Joseph Fowler Jr., MD, FAAD; Lynn Fowler, RN, BSN
Dermatology Specialists Research, PSC, Louisville, Kentucky
Disclosure: Dr. Fowler serves on the Speakers Bureau and is a consultant for Ranbaxy and many other dermatology companies. Ms. Fowler reports no relevant conflicts of interest. Financial support for this study was provided by Ranbaxy.
Abstract
Objective: To assess the clinical outcomes of triamcinolone acetonide spray for steroid-responsive dermatoses using investigator and patient global assessment scores and evaluate patient satisfaction. Design: This open-label, single-center, noncomparator study enrolled 42 patients (aged 18 years or older) with dermatoses. Patients were instructed to use triamcinolone acetonide spray 1 to 4 times daily, depending on investigator instructions, for up to 28 days. Measurements: Investigators and patients scored the overall severity of dermatoses based on a global assessment scale. Investigators also rated signs and symptoms of dermatoses and evaluated clinical outcomes based on an improvement assessment scale. Patient satisfaction with treatment was assessed at the end of treatment or at Day 28 using a questionnaire. Patients were evaluated on Days 7, 14, 21, and 28. Complete clearing of dermatoses warranted early discontinuation from the study. Results: Triamcinolone acetonide spray effectively improved dermatoses scores, clinical outcomes, and signs and symptoms of dermatoses. More than 80 percent of patients entered the study with moderate or severe dermatoses. Within 14 days, none had severe dermatoses, and by 28 days, 64 percent of patients were completely clear or almost clear. From the patient perspective, 51.3 percent experienced improvement in only three days, and 84.6 percent experienced improvement in seven days. An overwhelming number of patients (95%) preferred triamcinolone acetonide spray over creams and ointments, and more than half experienced a cooling effect upon contact with the spray. Conclusion: Triamcinolone acetonide spray is an effective topical corticosteroid that should be considered for patients with steroid-responsive dermatoses of all ranges of severity. (J Clin Aesthetic Dermatol. 2010;3(5):27–31.)
The vast majority of topical agents prescribed in dermatology are creams and ointments—two vehicles associated with a variety of concerns from the patient’s perspective. Soiling and/or staining of fingers and clothing, inconvenience of application to certain body areas, difficulty of even distribution and application over extensive areas of the body, occasional formation of a film at the application site that prevents air circulation and may lead to discomfort, and the inability to apply consistent amounts of medication are all commonly associated with the use of creams and ointments and greatly affect patient satisfaction and adherence to therapy.[1] Housman et al conducted a quantitative assessment of vehicle preference in patients with psoriasis and reported that these patients preferred solutions and foams over creams, gels, and ointments.[2] They found a good correlation between quality-of-life measure and vehicle preference, suggesting that the characteristics of solutions and foams may favor improved adherence to topical therapy.
Triamcinolone acetonide is a mid-potency, class 4/5 topical corticosteroid that is available in a spray formulation (Kenalog® Spray, , Ranbaxy Laboratories, Inc). It is indicated for the relief of inflammatory and pruritic manifestations of corticosteroid-responsive dermatoses. Unlike more potent corticosteroid products, Kenalog® Spray has no time limitations on its use; therefore, it is commonly used to treat flares in eczema, psoriasis, atopic dermatitis, seborrheic dermatitis, and contact dermatitis.[1,3]
In contrast to creams and ointments, triamcinolone acetonide spray can easily cover large and hard-to-reach areas of the body. Its optional nozzle directs application of the medication to precise areas without affecting nearby areas. Patients requiring a mid-potency corticosteroid for lesions on the scalp, back, intertriginous folds, large areas, or areas that require precise application would benefit from the triamcinolone acetonide spray formulation. In the time since the introduction of Kenalog® Spray in dermatology, other topical corticosteroids have entered the market, but Kenalog® Spray remains the only mid-potency corticosteroid available in a spray formulation. Spray formulation may provide patients and physicians with advantages over creams, ointments, foams, and solutions. It was the aim of this study to assess the clinical outcomes of triamcinolone acetonide spray for steroid-responsive dermatoses using investigator and patient global assessment scores and evaluate patient satisfaction with this spray formulation.
STUDY DESIGN
This open-label, single-center, noncomparator study was designed to evaluate the clinical outcomes of triamcinolone acetonide spray based on physician and patient assessments. A total of 42 patients were enrolled.
Patients were diagnosed and enrolled at the first visit (baseline), based on the following inclusion criteria:
• Men and women, 18 years of age and older and in good general health, as confirmed by a medical history
• Steroid-responsive dermatoses with target severity score between 2 and 5, as determined by the investigator
• Negative urine pregnancy test for women of childbearing potential
• Use of effective birth control by women of childbearing potential
• Patient understanding of study requirements, agreement to follow study instructions and return for required examinations
• Signed informed consent prior to study procedures.
Exclusion criteria were as follows:
• Age less than 18 years
• Women who were pregnant or nursing
• Known allergy to or contraindications to the study medication
• Use of topical corticosteroids or calcineuron inhibitor medication for dermatosis within one week of study start
• Oral corticosteroids or oral immunosuppressive agents within two weeks of study start
• Phototherapy within two weeks of study start
• Intramuscular injection of corticosteroids within four weeks of study start.
Study medication and administration. Patients were given one unit of the study medication (Kenalog® Spray 63g) and instructions for its application and use at the baseline visit. Additional units were distributed at the discretion of the investigator.
The amount of medication applied was based on the percentage of body surface area to be treated (e.g., a 2-second application of triamcinolone acetonide spray is sufficient to cover the hand). Triamcinolone acetonide spray was applied 1 to 4 times daily as per the investigator’s instructions. Most patients were instructed to apply the medication 1 or 2 times daily. When appropriate, patients were told to use the optional nozzle.
Patients were examined every seven days for 28 days and evaluated for improvement in their conditions based on an Investigator and Patient Global Assessment Scale and Physician Assessment Improvement Score. Patient satisfaction with treatment was assessed using a questionnaire completed at the end of treatment or at four weeks, whichever occurred first.
Evaluation. Patients used triamcinolone acetonide spray for a total of 28 days. If dermatoses cleared completely, then treatment was stopped prior to 28 days.
Baseline. Investigators and patients scored the overall severity of dermatoses based on the following global assessment scale: 0=clear, 1=almost clear, 2=mild, 3=moderate, 4=severe, and 5=very severe. A score of 2 to 5 was required for enrollment into the study.
Investigators rated signs and symptoms of erythema, papules/vesicles, excoriation, pruritus, and burning/stinging using the following scale: 0=clear, 1=mild, 2=moderate, and 3=severe.
Follow-up visits. At each follow-up visit, investigators and patients rated the severity of dermatoses, and investigators rated signs and symptoms based on the scales listed above. A global assessment score of 0 at any of the follow-up visits (Day 7, 14, or 21) warranted early discontinuation from the study.
Investigators also evaluated clinical outcomes at these follow-up visits based on the following improvement assessment scale: 0=complete clearing, 1=marked, improvement (> 75% overall improvement from baseline), 2=moderate improvement (25–75% overall improvement from baseline), 3=mild improvement (<25% overall improvement from baseline), and 4=no response/worsening.
Patient satisfaction with treatment was assessed at the end of treatment or at Day 28 using a questionnaire.
RESULTS
Patient demographics. Total enrollment in this clinical study was 42 patients; 39 patients completed the trial and three discontinued early due to unrelated adverse events requiring prohibited medications. Slightly more than two-thirds of patients were women (69%) and 31 percent were men. The average age was 51 years. Most patients (48%) were between the ages of 41 and 59 years, 21 percent were between the ages of 18 and 40 years, and 31 percent were age 60 years and older. The majority of patients was Caucasian (79%), followed by African American (19%), and Asian (2%). Sites of dermatoses included scalp, elbow, arms, hands, legs, trunk, and neck.
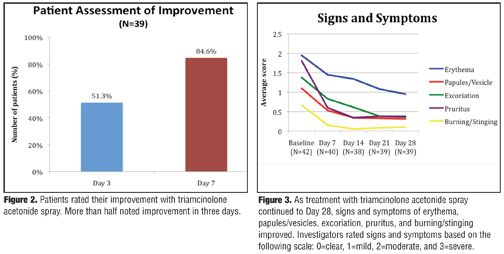
Investigator and patient global assessment. At baseline, the majority (83%) of patients exhibited dermatoses rated as severe (score of 4) or moderate (score of 3) by the investigator (Figure 1a). Only 17 percent of patients had mild dermatoses. After using triamcinolone acetonide spray for 14 days, a third of patients (32%) were completely clear or almost clear of dermatoses; none had severe dermatoses (Figure 1b). Patients continued improving to Day 28—twice as many (64%) patients were completely clear or almost clear compared with 14 days earlier, and none had severe dermatoses (Figure 1c). At this time, 87 percent were clear, almost clear, or had mild dermatoses. Patient assessment of improvement was in line with these results. At baseline, 72 percent of patients assessed their dermatoses as moderate or severe. By Day 28, 89 percent assessed their dermatoses as completely clear, almost clear, or mild. One-half of patients noted improvement by Day 3, and more than 8 out of 10 patients reported improvement by Day 7 (Figure 2).
{kind=link}
{kind=link}
Signs and symptoms of dermatoses. Signs and symptoms of erythema, papules/vesicles, excoriation, pruritus, and burning/stinging decreased over the course of treatment (Figure 3). At baseline, most patients (67%) had moderate erythema. By Day 28, erythema was absent or nearly absent in 77 percent of patients. Similar results were seen with papules/vesicles, excoriation, and pruritus—the majority of patients who had moderate or severe levels of these symptoms at baseline improved to complete or almost complete clearing by Day 28. For burning/stinging, 24 percent of patients had moderate or severe levels at baseline and none had moderate or severe levels by the end of the study period.
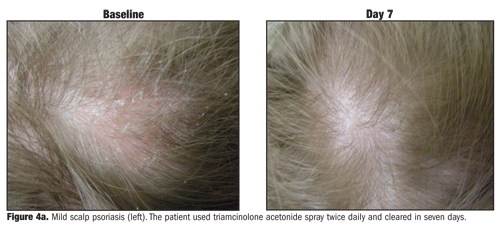
Clinical outcomes. Seven days of treatment with triamcinolone acetonide spray led to a third of patients showing complete clearing of dermatoses or at least 75-percent improvement. By Day 28, two-thirds of patients achieved the same levels of improvement; an additional 21 percent had moderate improvement at this time. Only 1 out of 39 patients experienced no response or worsening of dermatoses by the end of the study period. Figure 4a and Figure 4b document clinical improvement in two patients—one who used triamcinolone acetonide spray twice daily for scalp psoriasis and cleared in seven days (Figure 4a) and the other who used triamcinolone acetonide spray twice daily for leg psoriasis (Figure 4b).
Patient satisfaction. Based on end-of-study questionnaires, more than 9 out of 10 patients preferred triamcinolone acetonide spray over creams and ointments, citing “no residue,” “easier to apply,” “not greasy,” “fast drying,” and “not sticky.” Nearly all patients would use triamcinolone acetonide spray in the future. More than half experienced a cooling effect upon contact with the spray (Figure 5).
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Triamcinolone acetonide spray has been used for more than 35 years and continues to be a highly effective topical corticosteroid with unique advantages. It contains 0.2% triamcinolone compared to 0.1% triamcinolone, which is found in most creams and ointments. The spray formulation eliminates the messiness of creams and ointments, allows simple, even application to large areas of the body, and when used with the optional nozzle, allows precise application to distinct areas. In addition, the spray does not drip and allows for no-touch, no-rub application, which is valuable when treating inflamed or infectious skin. To the surprise of investigators, triamcinolone acetonide spray provided a cooling, anti-pruritic effect on inflamed skin despite its alcohol base. All of these benefits, however, do not compromise its efficacy.
This study demonstrated that triamcinolone acetonide spray effectively improved dermatoses scores, clinical outcomes, and signs and symptoms of dermatoses when used 1 to 4 times daily for up to 28 days. More than 8 out of 10 patients entered the study with moderate or severe dermatoses. Within 14 days, none had severe dermatoses, and by 28 days, 6 out of 10 patients were completely clear or almost clear. From the patient perspective, 51.3 percent experienced improvement in three days, and 84.6 percent experienced improvement in seven days. An overwhelming number of patients (>90%) preferred triamcinolone acetonide spray over creams and ointments since it was easy to apply, not greasy, fast drying, and not sticky. Patients also preferred triamcinolone acetonide spray because it allowed for much shorter treatment times, compared to previous therapies. In addition, more than half experienced a cooling effect upon contact with the spray.
The authors conclude that triamcinolone acetonide spray is an effective topical corticosteroid that should be considered for patients with steroid-responsive dermatoses of all ranges of severity. Its cooling effect helps provide immediate relief and its spray formulation is an advantage when treating extensive areas or distinct areas when used with the optional spray nozzle.
References
1. Singer JI. Triamcinolone acetonide in an aerosol spray: effectiveness as topical therapy for various dermatoses. J New Drugs. 1961;1:238–243.
2. Housman TS, Mellen BG, Rapp SR, Fleischer AB Jr., Feldman SR. Patients with psoriasis prefer solution and foam vehicles: a quantitative assessment of vehicle preference. Therapeutics Clinician. 2002;70:327–332.
3. Goldner R. Triamcinolone acetonide spray (reformulated) in the treatment of topical steroid-responsive dermatoses. Int J Dermatol. 1981;20:659–661.