Susun Bellew, DO; James Q. Del Rosso, DO, FAOCD; Valley Hospital Medical Center, Las Vegas, Nevada;
Narciss Mobini, MD; University of Nevada School of Medicine, Las Vegas, Nevada
Abstract
Primary carcinosarcoma is a very rare neoplasm comprising two intermingling malignant components—epithelial and mesenchymal. The authors report a new case of primary cutaneous carcinosarcoma involving the helix of the ear. Immunohistochemical analysis revealed epithelial components of both basal cell and squamous cell carcinomas with a partially ossified sarcomatous-like component.
(J Clin Aesthetic Dermatol. 2009;2(8):33–35.)
Cutaneous carcinosarcoma (CS) is a neoplasm with dual epithelial and mesenchymal malignant components. It is most commonly seen in elderly males on sun-exposed areas of the body.[1–2] The histogenesis of CS is currently under debate. Immunohistochemistry plays an integral part in the diagnosis of this rare biphasic neoplasm. After a review of the literature, the authors were able to find only four other reported cases of CS involving the ear.[1,3 ]They present the fifth case of primary cutaneous CS, which involved the helix of the ear.
Case Report
An 87-year-old woman presented with a 1.5×1.7cm ulceration on the superior helix of the left ear. The patient reported that the original lesion began as a “scab” approximately two years ago, which steadily enlarged with time. A previously performed biopsy indicated basal cell carcinoma (BCC) with probable poorly differentiated squamous cell carcinoma (SCC) component. The lesion bled intermittently secondary to trauma and was very tender to palpation. The patient reported no prior history of skin cancer, no family history of skin cancer, and past medical history did not reveal any major medical disorders.
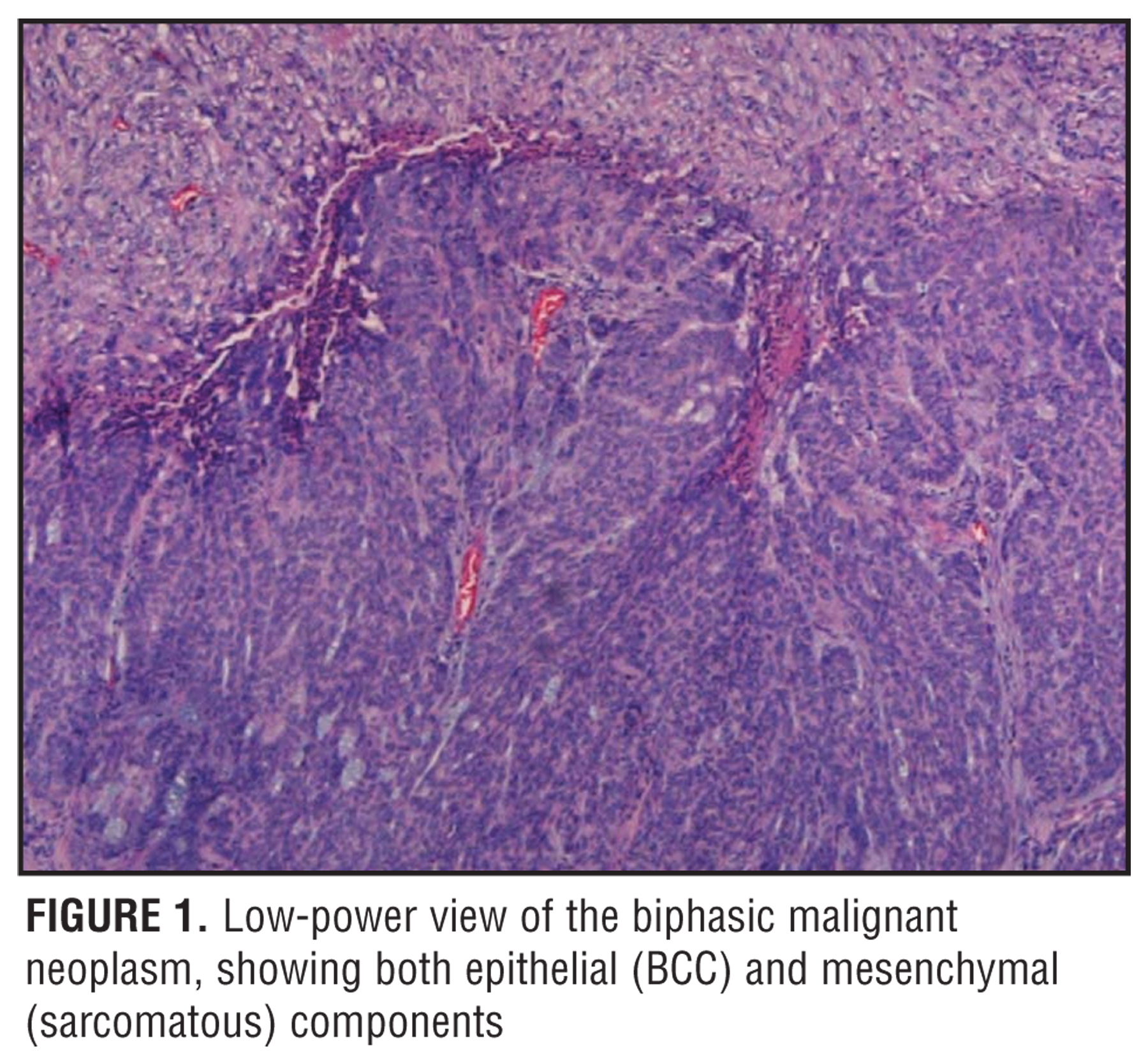
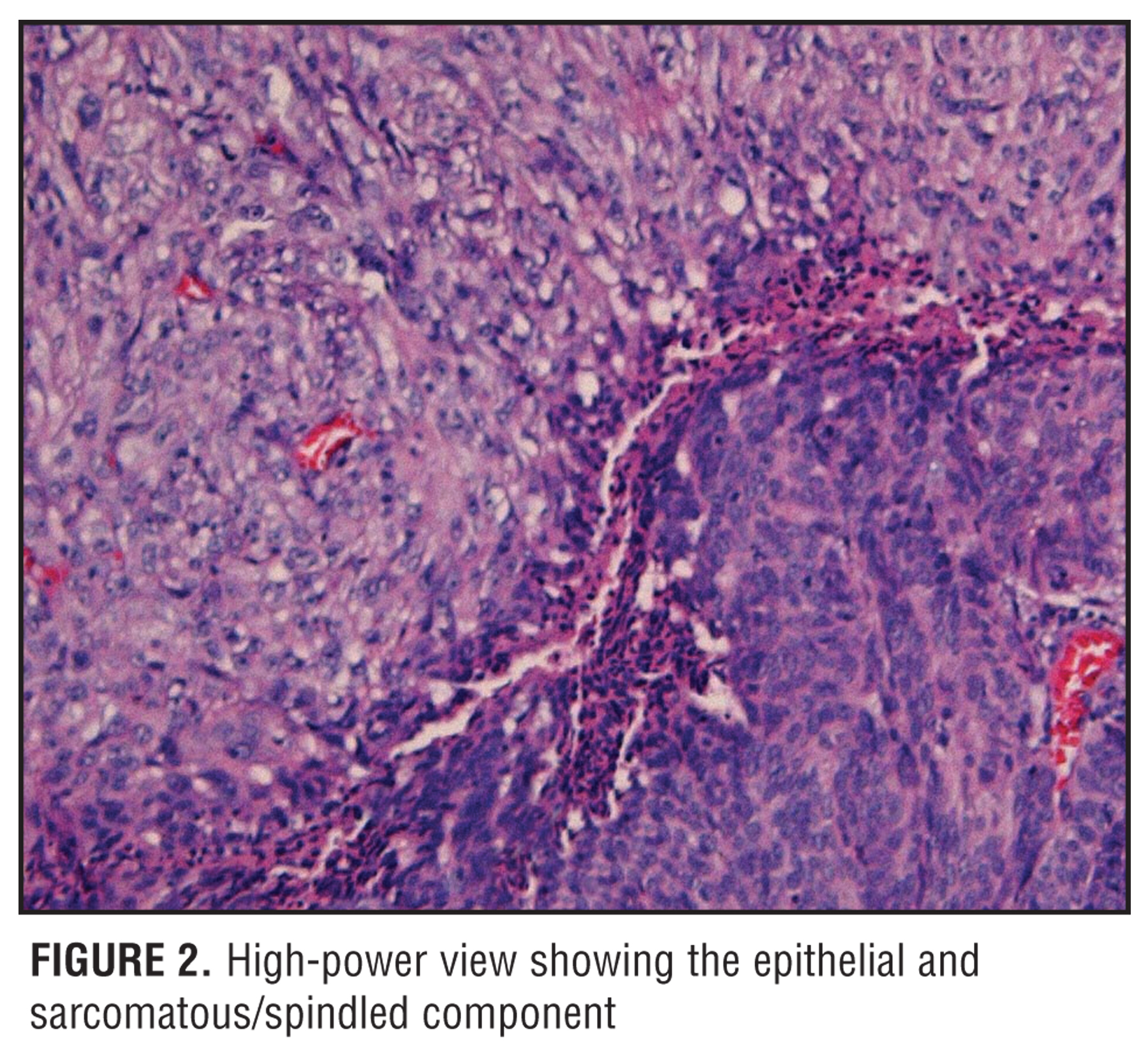
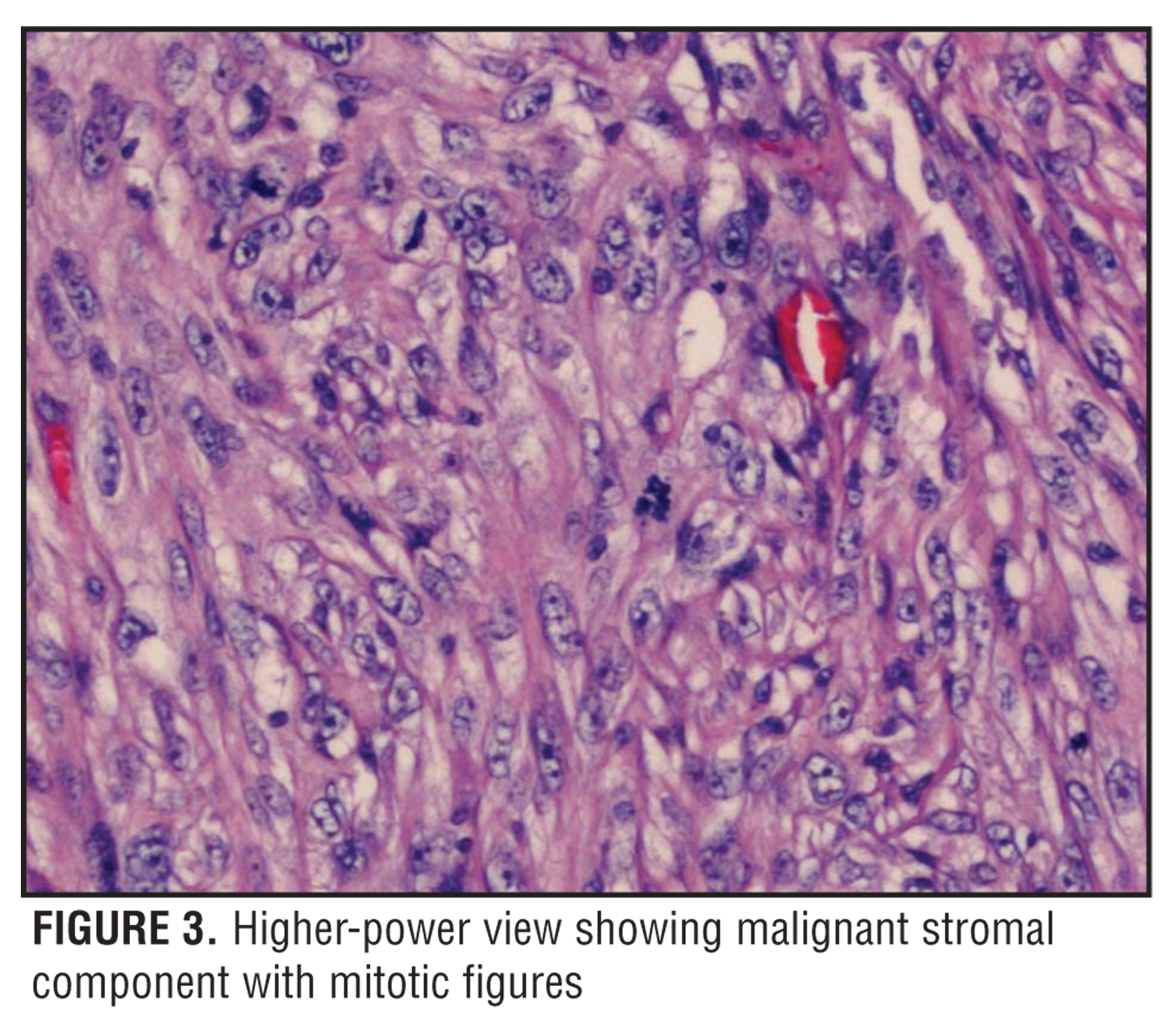
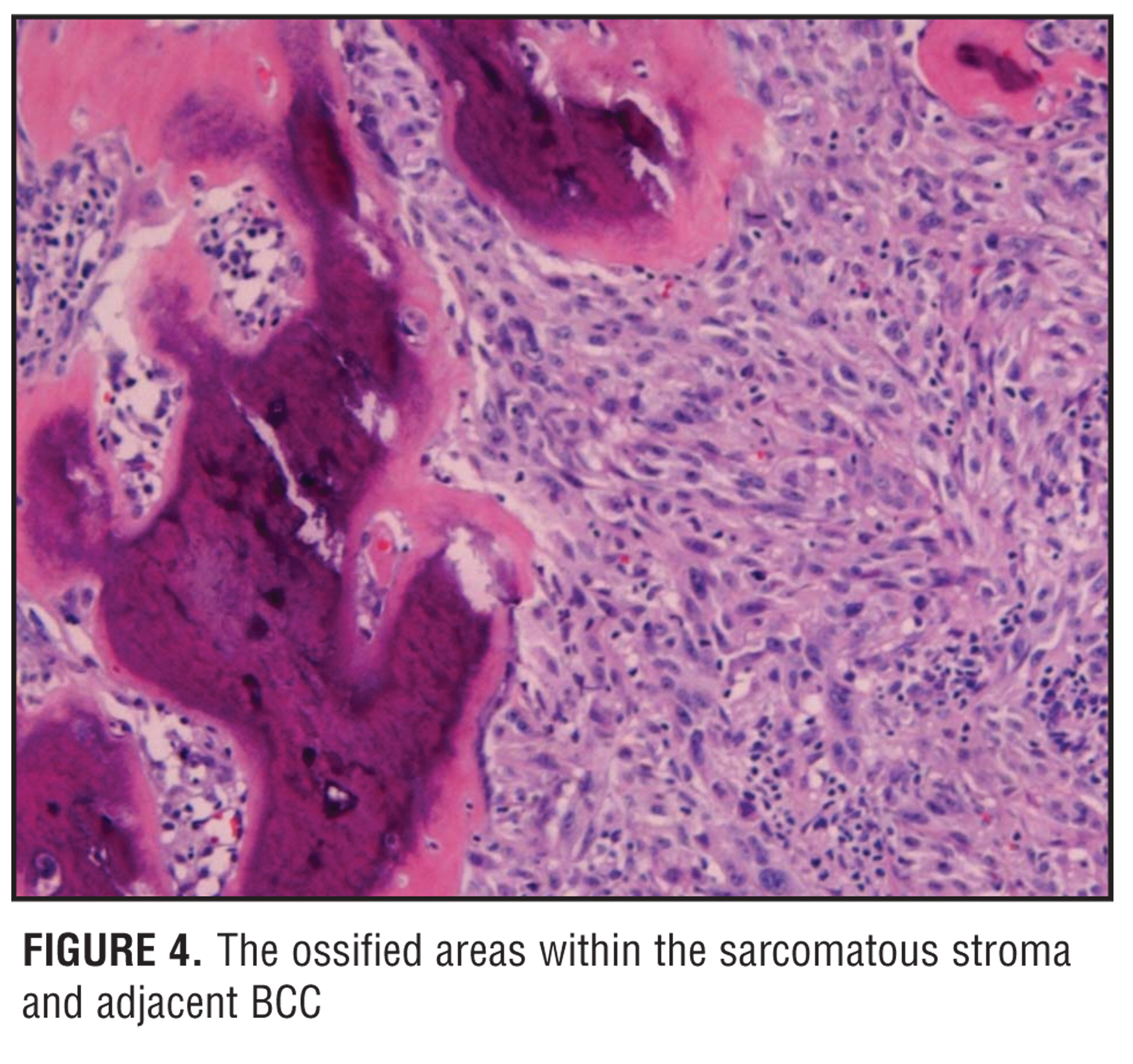
A saucerization biopsy was performed of the current lesion, which displayed a poorly differentiated infiltrative BCC with a possible SCC component. Based on these findings, the lesion was treated with Mohs micrographic surgery (MMS). Initially, a sarcomatous element was not identified; however, histopathologic examination of the central debulked specimen obtained prior to completion of the first stage of MMS revealed an ulcerated biphasic malignant neoplasm (Figure 1 and Figure 2). In addition to classic BCC, most of the lesion comprised a cellular component with an infiltrating pattern of growth showing enlarged and pleomorphic oval to spindle-shaped nuclei and prominent nucleoli with pale amphophilic to eosinophilic cytoplasms, with typical and atypical mitotic figures (Figure 3). The sarcomatous-like stroma was partially ossified (Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical studies revealed that neoplastic cells were positive for vimentin, keratins AE1/AE3, high molecular weight cytokeratin (CK HMW), CK 5/6, and CK MAK6. Cells were focally positive for epithelial membrane antigen (EMA) and negative for S-100, panmelanoma and BerEP4. Furthermore, the spindle cells were positive for vimentin and smooth muscle actin (SMA), and BCC was negative for vimentin and EMA and showed positive reactions to BerEP4 in addition to the other keratin markers. Based on the histologic and immunohistochemical findings, with presence of both epithelial and mesenchymal malignant components, a diagnosis of carcinosarcoma was rendered.
DISCUSSION
Primary CS is a rare tumor consisting of both carcinoma and sarcomatous components.4 The former can further be divided into epithelial components (commonly BCC and/or SCC)[4–6] and adnexal CS comprising benign and malignant spiradenoma, proliferating tricholemmal cystic carcinoma, metrical carcinoma, and porocarcinoma.[1,2] The most frequently occurring sarcomatous components are reported to be atypical fibroxanthoma, osteosarcoma, and chondrosarcoma.[1] A myofibroblastic sarcomatous component has also recently been described.[7] The distinction between epithelial and adnexal CS is an important one as adnexal CS is shown to exhibit a poorer prognosis.[1] The overall, five-year, disease-free, survival rate for adnexal CS is 25 percent as compared to 70 percent for epithelial CS.[1] Other features associated with poorer outcome include tumor size greater than 2cm, recent growth pattern, metastasis to lymph nodes, and a longer history of existing skin tumor.[1] Overall, CS appears to have a more favorable prognosis when compared to CS involving visceral organs.[3,8–9] CS may occur at a variety of other primary sites, including genitourinary tract, lung, breast, salivary glands, gastrointestinal tract, and thymus.[1]
CS occurs more commonly in elderly males with photo-damaged skin, particularly the head and neck region and upper extremities.[1,2] However, skin sites that are not often sun exposed, such as genital skin, have also been reported as sites of CS.[10–12] Most cases present as persistent neoplasms, with or without ulceration, with a noted duration of several weeks to 2 to 3 decades prior to diagnosis.[9] At the time of presentation, most lesions are clinically consistent with BCC or SCC, and are therefore biopsied due to suspicion of malignancy.[1]
Upon review of the literature, only four cases of primary CS involving the ear have been reported.[1,3,13–14] All studies illustrated a BCC and/or SCC epithelial component with mesenchymal components consisting of either atypical fibroxanthoma or osteosarcoma. Treatment was surgical excision in all cases with no reported cases of metastasis.
Immunohistochemical studies are enormously beneficial for diagnosis of CS due its biphasic nature. Moreover, there may be poorly differentiated cells or uneven distributions of cell populations that make definitive diagnosis challenging.13 To that end, studies show that staining for p63, a homologue of the p53 suppressor gene, may be beneficial in confirming cells of epithelial origin in poorly differentiated carcinomas, as this protein is present only in cells with proliferative potential.[14] In other words, p63 would be weakly positive in well-differentiated cells. The converse is true for AE1/AE3, which is strongly expressed in well-differentiated cells and weakly expressed or negative in poorly differentiated SCC. Therefore, it is suggested that testing for p63 and AE1/AE3 may increase the sensitivity for diagnosis of CS.[14]
The histogenesis of primary CS remains unknown at this time; however, four main theories have been postulated.[2,15] Currently, the most widely accepted theory is the conversion theory, which hypothesizes that a portion of an existing carcinoma undergoes a metaplastic transformation into its sarcomatous component. Studies supporting this theory illustrate the presence of p53 tumor-suppressor gene mutations in both mesenchymal and epithelial components of CS.[16,17] Moreover, a transition state from neoplastic epithelial to mesenchymal cells were demonstrated in some reported cases.[16] The composition theory suggests that there is a pseudosarcomatous reaction by the stromal component to the presence of the carcinoma. The collision tumor theory suggests that entirely separate independent tumors collide in one common site for development. Lastly, the combination theory argues that a common pluripotential progenitor cell gave rise to both epithelial and sarcomatous components. Based on available literature to date, the underlying histogenesis of primary CS remains controversial.[2,15–17]
SUMMARY
Primary CS is an exceedingly rare malignant neoplasm comprising both epithelial and mesenchymal components. The present case illustrates the biphasic nature with BCC and poorly differentiated SCC intermixed with a partially ossified sarcomatous-like counterpart. Immuno-histochemical studies are important for the diagnosis of CS, especially in lesions that have uneven distributions of cell populations and in those that are poorly differentiated. To this end, staining for p63 has been shown to be beneficial in supporting a diagnosis of CS. Overall, CS has a more favorable prognosis when compared to CS involving other organs. Here, the authors present the fifth reported case of CS of the ear and emphasize the crucial role of biopsy, along with both histopathologic and immunohistochemical examination, in order to confirm the diagnosis of this rare neoplasm.
References
1. Tran TA, Muller S, Chaudahri PJ, Carlson JA. Cutaneous carciniosarcoma: adnexal vs. epidermal types define high- and low-risk tumors. Results of meta-analysis. J Cutan Pathol. 2005; 32:2–11.
2. Bigby SM, Charlton A, Miller MV, et al. Biphasic sarcomatoid basal cell carcinoma (carcinosarcoma): four cases with immunohistochemistry and review of the literature. J Cutan Pathol. 2005;32:141–147.
3. Vincek V, Mirzabeigi M, Jewett B, et al. Primary carcinosarcoma of the helix of the ear. Ear Nose Throat J. 2005;84(11):712–725.
4. Quay SC, Harrist TJ, Mihm MC. Carcinosarcoma of the skin. Case report and review. J Cutan Pathol. 1981;8:241–246.
5. Isaki S, Hirai A, Yoshizawa Y, et al. Carcinosarcoma of the skin: immunohistochemical and electron microscopic observations. J Cutan Pathol. 1993;20:272–278.
6. Rios-Martin JJ, Parra-Martin JA, Gomez-Pascual A, et al. Sarcomatoid carcinoma of the skin: report of a case. J Dermatol. 1998;25:314–321.
7. Agostini T, Mori A Leporatti G, et al. Cutaneous carcinosarcoma: report of a case with myofibroblastic sarcomatous component. Dermatol Surg. 2008:34(3):418–422.
8. Patel NK, McKee PH, Smith NP, et al. Primary metaplastic carcinoma (carcinosarcoma) of the skin. A Clinico-pathologic study of four cases and review of the literature. Am J Dermatopathol. 1997;19(4):363–372.
9. Brown TJ, Tschen JA. Primary carcinosarcoma of the skin: report of a case and review of the literature. Dermatol Surg. 1999;25:498–500.
10. Antonini C, Zucconelli R, Forgiarini O, et al. Carcinosarcoma of penis. Case report and review of literature. Adv Clin Path. 1997;1:281.
11. Carter C, Lesna M, Rundle J. Carcinosarcoma of the penis. J Pathol. 1995;175:132A.
12. Parham DM, Morton K, Robertson AJ, Philip WD. The changing phenotypic appearance of a malignant vulval neoplasm containing both carcinomatous and sarcomatous elements. Histopathology. 1991:19:263.
13. Leen EJ, Saunders MP, Vollum DI, et al. Carcinosarcoma of skin. Histopathology.1995;26:367–371.
14. Gomez-Espejo C, Herrera-Sabal A, Rios-Martin J, et al. Basal cell carcinoma with sarcomatoid features (sarcomatoid carcinoma): report of a case and review of the literature. J Dermatol. 2003;30:543–549.
15. Romanelli P, Miteva M, Schwartzfarb E, et al. P63 is a helpful tool in the diagnosis of a primary cutaneous carcinosarcoma. J Cutan Pathol. 2009;36(2):280–282.
16. Suh KY, Lacouture M, Gerami P. p63 in primary cutaneous carcinosarcoma. Am J Dermapathol. 2007;29(4):374–377.
17. McCluggage WG. Malignant biphasic uterine tumours: carcinosarcomas or metaplastic carcinomas? J Clin Pathol. 2002;55:321–325.
18. McMenamin ME, Goh SG, Poblet E, et al. Sarcomatoid basal cell carcinoma—predilection for osteosarcomatous differentiation: a series of 11 cases. Am J Surg Pathol. 2006;10:1299–1308.
19. Kounelis S, Jones MW, Papadaki H, et al. Carcinosarcomas (malignant mixed mullerian tumors) of the female genital tract: comparative molecular analysis of epithelial and mesenchymal components. Hum Pathol. 1998;29:82–87.