Yvette A. Tivoli, DO, Palmetto General Hospital, Hialeah, Florida; bRichard M. Rubenstein, MD, Co-Director, Wellington Regional Medical Center Dermatology Program, Wellington, Florida
Abstract
Pruritus is among the most common dermatological complaints. The authors examine the pathophysiology of itch according to the most common mediators uncovered by researchers. They also discuss the encompassing etiologies, which include dermatological, psychological, and systemic causes. Finally, they discuss the diagnostic approach and the latest, most appropriate treatment options. (J Clin Aesthetic Dermatol. 2009;2(7):30–36.)Pruritus, or itching, is a frequent complaint heard by dermatologists and primary care physicians. Although generally considered a benign symptom, pruritus can have adverse effects on a patient’s wellbeing and can be incapacitating when severe. The mechanisms of pruritus are not particularly well understood and are compounded by the subjective nature of the process itself. Pruritus occurs with a host of dermatological conditions, but can also be a marker of systemic disease. Dermatologists and primary care physicians must be aware of the varied causes of itching.
Everyone knows the sensation of itching, yet it is an elusive concept to define. The term “itch” is commonly used in the English language—we itch to get our hands on something, we scratch our heads to solve a problem, and who among us does not have the itch to succeed? Itching has been defined by Tonneson[1] as “an irritating sensation which evokes the impulse to scratch.” The aggravating and nonadapting nature that invokes scratching distinguishes itching from other cutaneous sensations, such as pain, touch, and temperature.
Physiologically, itching is the conscious expression of cutaneous sensations that evoke the well-known scratch reflex. The purpose of this reflex is the removal of the noxious stimulus. Unfortunately, scratching can cause further damage to the skin and can perpetuate the problem. Severe pruritus can be relieved by self-trauma, essentially replacing itching with pain, but such action can result in chronic skin changes, such as lichenification, erythema, excoriation, and even lacerations.
Pathophysiology
Itch has been categorized into the following four classifications: cutaneous, neuropathic, neurogenic, and psychogenic.[2] Cutaneous itch, also referred to as pruritoceptive itch, is due to inflammation of the skin. Neuropathic itch is caused by an itch that arises anywhere along the afferent nerve pathway due to damage of the nervous system. It is typically seen in herpetic neuralgia, multiple sclerosis, and brain tumors. Neurogenic itch originates centrally without evidence of neuronal pathology, as seen in cholestasis. Lastly, psychogenic itch is seen in delusional states, such as parasitophobia.
Pruritogens are substances that stimulate itch-mediated C fibers. These unmyelinated fibers are slow conduction velocity fibers (mean 0.5m/s) with extensive terminal branches. These fibers transmit to the dorsal horn of the spinal cord and via the lateral spinothalamic tract to the thalamus, and finally the somatosensory cortex. The brain then interprets this as the sensation of itching.
Mediators
Studies on itching have resulted in a better under-standing of the pathophysiology of this process. It is a complex process that involves a multitude of pruritogenic substances and receptors. The most notable itch-mediating substance is histamine. It is stored in mast cells and keratinocytes.[3]
Histamine. In the 1920s, Sir Thomas Lewis demonstrated that intradermal injection of histamine elicited itch and a vascular response with erythema, wheal, and flare. These are the symptoms exhibited in urticaria.[4,5] Antihistamines usually treat the symptoms of urticaria, but some cases respond poorly, indicating there are other mediators, such as cytokines and chemokines.[2] Though efficacious, the actual role of antihistamines in reducing itch may be due more to the sedative effect. It seems nonsedating antihistamines do not have any effect on itching dermatoses absent of erythema and wheal formation.[6]
Histamine can also be released via immunoglobulin E receptors, complement, C5a, and tachykinins, including the neuropeptide substance P (SP).[4] Histamine displays tachyphylaxis upon repeated injection of histamine, and thus it generally will not mediate chronic persistent itch.
Serotonin (5-HT). Serotonin (5-HT) is another amine compound stored in human platelets. It is released when platelets aggregate. This substance may regulate itch by acting on 5-HT3 receptors. A placebo-controlled study of a 5-HT3 antagonist, ondansetron, demonstrated significant reduction in itch 30 to 60 minutes after the drug was administered and lasted up to six hours.[4]
Acetylcholine. Acetylcholine, a neurotransmitter, stimulates histamine-sensitive and insensitive C-fibers. The flare response with intradermal injection of acetylcholine is smaller than that of histamine injection. Studies have demonstrated that patients with atopic dermatitis have increased sensitivity to acetylcholine versus normal subjects. Normal patients experienced pain upon administration of acetylcholine injection, but the atopic subjects experienced itching.[2,7,8]
Prostaglandins. Prostaglandins, arachidonic acid metabolites, are not themselves pruritogenic, but rather they potentiate itching caused by histamine and other mediators. Studies have shown that when abraded skin was pretreated with prostaglandin E, the itch threshold was lowered.[2,4] There has been some evidence that leukotrienes may have some relevance with respect to itching. An article by Miyoshi et al[9] found a correlation between elevated urinary leukotriene B4 levels in patients with atopic dermatitis with associated nocturnal itch.
Other mediators. Other mediators of the itch response have been appreciated historically. Mucuna pruriens, a tropical plant with pods that are covered by cowhage spicules, is known to cause ferocious itching. Although this plant was first described by an English physician who accompanied the Duke of Albermarle on a trip to Jamaica in 1688, the natives knew about it for some time. The natives would eat this inhospitable bean in times of scarcity only. They would heat the spicules to prevent the itching, for it was felt for some time that the spicules themselves caused the itching. In fact, the term cowhage is from the Hindu kiwach, or bad rubbing. In the late 18th century, William Chamberlain sprinkled cowhage on intestinal roundworms and noted their hyperactivity (which may have been caused by itching), causing them to release their hold on the intestinal mucosa. He noted that prior boiling of the spicules eliminated this effect and the worms stayed happily attached to the intestine.[10]
It was not until 1955 that Shelley and Arthur isolated a heat labile endopeptidase from the mucuna plant, mucunain, which produces itching upon subepidermal injection.[11] The Jamaicans were unknowingly altering a heat-labile substance when they boiled the spicules of the mucuna plant.
Subsequently, many other peptidases have been shown to be produced by epidermal or dermal cells from inflammation and give rise to itching. A number of peptides are also known to cause a vascular response and varying degrees of itch, including kinins, vasoactive intestinal protein, enkephalin, and substance P. The effects of these substances may be mediated through the subsequent release of histamine, since exhaustion of skin histamine by agent 48/80 (a histamine releaser) or H1 blockers can prevent these responses.
Mechanical factors may play a role in pruritis, including heat (vasodilation) and xerosis. Nighttime pruritus, which is often organic in nature, is associated with increased parasympathetic activity and a lowered threshold to itching.
Substance P (SP), the oldest and most studied neuropeptide, is an 11-amino-acid substance that, when injected intradermally, causes flare, wheal, and itch. However, it causes itch indirectly by release of histamine from dermal mast cells.[4,5] This was concluded based on the use of 48/80, a histamine liberator compound that reduced the amount of histamine stores and ultimately itch. With repeated topical application, capsaicin depletes C-fiber contents of neuropeptides and destroys approximately 80 percent of these fibers. This mechanism reduces itch symptoms in chronic itch disorders.[2,4]
Interleukins (ILs)—cytokines produced by lymphocytes—as well as keratinocytes, fibroblasts, and mast cells in the skin, play a role in the pathophysiology of itch. Intradermal injections of IL-2 in atopic and nonatopic patients revealed itching several hours after administration. The itch and erythema lasted for 2 to 3 days.[2,12] It has also been noted that intravenous IL-2, when given with chemotherapy, has caused intense itching.[2]
Opioid receptors have been found to play a role in central and peripheral induction of itch; mu opiate receptors (MOR) modulate pain and itch in the central nervous system.4 Itch may be provoked by an imbalance between these receptors. The opiate kappa receptor TRK-820 was effective in the treatment of uremic pruritus.[13] Investigation of opiate receptors has suggested that itch may be provoked by an imbalance between the mu and kappa opioid systems in systemic and peripheral pathways.[9]
A recent intriguing study by Davidson et al14 found that noxious stimuli (scratching) stopped the firing of spinal cells in an animal model. This suggests that itch may be modified by spinal cord activity.
Etiology
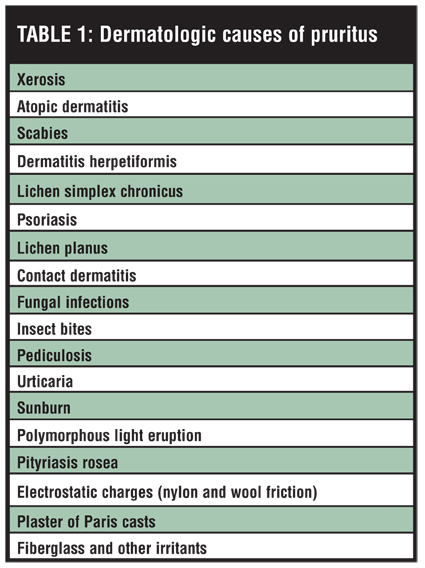
Dermatological. When approaching the itching patient, one should first consider a variety of skin diseases that are known to cause pruritus (Table 1). Xerosis, or dry skin, by itself is a cause of significant pruritus. A particularly common problem in the elderly, xerosis may be exacerbated by environmental factors, such as cold air, low humidity, or central heating. Atopic dermatitis, or eczema, is a chronic skin disorder usually presenting in infancy or childhood. Involved areas, such as the flexor surfaces, will be quite pruritic, and papules may appear with varying degrees of lichenification depending upon the amount of scratching. A personal or family history of atopy (eczema, asthma, or hay fever) is helpful in identifying this condition.
{kind=link}
A common, easily missed, and treatable condition is scabies, a fiercely pruritic disorder caused by the mite Sarcoptes scabiei. Patients with these parasites can have itching over their entire body without primary skin lesions, but will usually have widespread excoriations. A history of scabies and other family members with similar problems is suggestive of this condition. Infants may be affected as well. The diagnosis is made by identifying the mite from skin scrapings or biopsy. Treatment involves overnight application of permethrin cream or other antiscabetic preparations.
Dermatitis herpetiformis is an uncommon, but intensely pruritic, papulovesicular eruption occurring on extensor surfaces in young adults. The diagnosis is made on clinical, and histological findings, as well as immunoglobulin A (IgA) depositions in the dermal papilla.
Lichen simplex chronicus, or neurodermatitis, refers to localized, lichenified patches of pruritic skin caused by frequent scratching. The stimulus for itching is unknown, but these areas may respond to local application of corticosteroids.
A host of other dermatological conditions may cause pruritus. A careful history and physical examination can aid in the diagnosis of many of these disorders. Some have characteristic clinical findings, such as the silver erythematous scales of psoriasis, the linear vesicular eruptions of contact dermatitis, and the flat-topped violaceous papules of lichen planus. Urticaria will usually exhibit raised blanching wheals, and pityriasis rosea classically exhibits a herald patch followed by a scaling truncal rash in a fir tree distribution.
Fiberglass is a rare, but important skin irritant. When patients place fiberglass curtains in a washing machine, their clothes subsequently become impregnated with the fibers, causing a severe and vexing pruritus.
Psychological. Pruritus, like pain, is not simply a physiological expression; it has a profound psychological component. No two people react to itching in the same manner. Many factors come into play, including the state of consciousness, attentiveness, and the ability to relieve the sensation by scratching.
Patients with persistent pruritus and no specific diagnosis are often outwardly calm, but hiding feelings of hurt, anger, weakness, and inferiority. These patients may wear their emotions on their skin rather than on their sleeve. Other studies show scratching to represent pent-up resentment or a form of self-punishment. Musaph,[15]after examining hundreds of patients with pruritus of uncertain etiology, feels that itching is a result of thwarted emotion. Many patients scratch without itching as a release of emotional tension. Furthermore, since scratching can produce mild pain, pleasure, and afterglow, Musaph likens the itch-scratch pleasure cycle to a form of autoeroticism. In other patients, it may be a form of self-torture.
It is unclear how tension and repressed emotions are involved in the itching patient. As physicians, it is important to attempt to identify the role these factors play. Telling a patient that the itching is in his or her head will not solve the problem and may create further adverse feelings. The patient should be reassuringly educated to the various roles that emotions play. Serious underlying conflicts, when present, must be evaluated and treated.
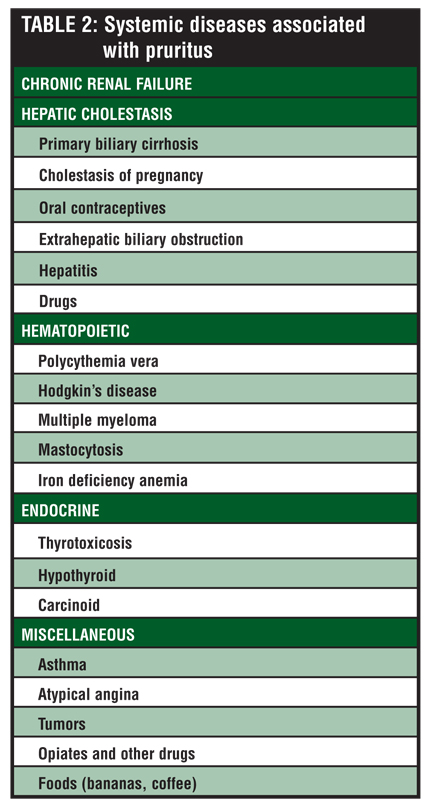
Systemic. The patient with generalized pruritus who presents without obvious dermatological or psychological cause should be evaluated for systemic disease (Table 2).
{kind=link}
Chronic renal failure is an important cause of persistent generalized pruritus. Uremic patients, who now live longer since the advent of hemodialysis, have an increased incidence of pruritus.
Fifty years ago, only 20 percent of patients with uremia developed pruritus; now 80 to 90 percent may eventually develop severe intractable itching.[16] The pruritus may occur anywhere on the body, is not associated with skin lesions, and is only loosely correlated with the degree of uremia. The cause is uncertain, but theories include elevated histamine levels, secondary hyperparathyroidism, and peripheral neuropathy. The ineffectiveness of H1 and H2 blockers implicates an endopeptidase or kinin, which may accumulate. Successful clinical trials with ultraviolet (UV) light suggest a photolabile systemic mediator.
Hepatic cholestasis can cause pruritus in a variety of diseases. Nearly all patients with primary biliary cirrhosis have pruritus, and it can be the presenting manifestation in up to half of all cases. Cholestasis of pregnancy, extrahepatic biliary obstruction, hepatitis, and a number of drugs, including phenothiazines, tolbutamide, erythromycin, and oral contraceptives, can all cause significant pruritus. The itching may be related to an accumulation of bile salt in the skin, although there is no direct correlation. The bile salts may directly affect cutaneous nerves, causing mast cells to release histamine, or may liberate proteases, which subsequently cause pruritus.
A number of unrelated hematopoietic diseases are associated with pruritus. Patients with polycythemia vera frequently have pruritus that is aggravated by hot baths. Fifty percent of patients with Hodgkin’s disease may have pruritus, and in one study, pruritus was considered to be a bad prognostic sign compared with stage-matched patients without pruritus.[13] Multiple myeloma, mastocytosis, and iron-deficiency anemia may also present with itching.
Among the endocrine diseases, thyrotoxicosis is associated with itching in up to 10 percent of patients, especially those with longstanding disease. The increased body temperature, kinins, and vasodilation all play a role. Hypothyroidism probably contributes to pruritus through the associated dry skin. Diabetes is a frequently cited but poorly documented cause of generalized pruritus.[17] The best documented study only had an incidence of three percent, indicating overestimation. Patients with diabetes are prone, however, to pruritus ani and vulvae from candidal infections. Carcinoid syndrome, though rare, can be the cause of pruritus associated with increased histamine and kallikrein levels.
Through a degranulation of mast cells, the opiates may cause pruritus, which may be the presenting complaint of drug addicts. There are case reports of asthma presenting with prodromal itching, atypical angina associated with nasal pruritus, and brain tumors manifesting with ferocious itching of the nostrils.
Diagnostic Approach
Pruritus is a common symptom seen in various skin conditions as well as systemic disorders. Treatment of this symptom is often confounded by the fact that the causes are often multifactorial and involve more than one mediator. Moreover, the etiology is not identified in as many as 50 percent of patients.
When evaluating the patient with significant pruritus, the physician should obtain a careful history, paying attention to the severity and quality of the itching and the influence of environmental factors. The physician should try to assess the patient’s overall psychological state and the degree of disruption of his or her lifestyle. During physical examinations, careful note should be made of primary skin lesions, which may suggest a dermatological diagnosis, as well as secondary lesions from scratching. Persistent rubbing can cause erythema and eventually confluent plaques of lichenified skin, which are indistinguishable from atopic dermatitis. Prolonged scratching can cause the free margin of the nails to become beveled and may aid in the diagnosis when patients are unaware of their scratching. Examination of the skin with dermatographism, defined as the occurrence of a linear wheal at the site of application of stroking of the skin, can be a helpful adjunct if physical urticaria is suspected.
For those patients without overt causes of primary skin lesions who have not responded to an initial short-term course of antipruritic therapy, laboratory workup is recommended. A complete blood cell count with differential can effectively screen for hematopoietic disorders. Serum glucose concentration will exclude diabetes mellitus. Liver function tests are indicated to rule out cholestatic disorders. A basic chemistry panel will evaluate blood urea nitrogen and creatinine along with a urinalysis to detect renal dysfunction. A chest roentogram may show overt mediastinal enlargement associated with Hodgkin’s disease. A thyroid screening test is probably indicated, although it will have a low yield in the absence of suggestive factors and can be considered optional. An HIV antibody test is indicated for patients with historical risk factors.
Treatment
The treatment of pruritus is often an unsatisfactory endeavor for both the patient and the physician. The number of different causes suggests that the treatment will be quite varied. Treatment difficulty is further compounded by the subjective nature of the complaint. In a simple but elegant study, Epstein and Pinski treated patients suffering from pruritic dermatoses with four different tablets.[16] Two-thirds of the patients benefited from at least one of the preparations, although all four tablets were placebo. The placebo effect has been noted as being as high as 50 percent in patients with pruritus, making it difficult to evaluate the efficacy of antipruritic agents.[18]
Skin hydration. Since no antipruritic therapies benefit all patients, patient education is important. Since dry skin has been documented to worsen pruritus, patients with pruritus are advised to keep their skin hydrated by applying bland emollients, such as petrolatum jelly, several times a day. They are also told to apply moisturizers within minutes after drying off from a shower or bath so as to “seal in” the hydrated skin. Patients should avoid hot baths and showers and use only mild soaps, such as Dove or Basis. Avoiding contact irritants, such as cleansing agents, pet dander, and wool or synthetic fabrics, is also advised. Applying cold water or ice compresses is also helpful. By taking these measures, patients can help reduce xerosis (dry skin), thereby reducing the itch-scratch cycle.[19]
Nojima’s study on dry skin in Nishiki cinnamon mice, an animal model simulating atopic eczema, demonstrated that dry skin induced nerve fiber transmission and an increase in the number of nerve fibers in the epidermis. Further differences in skin hydration between the rostral and caudal sites demonstrated that there is communication between the stratum corneum and nerve fibers. These findings open future research related to dry skin and itching.
Documented antipruritic therapies include topical agents, systemic agents, physical modalities, and nonpharmacological treatments for itching.[20]
Antihistamines. Two decades ago, the focus of pruritus treatment was on the antagonism of histamine. Because histamine is the most consistent mediator of pruritus, antihistamines should always be tried. However, antihistamines may act only by sedation[21] and are ineffective in some patients. The two main classes of antihistamines are H1 and H2. H1 antihistamines are further broken down into two categories: first-generation antihistamines with significant sedative and anticholinergic effects and second-generation antihistamines, with decreased sedative properties due to low lipophilicity.[20] Pruritus due to histamine is mediated via H1 receptors; therefore, H1 antihistamines are typically effective for urticaria while H2 antihistamines are generally ineffective in treating itch.
Randomized, controlled trials of second-generation agents, though limited, demonstrated that levocetirizine achieved total wheal and flare inhibition (?95%) with peak wheal inhibition attained at four hours and relatively longer duration of activity at 21.4 hours (P<0.0001).[22]
A single-dose, cross-over trial comparing second-generation agents reported the order of effectiveness, from most to least efficacious as: levocetirizine 5mg > fexofenadine 180mg > mizolastin 10mg > ebastine 10mg > loratadine 10mg > placebo.[30,31] These newer agents exhibit favorable side-effect profiles with no major cytochrome P450 inhibition, limited central nervous system effects, minimal sedation, and minimal motor impairment.[25,26]
Psychotropic agent. Doxepin, a tricyclic compound, typically used to treat depression and anxiety, has been found to exhibit potent H1 and H2 antihistamine and anticholinergic properties. In one study, doxepin was found to be more effective than hydroxyzine or diphenhydramine in relieving pruritus in patients with idiopathic urticaria.[27] Doxepin can be applied topically or given systemically. Its utility is occasionally limited because it causes drowsiness in approximately 25 percent of patients.[20]
Topical therapies. Capsaicin cream.Capsaicin cream can be effective for itching because it desensitizes neurons in the skin by activating the release of substance P from type C nociceptive fibers. However, the major side effect of capsaicin cream is the transient burning sensation secondary to the release of substance P at the application site. This burning sensation has been the cause of nonadherence in 30 percent of patients.[18] Use of the topical anesthetic, lidocaine, prior to applying capsaicin cream may counteract this side effect, but should be limited to only a few days so as to avoid contact dermatitis and systemic absorption resulting in cardiac arrhythmias.[2] Alternatively, more frequent application of capsaicin cream during initial treatment of pruritus can help bring about desensitization in a shorter period of time.[18] Capsaicin has been shown to be effective for localized itching as in nostalgia paresthetica,2 brachioradial pruritus,20 and uremia.[2,28]
Menthol and phenol. Menthol and phenol are agents that have been added to aqueous cream to form a 1 to 2% compound cream that will activate nerve fibers to transmit a cool sensation. This cooling sensation can reduce the perception of itching.[20,29]
Topical corticosteroids. Topical corticosteroids alleviate pruritus that is secondary to inflammatory disorders. However, their usefulness is limited to short-term treatment given that they can cause adverse effects, such as telangiectasia, atrophy, and striae if used long term.[18,29]
Aspirin. A study of the use of topical 3% aspirin solution conducted on patients with chronic localized itch30 demonstrated significant reduction in pruritus.
Salicylic acid. Topical salicylic acid in combination with topical immunomodulators, such as tacrolimus and pimecrolimus, may be effective in reducing itch.
New possibilities in the reduction of itch for patients with atopic dermatitis[3,13,19] include topical agents that inhibit serine proteases and those that inhibit nerve growth factor and neurotrophin.[4]
Opioid receptor antagonists. Controlled clinical trials support the use of opioid receptor antagonists, such as naloxone and naltrexone, for pruritus associated with cholestasis, uremia, and various dermatological diseases.[20,31] It should be noted, however, that there have been conflicting results in clinical trials on the efficacy of naltrexone in uremic pruritus.[32]
Anion exchange resin. Cholestyramine, an oral anion exchange resin, is effective for the relief of biliary pruritus. Its mechanism of action is uncertain, but may be partially related to the removal of bile salts.[16]
Selective serotonin reuptake inhibitor. Fluoxetine, a selective serotonin reuptake inhibitor, has been used in the treatment of cholestatic pruritus.[2,20,29]
Kappa opioid receptor antagonist. A kappa opioid receptor antagonist, nalfurafine (TRK-820), was studied in 92 hemodialysis patients with severe itch and was shown to reduce symptoms. This agent inhibits pruritus and scratching induced by substance P or histamine.[13,20] It is not commercially available in the United States at this time.
Antidepressant. Mirtazapine, an antidepressant that stimulates norepineprhine and serotonin release while simultaneously blocking serotonin receptors, has been used in the treatment of nocturnal pruritus[33] and pruritus associated with lymphoma, cholestasis, and uremia.[2,34] Side effects and drug interactions for this agent are considered minimal, making it a safe alternative for the treatment of pruritus.
Glutamic acid derivative. Thalidomide, a glutamic acid derivative, acts by inhibiting tumor necrosis factor alpha and antagonizing histamine. It is used in chronic pruritus associated with prurigo nodularis, eczema, psoriasis, senile pruritus, and primary biliary cirrhosis.[29] Unfortunately, thalidomide has major adverse effects, including peripheral neuropathy and teratogenicity. Patients taking this medication must be enrolled in the STEPS program (System for Thalidomide Education and Prescribing Safety).[13]
Gamma-aminobutyric acid analogue. Gabapentin, a structural analogue of gamma-aminobutyric acid, blocks the neuropathic afferent pathway. This agent has been used effectively in brachioradial pruritus, multiple sclerosis-induced itch, and neuropathic itch.[13,20,29,30]
Ultraviolet therapy. UVB therapy, especially narrow-band UVB, is effective in pruritus associated with uremia.[2] The results can be quite dramatic, resulting in rapid improvement for patients with severe itch. UVB therapy has also been supported in the treatment of cholestatic pruritus.[18]
Cutaneous field stimulation. Cutaneous field stimulation (CFS) is a new technique that electrically stimulates afferent fibers including nociceptive C fibers. CFS targets unmyelinated C nerve fibers and endogenous central inhibitory mechanisms normally activated by scratching. In a study of patients with localized pruritus, CFS significantly reduced itch and caused degeneration of epidermal nerve fibers.[20] It is most effective in localized disease.
CONCLUSION
Pruritus is a complex, yet not uncommon, phenomenon of great interest to dermatologists and primary care physicians. There is no single mediator of this sensation, and as more is learned about the pathophysiology of this symptom, additional pharmacotherapies have been introduced as discussed in this paper. A thorough history and physical examination enable the physician to separate the causes into dermatologic, psychologic, or systemic. Specific treatments can be undertaken where appropriate and general measures, such as antihistamines and emollients, can also provide significant benefit.
References
1. Tonneson M. Pruritus. In: Fitzpatrick TB, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. New York: McGraw-Hill; 1979:32–34.
2. Twycross R, Greaves MW, Handwerker H, et al. Itch: scratching more than the surface. QJM. 2003;96:7–26.
3. Stander S, Weishaar E, Luger T. Neurophysiological and neurochemical basis of modern pruritus treatment. Exp Dermatol. 2008;17(3):161–169. Epub 2007 Dec 5.
4. Greaves MW, Wall PD. Pathophysiology of itching. Lancet. 1996;348:938–940.
5. Hägermark O. Itch mediators. Semin Dermatol. 1995;14(4): 271–276.
6. Hägermark O. Peripheral and central mediators of itch. Skin Pharmacol. 1992; 5(1):1–8.
7. Rukwied, R Lischetzki, et al. Mast cell mediators other than histamine induce pruritus in atopic dermatitis: a dermal microdialysis study. Br J Dermatol. 2000;142:1–8.
8. Heyer GR, et al. Recent studies of cutaneous nociception in atopic and nonatopic subjects. J Dermatol. 1999;26:77–86.
9. Miyoshi M, Sakurai T, Kodama S. Clinical evaluation of urinary leukotriene E4 levels in children with atopic dermatitis. Areragi. 1999:48(10):1148–1152.
10. Herndon JM Jr. Itching: the pathophysiology of pruritus. Int J Dermatol. 1975;14:465–484.
11. Shelley WB, Arthur RP. Studies on cowhage (Mucuna pruriens): pruritogenic proteinase, mucunun. Arch Dermatol. 1951;72:399–406.
12. Wahlgren CF, Tengvall Linder M, Hägermark O, Scheynius A. Itch and inflammation induced by intradermally injected interleukin-2 in atopic dermatitis patients and healthy subjects. Arch Dermatol Res. 1995;287(6):572–580.
13. Summey BT Jr, Yosipovitch G. Pharmacologic advances in the systemic treatment of itch. Dermatol Ther. 2005;18(4): 328–332.
14. Davidson S, Zhang X, Khasabov SG, Simone DA, Giesler GJ Jr. Relief of itch by scratching: state-dependent inhibition of primate spinothalamic tract neurons. Nat Neurosci. 2009;12(5):544–546. Epub 2009 Apr 6.
15. Musaph H. Psychodynamics in itching states. Int J Psychoanal. 1968; 49:336–340.
16. Rubenstein R. Pruritus: a new look at an old problem. J Fam Pract. 1987;24(6):625–629.
17. Greenwood AM. A study of the skin in 500 cases of diabetes. JAMA. 1927;88:774–776.
18. Yosipovitch G, David M. The diagnostic and therapeutic approach to idiopathic generalized pruritus. Int J Dermatol. 1999;38(12):881–887.
19. Yosipovitch G. Itching in the new millennium: highlights of the Second International Workshop for the Study of Itch, Toyoma, Japan. J Am Acad Dermatol. 2004;51(4):625–627.
20. Bolognia J, Jorizzo J, Rapini R, et al. Dermatology. 2nd ed. Mosby Elsevier; 2008: 91–103.
21. Krause L, Shuster S. Mechanism of action of antipruritic drugs. Br Med J (Clin Res Ed). 1983;287(6400):1199–1200.
22. Purohit A, Melac M, Pauli G, Frossard N. Twenty four hour activity and consistency of activity of levocetirizine and desloratadine in the skin. Br J Clin Pharmacol. 2003;56(4):388–394.
23. Simons FE. Comparative pharmacology of HI antihistamines: clinical relevance. Am J Med. 2002;113 (Suppl 9A):38S–46S.
24. Grant JA, Riethuisen JM, Moulaert B, DeVos C. A double-blind, randomized, single dose, crossover comparison of levocetirizine, with ebastine, fexofenadine, loratadine, mizolastine, and placebo: suppression of histamine-induced wheal-and-flare response during 24 hours in healthy male subjects. Ann Allergy Asthma Immunol. 2002;88(2):190–197.
25. Devillier P, Roche N, Faisy C. Clinical pharmacokinetics and pharmacodynamics of desloratadine, fexofenadine, and levocetirizine: a comparative review. Clin Pharmacokinet. 2008;47(4):217–230.
26. Popov TA, Dumitrascu D, Bachvarova A, et al. A comparison of levocetirizine and desloratadine in the histamine-induced wheal and flare response in human skin in vivo. Inflamm Res. 2006;55(6):241–244.
27. Greene SL, Reed CE, Schroeter AL. Double-blind crossover study comparing doxepin with diphenhydramine for the treatment of chronic urticaria. J Am Acad Dermatol. 1985;12(4):669
28. Breneman DL, Cardone JS, Blumsack RF, et al. Topical capsaicin for treatment of hemodialysis-related pruritus. J Am Acad Dermatol. 1992;26(1):91–94.
29. Lynde CB, Kraft JN, Lynde CW. Novel agents for intractable itch. Skin Therapy Lett. 2008;13(1):6–9.
30. Yosipovitch G, Sugeng MW, Chan YH, et al. The effect of topically applied aspirin on localized circumscribed neurodermatitis. J Am Acad Dermatol. 2001;45(6):910–913.
31. Bigliardi PL, Stammer H, Jost G, et al. Treatment of pruritus with topically applied opiate receptor antagonist. J Am Acad Dermatol. 2007;56:979–988.
32. Pauli-Magnus C, Mikus G, Alscher DM, et al. Naltrexone does not relieve uremic pruritus: