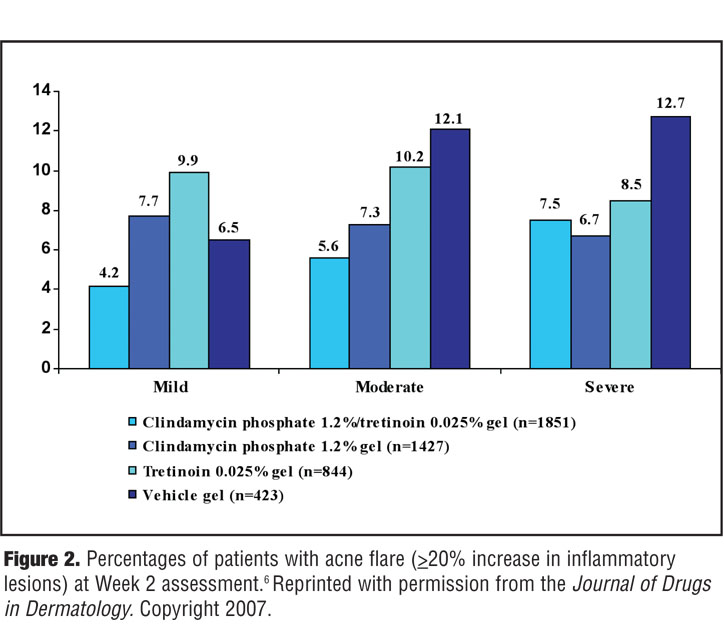
The percentages of patients who experienced an increase of at least 10 percent or 20 percent in the number of inflammatory lesions after the first two weeks of treatment are shown in Figure 1 and Figure 2.[7] Analysis of flare responses in patients using the 10 percent or greater measure stratified by severity of acne based on EGSS scores revealed that the majority of patients experienced an improvement in acne lesions.
{kind=link}
{kind=link}
Among patients with mild acne at baseline, the highest flare rate was observed for patients who received tretinoin monotherapy (15.4%). In patients with moderate or severe acne at baseline, the highest prevalence of flares was noted in the VEH group (23.8%) for patients with severe acne at baseline. At the 10 percent or greater measure, patients treated with CLIN/RA consistently had the lowest rates of flaring (7.6% of patients with mild acne and 8.5% of patients with moderate acne at baseline), except in those study subjects who had severe acne at baseline. There was little difference between flare rates for those patients in the clindamycin monotherapy group (11%) and those in the CLIN/RA group (12%).
Results were similar when the 20 percent measure was used to determine flare rates after two weeks of therapy. Among those with moderate acne at baseline, the CLIN/RA group had significantly lower percentages of patients with 10 percent or greater and 20 percent or greater increases in inflammatory lesions than did the tretinoin monotherapy and VEH groups (P<0.001 for all comparisons).
What produces acne flaring, the vehicle or the active compound?
Acne flaring, as demonstrated by a visibly noticeable increase in inflammatory lesions, can be observed in patients treated with an active compound when compared to those treated with a vehicle formulation. If higher proportions of patients treated with a topical retinoid are shown to have an increase in inflammatory lesions than those treated with antibiotic monotherapy, this suggests exacerbation of inflammation by the active topical retinoid. Alternatively, it is possible that the increase in inflammatory lesions could be the result of the natural drive of underlying acne overcoming the anti-inflammatory activity of the therapy and/or it may represent a delay in the onset of therapeutic activity.
What were the conclusions regarding acne flaring based on the clinical trials completed with clindamycin phosphate 1.2%/tretinoin 0.025% gel?
Results from the three Phase 3 clinical trials demonstrate that treatment with a 0.025% formulation of tretinoin used as monotherapy provoked acne flaring in a subset of subjects.[6] Almost twice as many study participants with mild acne at baseline demonstrated a 10 percent or greater increase in number of inflammatory lesions as compared to subjects in the vehicle arm (15.4% vs 8.7%). However, this effect was seen only for those with mild acne at baseline and not in those with moderate or severe baseline inflammatory acne. There was no evidence that clindamycin phosphate 1.2%/tretinoin 0.025% gel provoked acne flaring.
References
1. Leyden JJ. A review of the use of combination therapies for the treatment of acne vulgaris. J Am Acad Dermatol 2003;49(suppl 3):S200–S210.
2. Kligman AM, Fulton JE, Jr, Plewig G. Topical vitamin A acid in acne vulgaris. Arch Dermatol 1969;99(4):469–476.
3. Differin® (adapalene cream, 0.1%) [package insert]. Fort Worth, Tex; Galderma Laboratories, LP; June 2004. Available at: http://www.differin.com/AboutDifferin/ProductInsert_Cream.aspx. Accessed November 15, 2007.
4. Tazorac® (tazarotene cream 0.05% and 0.1%) [package insert]. Irvine, Calif: Allergan, Inc; May 2004. Available at: http://www.allergan.com/ download/TAZORACcream.pdf. Accessed November 15, 2007.
5. Smolinski KN, Yan AC. Acne update: 2004. Curr Opin Pediatr 2004;16(4):385–391.
6. Schlessinger J, Menter A, Gold M, et al. Clinical safety and efficacy studies of a novel formulation combining 1.2% clindamycin phosphate and 0.025% tretinoin for the treatment of acne vulgaris. J Drugs Dermatol. 2007;6(6):607-615.
7. Eichenfield LF, Gendreau MA. Topical acne treatments express report-new topic retinoid/antibiotic treatment option for acne vulgaris: focus on safety and tolerability. Dermatology Education Initiative. Hampton, NH: Millennium CME Institute, Inc.; 2007:1–4.