Matthew J. Zirwas, MD; Jessica L. Holder, BS, Department of Internal Medicine, Division of Dermatology, The Ohio State University College of Medicine, Columbus, Ohio
Abstract
Patient education is an important aspect of patient care in dermatology. Successful education increases patient satisfaction and results in improved outcomes and adherence. This article individually evaluates several patient-education strategies: verbal education, written information, group-based learning, audiotapes, videotapes, computer-assisted education, and the internet. The review presents the strengths and limitations of each strategy based on recognized barriers to effective patient education that were discussed in Part 1. Additionally, a summary of recommendations for effective patient education is provided. (J Clin Aesthetic Dermatol. 2009;2(12):28–34.)
In Part 1 of this review of patient-education strategies in dermatology, the authors examined evidence supporting the use of patient education to benefit patient care. Additionally, they analyzed barriers, such as illiteracy, information overload, and physician time, which can hinder effective patient education. Successful education is ultimately dependent on choosing an effective method of education that is appropriate for the given patient. Therefore, in Part 2 of this review, the authors focus on individual patient-education strategies and their inherent strengths and weaknesses. In evaluating and discussing the different methods of patient education, the authors hope to create a better understanding of what generates optimal patient education.
Specific Patient-Education Strategies
In order to analyze and evaluate individual education strategies, the most commonly used methods are presented in this article. The techniques are organized from the more standard to the more modern approaches. Their strong points and limitations are summarized in Table 1.
{kind=link}
Verbal. The most traditional form of patient education is the one-on-one exchange of information that occurs between physician and patient. Dent[1] refers to spoken advice as the “gold standard” of patient education. A 2008 survey of patients with irritable bowel syndrome found that individualized information received directly from their providers was most desirable.[2] In order to be successful, almost every patient-education strategy—printed material, computerized program, or video—needs to be supplemented with some degree of verbal support from the physician. Treatment of asthma patients with written action plans has been found to be relatively unsuccessful in the absence of any verbal support.[3] Additionally, in a study by Hill et al,[4] education about rheumatoid arthritis medications resulted in improved pharmacologically measured adherence only when receiving verbal support in addition to a pamphlet. Communicating with a patient verbally allows the physician to adapt education based on the response of the patient. Additionally, the physician can individualize information to be directly relevant.[1] In the management of atopic dermatitis, patients typically respond better when they receive individualized advice and personalized ways of incorporating management into their lives.[5] Brief educational messages by telephone, usually as follow up, have also been shown to be an effective, quick use of verbal communication that increases adherence in patients.[1,6]
Compared to alternative education strategies, exchange of information verbally is significantly more time consuming and costly.[1,7]
Additionally, patients may struggle with recall if information is only presented to them verbally. Speaking to the patient in the presence of family or caregivers may not only increase recall but also alleviate anxiety.[8] When presenting information verbally, physicians should organize and highlight the most important concepts and speak concretely. Verbal presentation is the most effective for communicating new information.[6] Although patient recall for numbers is poor, presenting probabilities using exact numbers rather than words helps patients understand.[9] Specific directions are more helpful than general suggestions.[3,5–6] Isaacman et al10 evaluated the impact of standardized verbal and written instructions upon discharge of otitis media patients from the hospital. Patients were either discharged normally from the hospital or received written and/or verbal standardized instructions by trained housestaff. There was significantly improved recall of medications and dosages in patients receiving either verbal or verbal and written standardized instructions.[10] To alleviate the physician time demand, nonphysicians in the office may be trained to present verbal education to patients. While this does not increase patient-physician interactions specifically, it does provide direct support and personalized information from another member of the healthcare team.
Verbal information lies at the foundation of patient education, especially in dermatology where personalized information is of extreme importance. Direct conversation with patients is not only an effective education strategy alone, but it bolsters additional education strategies. It seems especially beneficial in scenarios where new information is presented in order to afford patients the opportunity to ask questions and get feedback. Furthermore, one-on-one interaction allows the dermatologist to assess the literacy level of the patient, note any cultural barriers, and identify and alleviate any anxiety or doubt the patient may be experiencing. Purely verbal communication in educating patients may be limited by the time-consuming nature of direct conversation, poor recall, and cost. Since verbal information has no finite limitation in length, it also may predispose patients to information overload. For these reasons, it may be advantageous for dermatologists to use additional members of the healthcare team to deliver verbal education and to combine verbal messages with additional education techniques.
Written. According to the same survey of irritable bowel syndrome patients in 2008, written education materials were the least preferred mode of information by patients.2 However, in other instances, written information seems to satisfy patients and, in acute cases, decrease anxiety.[6,11] Regardless, written materials continue to be a cost-effective, easy intervention to increase patient education.[6] The National Heart Lung and Blood Institute (NHLBI) recommends that asthma patients receive written goals, medication dosages, and actions to take during an exacerbation. However, they also stress the importance of personalized reinforcement in addition to written materials.[3] Similar to the recommendation for written action plans in asthma patients, specific verbal and written information on nut avoidance for those with nut allergies has been found to be effective.[12] Isaacman[10] found that written information combined with verbal information upon discharge compared with purely verbal information showed slight increases in recall ability three days later. However, the difference was not statistically significant.[10]
Written information concerning a patient’s diagnosis and treatment has little meaning or impact if the patient does not receive any personalized, direct information from the physician.[13] Printed materials that have been tailored to the patient’s age, race, or stage of disease are more likely to be read and understood, especially by certain groups.[14] Skinner et al[14] studied the effects of personalized letters mailed to patients for mammography and found that letters addressing the patient’s age, race, and other characteristics seemed to be more effective in African-American patients and patients coming from lower economic backgrounds. Interestingly, patients were more likely to remember receiving and reading the letters despite there being no statistically significant differences in mammogram usage with the tailored letters.[14,15] It is important that printed information be readable, and it should always be engaging or interactive for the patient. For example, Tschopp et al[16] found that creating a multidisciplinary informative brochure and coupling it with a personalized patient notebook created both a multidisciplinary and individualized approach to effectively teach patients. The 12-month study in Sweden resulted in improved quality of life, decreased utilization of the health system, and improved severity of asthma.[16]
Newsletters can be a method of broadly communicating to a group of patients and continually updating patients in a world of rapidly developing and changing healthcare.[1] Additionally, office posters with brief educational messages have been established as effective ways of reaching large numbers of people.[6]
Because of the prevalence of illiteracy in the general population, it is important to keep writing levels below the eigth-grade level; keeping the level below the fifth- or sixth-grade level may be even better.[17,18] Despite these recommendations, most printed patient-education materials are written for the high school and even college levels.[18] In fact, it has been found that all patients, regardless of literacy level, prefer easier-to-read materials when it comes to healthcare. In a study of polio vaccine pamphlets, patients of all literacy levels preferred a simple brochure with illustrations instead of the longer Centers for Disease Control and Prevention (CDC) version.[19] Lists rather than paragraphs and concrete instructions written in active conversational writing rather than passive writing have been found to be more effective.[20,21] Wilson and Williams[17] evaluated a small assortment of pamphlets educating patients on pressure ulcers and skin care that were commonly used in urban hospitals and clinics in Midwestern United States. They found that, overall, the average reading level of material was around tenth grade, and only 5 of the 10 sources evaluated were under the recommended eigth-grade level. Additionally, none of the sources were able to be tailored to different races, sex, or ages, and they rarely contained summaries or categorized information. While a variety of formulas exist to calculate readability, most are based on number of words per sentence and number of syllables per word.[17] The generally high reading levels of printed patient-education sources make them impossible to understand for many patients, and even more literate patients may struggle with recall when reading at such advanced levels.
Like verbal information, written materials have been a long-standing method of educating patients. Written information can be mass distributed, making it time and cost effective. While it seems logical that written material would improve recall and adherence, the actual effectiveness of written materials is not clear in the literature. It is important to note that most of these studies evaluated short-term recall as opposed to long-term recall. Perhaps written materials would increase long-term recall and adherence by providing patients with reliable sources of information to fall back on when physicians are not available. However, if reading materials are not created at an appropriate level with techniques to increase readability, it seems wasteful to even print the materials for patients. One must also keep in mind that the value of written materials from a clinical standpoint and a research standpoint cannot truly be determined since there is no proof that patients actually read the information.[10] It seems most advantageous to use written materials to communicate specific and standardized instructions to patients. When utilizing pamphlets to supplement patient education, strive to create reading levels below the eigth-grade level with categorized information and images when possible.
Group education. Self-management programs and support networks are patient-education strategies that may be helpful for the long-term management of chronic conditions. Peer groups have been shown to provide good social support in adolescent asthma patients, and support groups have also been used successfully in patients with atopic dermatitis.[3,5] Group sessions are often cost and time effective, and they provide nonthreatening venues for patients to share education, ideas, and support.[13]
Self management is the concept of an individual effectively taking care of his or her chronic disease physically and psychologically. Self-management programs emphasize education, following protocols for treatment, behavioral modification, and building self confidence. Oftentimes, these programs are led by trained individuals who also suffer from chronic diseases.[22] Modular behavioral arthritis programs that utilize cognitive, behavioral, and educational components have been shown to be more effective in managing disease compared with purely information-based programs.[23] Additionally, an assortment of different chronic diseases can to be managed within one self-management based intervention.[22]
Because many dermatological complaints involve complex treatment regimens and behavioral modifications, self-management programs may be helpful. They have the advantage of alleviating anxiety and providing continuous support systems without taking dermatologists’ time. Furthermore, since several different diseases can be managed within one program, it could potentially be useful for any chronic disease management. Language and cultural barriers may exist depending on the type of group, and the education gained may be more supportive rather than informative. Ultimately, education in the form of self-management programs may not be suitable for every patient, but for patients who are interested or lack support systems, it is a useful supplement to more traditional forms of patient education.
Audio. As with written patient information, audiotapes have the advantages of being simple to distribute, not requiring increased time from the physician, and avoiding the issues of readability encountered with written materials. Despite the proposed benefits, audiotapes have been associated with mixed outcomes in patient knowledge and understanding. Schaffer’s study of patient education in asthmatics found no significant differences in education by audiotape or written material. However, both audiotape and written material were more effective than no additional educational materials.[24] Bader et al[25] found that audio was the least preferred method of education even though it was equally as effective as other modes of education in increasing patient knowledge about cancer.
In a randomized, controlled trial, Bruera et al[26] found that audiotapes in addition to written information were superior to only written information when counseling newly diagnosed cancer patients. The addition of the audiotapes not only increased patient knowledge, but also improved patient satisfaction.[26] Similarly, providing audiotapes of conversations to mothers of babies in the neonatal intensive care unit in addition to standard verbal patient counseling was found to increase recall of information four months after the encounter and improve patient satisfaction.[27]
It seems logical that audiotapes would increase recall and satisfaction in patients. They provide information without relying on literacy and give patients the ability to review information repeatedly if necessary. Furthermore, they can be created in any number of languages to reach separate patient populations. However, as educational methods, audiotapes have been accepted with mixed results. Effectiveness ultimately depends on whether patients actually listen to the audiotapes, which is most likely dictated by personal preference. The lack of interaction involved in listening to an audiotape and the mixed appeal that audiotapes have may contribute to nonadherence with audiotapes and, therefore, failed patient education.
Video. Videotapes provide the advantages of audiotapes in addition to the effect of visual stimulation. They are growing in popularity in clinical practice and are increasingly being studied. Home use of videotapes is especially effective because it alleviates anxiety as a confounding factor and allows for unlimited repetition, both of which have been found to effect recall.[8]
Two subsequent studies by Volk et al[28,29] evaluated the use of educational videotapes for the risks and benefits of prostate specific antigen (PSA) testing. Brief 20-minute videos compared with brochures were initially found to increase knowledge and decrease intended use of PSA screen. In a follow-up study, the researchers re-evaluated patients one year after the 20-minute educational video and found continued decreases in PSA screening in patients educated by the videotapes. They concluded that educating patients on the risks and benefits of PSA screening using videotapes resulted in changed behaviors that persisted up to one year after intervention.[28,29] Similar results have been found using videotapes to educate patients that will be undergoing anesthesia. Use of a standardized videotape in addition to undergoing the typical pre-anesthetic interview was found to increase knowledge measured by an information recall test.[30]
Interestingly, the addition of the videotape had no effect on patients’ anxiety levels. The aforementioned study also evaluated the amount of time spent when counseling anesthesia patients by interview alone, video then interview, and interview then video. Duration of the encounter was the longest when the videotape was presented to the patient prior to the interview. In explaining this finding, it was felt that the video triggered more questions for the patient to ask his or her physician.[30]
The ability to use culturally sensitive approaches is especially unique to videotaped education. The appropriate use of actors, language, and specific messages tailors a video to a certain patient population and has been theorized to help educate patients with varying cultural backgrounds.[8] Cowan et al[31] demonstrated this when they evaluated patients’ educational responses to five-minute Spanish and English videotapes concerning the risks and benefits of intravenous (IV) contrast administration for computed tomography (CT) scans. It was found that when compared to a typical interview, patient knowledge and satisfaction increased with the addition of a videotape. Furthermore, the proportional increase in knowledge retention with the videotape in Spanish-speaking patients was greater than the increase in English-speaking patients. From this study, it can be proposed that videotapes sensitive to one’s language and culture may be especially effective educational methods for patients whose primary language is not English.[31]
Videotape is an effective and unique communication method that has value in a number of clinical settings. It may be especially useful in dermatology because of the visual effects it provides and its ability to increase recall. Furthermore, the ability to tailor videos to certain groups of people enhances the effectiveness of videotapes when language or cultural barriers exist. The consequences of patient education through videotapes are those of nonadherence and cost of production depending on the complexity of the video. One important finding is the proposal that video prior to interview may increase the number of questions a patient has for the physician.[30] While this may take more time on the dermatologist’s part, it also signifies more effective education. It implies the patient is more actively engaged in his/her healthcare, which is the ultimate goal of patient education in dermatology.
Office-based, computer-assisted patient education. Like videotapes, computer-assisted patient education can eliminate language and literacy challenges while also minimizing the amount of time spent by physicians. Additionally, patients are able to work through computer modules at self-moderated paces.[6,32] The ability to use graphics and audio makes the computer a good choice for patient education. Computer-assisted instruction was used to demonstrate metered dose inhaler technique for asthmatics and resulted in better techniques.[33] Bader and Strickman-Stein[25] studied five forms of education for cancer patients, evaluating them by pretest and posttest. Although small, the study evaluated text in the form of a paperback book, the same text online in HTML format, audio alone, audio with text on a webpage, and flash multimedia with animations and audio and text. Surprisingly, each mode of communication yielded a similar increase in test score. Users did prefer the multimedia format, and the least preferred was audio. Long-term recall was not evaluated, and it is possible that certain strategies would be more effective in establishing long-term memory.[25]
Videogames and interactive computer games have also been used as educational strategies to encourage patients to self manage their diseases. In a randomized, controlled trial by Homer et al,[34] an interactive computer program for children with asthma was used to teach allergen identification, medication use, and typical management in the setting of a normal day. Control groups received printed pamphlets outlining the same topics. Both groups demonstrated increased knowledge and satisfaction and decreased severity of asthma, but other than a small improvement in knowledge, the multimedia computer program did not seem to offer any significant advantage in the time evaluated.[34] A similar randomized, controlled trial by Kato et al[35] evaluated the use of a videogame to enhance education and adherence to cancer medications in adolescents and young adults. Adherence to medications, knowledge, and self efficacy were measured to be higher in the intervention group.[35]
Adding a modern spin to videotapes, computer-assisted patient education has the advantage of being interactive while preserving physicians’ time. The studies mentioned demonstrate that interactive media may help patients change behaviors and establish chronic treatment regimens. This interactive approach may be especially important in dermatology patients in order to establish proper skin care, allergen avoidance, and other treatment principles. Treatment regimens often become complex and difficult to integrate in daily life, and being able to practice within a computer game may improve adherence. Whether or not computer-assisted education actually improves recall of information is controversial. It is important to note that these methods of education may be age or population dependent. Using computer-assisted education in individuals not experienced with computers may actually increase anxiety and inhibit education.
Internet. The internet is a relatively new and extremely broad source of information for patients. It is important for physicians to realize that patients are using the internet extensively for information because the content is unregulated and extremely variable.[3]
Many websites are driven by marketing and not evaluated for accuracy. In 1999, Hu et al[36] evaluated internet sites that came up when searching for 10 skin conditions. They found that for most skin diseases, possible treatments and product information came up more often than educational information. Since it is difficult to determine accuracy of websites, this predominance of product information contributes to patients receiving incorrect or biased education.[36]
While the aforementioned study demonstrates the inherent risk in an information source as broad and variable as the internet, there are also advantages. The Contact Allergen Replacement Database (CARD) is one example. Developed by the Mayo Clinic and available online, it allows dermatologists to input allergens and develop lists of products free of those allergens and all cross-reactants. For patients with allergic contact dermatitis, it prevents them from having to read through ingredient lists to search for long chemical names and all cross-reactants. Additionally, it is thought to decrease the amount of time spent by physicians in addressing contact dermatitis.[37] Although small, a study was conducted by Kist et al[38] to evaluate the effectiveness of CARD in clinical outcomes. One group of patients received a CARD-produced list and the other received the typical information regarding what chemicals to avoid. The CARD group seemed to demonstrate greater improvements overall, but results were not statistically significant. All patients in the control group; however, stated that the CARD-generated list would have been helpful.[38]
When monitored appropriately, the internet can be a wealth of information for both patients and physicians. Databases such as CARD may save time for dermatologists and make the lives of their patients simpler. Recall of information can be made easier for patients, and having a list of products to avoid may decrease anxiety. At the same time, it is important for dermatologists to be aware of the inaccuracies and extensive dermatological product information posted freely on the internet. Cultural and language barriers may still challenge effective education through the internet, and the wealth of information may contribute to information overload. Perhaps the misinformation inherently present on the internet provides more motivation for dermatologists to spend time with their patients highlighting true, evidence-based information. Additionally, since it is well known that patients will search the internet, it may be advantageous to provide patients with reliable websites to visit rather than leaving them on their own to search the web.
Conclusion
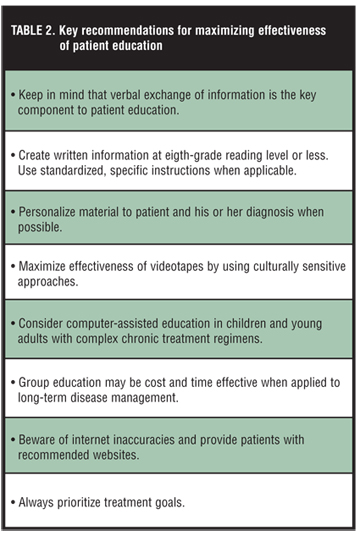
Patient education lies at the core of clinical dermatology. As a result, understanding the most effective modes of communicating with patients becomes extremely important. Each strategy of patient education has its own benefits and consequences, which have been summarized in Table 1. Because one strategy does not consistently emerge as the most effective way to communicate with patients, a variety of educational methods should be used to increase repetition and maximize individual learning. In doing so; however, one must keep in mind conflicting sources of information and the potential for information overload. Key recommendations are listed in Table 2. Ultimately, patient education is an interworking of effective education strategies, physician time, and patient motivation. Successful management of dermatological conditions is largely dependent on patient education, so understanding the process of education and putting forth the effort to educate patients effectively can produce long-lasting benefits on patient care.
{kind=link}
References
1. Dent, T. Part I. Patient education. Dis Mon. 2000;46(12):785–797.
2. Davis RH. Overcoming barriers in irritable bowel syndrome with constipation. J Fam Pract. 2009;58:S3–S7.
3. Cabana MD, Le TT. Challenges in asthma patient education. J Allergy Clin Immunol. 2005; 115(6):1225–1227.
4. Hill J, Bird H, Johnson S. Effect of patient education on adherence to drug treatment for rheumatoid arthritis: a randomized controlled trial. Ann Rheum Dis. 2001;60(9): 869–875.
5. Krakowski AC, Eichenfield LF, Dohil MA. Management of atopic dermatitis in the pediatric population. Pediatrics. 2008;122(4):812–824.
6. Glascoe FP, Oberklaid F, Dworkin PH, Trimm F. Brief approaches to educating patients and parents in primary care. Pediatrics. 1998;101(6):E10.
7. Kongsted A, Qerama E, Kasch H, et al. Education of patients after a whiplash injury: is oral advice any better than a pamphlet? Spine. 2008;33(22):E843–E848.
8. Vanderberg-Dent, S. Part II. Challenges in educating patients. Dis Mon. 2000;46(12):798–810.
9. Trevena LJ, Davey HM, Barratt A, et al. A systematic review on communicating with patients about evidence. J Eval Clin Pract. 2006;12(1):13–23.
10. Isaacman DJ, Purvis K, Gyuro J, et al. Standardized instructions: do they improve communication of discharge information from the emergency department? Pediatrics. 1992;89(6 Pt 2):1204–1208.
11. Arnold J, Goodacre S, Bath P, Price J. Information sheets for patients with acute chest pain: randomised controlled trial. BMJ. 2009;338:b541.
12. Ewan PW, Clark AT. Long-term prospective observational study of patients with peanut and nut allergy after participation in a management plan. Lancet. 2001; 357(9250):111–115.
13. Gold DT, McClung B. Approaches to patient education: emphasizing the long-term value of compliance and persistence. Am J Med. 2006;119(4 Suppl 1):32S-37S.
14. Skinner CS, Campbell MK, Rimer BK, et al. How effective is tailored print communication? Ann Behav Med. 1999;21(4):290–298.
15. Skinner CS, Strecher VJ, Hospers H. Physicians’ recommendations for mammography: do tailored messages make a difference? Am J Public Health. 1994;84(1):43–49.
16. Tschopp JM, Frey JG, Janssens JP, et al. Asthma outpatient education by multiple implementation strategy. Outcome of a programme using a personal notebook. Respir Med. 2005;99(3):355–362.
17. Wilson FL, Williams BN. Assessing the readability of skin care and pressure ulcer patient education materials. J WOCN. 2003;30(4):224–230.
18. Aldridge MD. Writing and designing readable patient education materials. Nephrol Nurs J. 2004;31(4):373–377.
19. Davis TC, Bocchini JA, Fredrickson D, et al. Patient comprehension of polio vaccine information pamphlets. Pediatrics. 1996;97(6 Pt 1):804–810.
20. Dimou C. Part III. Patient compliance. Dis Mon. 2000;46(12):811–822.
21. Morrow DG, Leirer VO, Andrassy JM, et al. The influence of list format and category headers on age differences in understanding medication instructions. Exp Aging Res. 1998;24(3):231–256.
22. Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalizations: a randomized trial. Med Care. 1999;37(1):5–14.
23. Hammond A, Bryan J, Hardy A. Effects of a modular behavioural arthritis education programme: a pragmatic parallel-group randomized controlled trial. Rheumatology (Oxford). 2008;47(11):1712–1718.
24. Schaffer S, Tian L. Promoting adherence: effects of theory-based asthma education. Clin Nurs Res. 2004;13(1):69–89.
25. Bader JL, Strickman-Stein N. Evaluation of new multimedia formats for cancer communications. J Med Internet Res. 2003;5(3):E16.
26. Bruera E, Pituskin E, Calder K, et al. The addition of an audiocassette recording of a consultation to written recommendations for patients with advanced cancer: A randomized, controlled trial. Cancer. 1999;86(11): 2420–2425.
27. Koh TH, Butow P, Coory M, et al. Provision of taped conversations with neonatologists to mothers of babies in intensive care: randomised controlled trial. BMJ. 2007;334(7583):28–31.
28. Volk RJ, Cass AR, Spann SJ. A randomized controlled trial of shared decision making for prostate cancer screening. Arch Fam Med. 1999;8(4):333–340.
29. Volk RJ, Spann SJ, Cass AR, Hawley ST. Patient education for informed decision making about prostate cancer screening: a randomized controlled trial with 1-year follow-up. Ann Fam Med. 2003;1(1):22–28.
30. Salzwedel C, Petersen C, Blanc I, et al. The effect of detailed, video-assisted anesthesia risk education on patient anxiety and the duration of the preanesthetic interview: A randomized controlled trial. Anesth Analg. 2008;106(1):202–209.
31. Cowan EA, Calderon Y, Gennis P, et al. Spanish and English video-assisted informed consent for intravenous contrast administration in the emergency department: a randomized controlled trial. Ann Emerg Med. 2007;49(2):221–230.
32. Wofford JL, Smith ED, Miller D. The multimedia computer for office-based patient education: a systematic review. Patient Educ and Couns. 2005;59(2):148–157.
33. Savage I, Goodyer L. Providing information on metered dose inhaler technique: is multimedia as effective as print? Fam Pract. 2003;20(5):552–557.
34. Homer C, Susskind O, Alpert HR, et al. An evaluation of an innovative multimedia educational software program for asthma management: report of a randomized, controlled trial. Pediatrics. 2000;106(1 Pt 2):210–215.
35. Kato PM, Cole SW, Bradlyn AS, Pollock BH. A video game improves behavioral outcomes in adolescents and young adults with cancer: a randomized trial. Pediatrics. 2008;122(2):E305–E317.
36. Hu W, Siegried EC, Siegel DM. Product-related emphasis of skin disease information online. Arch Dermatol. 2002;138(6):775–780.
37. el-Azhary RA, Yiannias JA. A new patient education approach in contact allergic dermatitis: the contact allergen replacement database (CARD). Int J Dermatol. 2004;43(4):278–280.
38. Kist JM, el-Azhary RA, Hentz JG, Yiannias JA. The contact allergen replacement database and treatment of allergic contact dermatitis. Arch Dermatol. 2004;140(12): 1448–1450.