James J. Leyden, MD, University of Pennsylvania Medical School, Philadelphia, Pennsylvania; James Q. Del Rosso, DO, Valley Hospital Medical Center, Las Vegas, Nevada
Disclosure: Drs. Leyden and Del Rosso are consultants for Medicis. Dr. Del Rosso is also a consultant, speaker, and/or researcher for Allergan, Coria, Galderma, Graceway, Intendis, Leo Pharma, Onset Therapeutics, Ortho Dermatology, PharmaDerm, Promius, Quinnova, Ranbaxy, SkinMedica, Stiefel, Triax, Unilever, and Warner Chilcott. This article was supported by Medicis, The Dermatology Company, Scottsdale, Arizona.
Abstract
Objective: To review data on pharmacokinetic factors that influence the absorption and tissue distribution for individual antibiotic agents to better inform clinicians on rational dosing considerations of oral antibiotics for the treatment of acne vulgaris. The focus is placed on the most commonly prescribed oral antibiotics for acne vulgaris, the tetracyclines. Dose-response is also reviewed. Design and methods: This review describes factors affecting the absorption, distribution, and target tissue penetration of the most frequently prescribed oral antibiotics for the treatment of acne vulgaris, the tetracyclines. Articles cited were identified by a search of PubMed covering the period from January 1, 2000, to November 15, 2010. Reference lists in articles identified in this search were searched manually for additional references of interest. Results: Pharmacokinetic factors that may influence outcomes in antibiotic therapy for acne vulgaris include drug solubility, gastrointestinal permeability, systemic absorption, tissue distribution, and target tissue penetration. In particular, drugs that are highly soluble and highly permeable are well absorbed and widely distributed. Drugs that are more lipophilic are believed to penetrate better into the lipid-rich sebaceous follicular tissues, where the therapeutic target, Propionibacterium acnes, resides. Food intake and differences in patient body weight can also alter antibiotic absorption and distribution, potentially resulting in differences in efficacy and tolerability. Dose-response data with oral antibiotics, including the tetracyclines, is scant. Pharmacokinetic studies completed with extended-release minocycline have allowed for assessment of interindividual differences in drug absorption, a consideration that may influence therapeutic response and/or predilection for adverse effects. Dose-response pharmacokinetic data is not currently available with other tetracyclines. Conclusion: An understanding of the differences in absorption (with and without meals or other ingestants), distribution, and target tissue penetration among oral tetracyclines is valuable for clinicians, as such factors may influence outcomes in patients treated for acne vulgaris. (J Clin Aesthet Dermatol. 2011;4(2):40–47.)
Oral antibiotics are recommended for the treatment of moderate or severe inflammatory acne.[1,2] These agents are frequently administered in combination with a topical acne regimen that may include a benzoyl peroxide–containing formulation to enhance therapeutic benefit and minimize the emergence of resistant strains of Propionibacterium acnes. A topical retinoid is commonly also incorporated, allowing for reduction in comedonal and inflammatory lesions via different mechanisms of action.[3]
The most commonly used oral antibiotics include the tetracyclines (tetracycline, doxycycline, minocycline); the macrolides (erythromycin and azithromycin)[4]; and trimethoprim/sulfamethoxazole (TMP/SMZ), a combination sulfonamide.[5] These agents work primarily through antibacterial effects against the proliferation of P. acnes within the sebaceous follicle.[6–8] Some agents, such as tetracyclines, may also have anti-inflammatory effects independent of their antibiotic activity.[9,10] P. acnes promotes an inflammatory cascade through multiple mechanisms, leading primarily to the development of inflammatory lesions and secondarily contributing to the formation of comedonal lesions.
Among the tetracyclines, doxycycline and minocycline are used most frequently in the United States and many other countries because of greater efficacy and lower prevalence of P. acnes resistance compared with tetracycline.[5] The macrolide erythromycin was used frequently in the past but is used less frequently now because of markedly decreased sensitivity of P. acnes to this agent. Use of TMP/SMZ is generally limited owing to concerns related to severe cutaneous drug reactions and hematological adverse events (AEs) and in an effort to conserve its use for the treatment of infections due to highly resistant pathogens, such as methicillin-resistant Staphylococcus aureus.[4]
Clinical use of oral antibiotics for acne is based primarily on empiric evidence. Clinical dose-response trial data and comparative efficacy trials are generally lacking.[11,12] In particular, trials to evaluate dose response in patients with acne are conspicuously rare,[11] but have been conducted with extended-release minocycline.[13,14]
Pharmacokinetic factors can influence the effectiveness of any systemic agent. The Biopharmaceutics Classification System is a helpful tool for predicting clinical pharmacokinetics of a drug based on its in-vitro aqueous solubility and in-vivo “permeability” (degree of oral absorption compared with intravenous absorption). Gastrointestinal (GI) absorption of a drug may be affected by food intake (particularly foods containing fat or minerals such as iron or calcium), by interpatient variability, and by specific drug attributes, such as drug solubility and permeability.[15,16]
Drug solubility and permeability influence absorption.[17,18] Generally, high solubility facilitates absorption of a drug, and low-solubility drugs, such as isotretinoin and cyclosporine, require the presence of a fatty meal because lipids solubilize the drug.[19] High permeability facilitates penetration of enterocytes for absorption but also facilitates access to hepatocytes and, consequently, to metabolizing enzymes. However, some agents with high permeability penetrate hepatocytes, but do not gain access to metabolizing enzymes; rather, they are excreted unchanged in bile. Other drugs with high permeability are rapidly metabolized and eliminated, leading to reduced distribution and target penetration.[19] In the antibiotic treatment of acne, target penetration refers to the ability of a drug to access the sebaceous follicles where excessive proliferation of P. acnes occurs in acne patients.[20] Lipophilic drugs have an advantage in penetrating these lipid-rich targets.
Given the range of factors that may potentially influence response, an understanding of the dose-response relationship with antibiotics is important for acne drugs, as it is for any medication. Inadequate or excessive dosing by the prescriber and patient can cause poor or unusually high GI absorption, leading to poor efficacy or an increased frequency of adverse events.[14,21] Inadequate dosing and/or prolonged exposure to antibiotics may encourage the development of antibiotic-resistant bacteria.[22,23] For example, exposure of P. acnes bacteria to sublethal doses of clindamycin and erythromycin has been shown to select for antibiotic-resistant bacterial strains in vitro.[24] Drug exposure may also be affected by body weight; research has shown that serum concentrations of minocycline decrease as body weight increases.[25]
This article reviews the factors that affect the absorption, distribution, and target penetration of systemic antibiotics prescribed for acne, as well as individual patient factors that contribute to their effectiveness, tolerability, and safety. The review focuses on the tetracyclines because they are the most commonly prescribed oral antibiotics for acne.[5]
Search Methodology
A PubMed search covering the period from January 1, 2000, to November 15, 2010, was conducted using the following search string: (acne OR “acne vulgaris”) AND (antibiotics OR tetracycline OR doxycycline OR minocycline OR macrolide OR azithromycin OR erythromycin OR clindamycin). Reference lists in articles identified in this search and in treatment guidelines were searched manually for additional references of interest.
Factors Contributing to Efficacy
To be effective, an oral medication must be absorbed, be distributed by circulation, and penetrate the target tissue. Absorption, distribution, and target penetration are influenced by the solubility and permeability of a drug and by inherent characteristics of the target site. Specifically, drug absorption is facilitated by high aqueous solubility and high GI permeability.[17,18] A drug is considered highly soluble if its highest dose dissolves in 250mL of aqueous solution across a pH range of 1 to 7.5 at a temperature of 37°C.[17,18] A drug is considered highly permeable if it is 90-percent absorbed when taken orally compared with an equal dose administered intravenously. Molecular weight is also an important factor affecting drug absorption, with lower-molecular-weight drugs being more easily absorbed.[26]
Food is most likely to adversely influence the absorption of a drug if the agent has both low solubility and permeability.[18] Several specific food components may interfere with drug solubility by forming complexes with the drug (e.g., iron, calcium, and other minerals), absorbing the drug (e.g., fiber, pectins), or changing GI pH levels. Food components may interfere with drug permeability by competing for enterocyte transporters or affecting motility, but dietary fat may improve the absorption of drugs with poor solubility and high permeability.[18] With highly soluble/highly permeable drugs, drug transporters are not as essential to absorption.[17] Nonetheless, a high-fat meal may reduce peak absorption time by delaying stomach emptying.[19] It is important to understand that rapid absorption may not only increase therapeutic drug effects, but may also induce or exacerbate AEs, especially if the AE is precipitated by a rapid rise in serum concentrations or a high-peak concentration.[27]
Absorption and subsequent distribution of a drug is also facilitated by the combination of high solubility and high permeability.[19] Drugs with high GI permeability are also highly permeable to hepatocytes, which contain a variety of metabolic enzymes that can deactivate, activate, and/or promote elimination of some drugs.[19] Penetration of the lipid-rich sebaceous follicles that make up the target tissues in the treatment of acne is facilitated by high lipophilicity, which is a common characteristic of highly permeable drugs.[27,28]
High permeability can also facilitate penetration of the blood-brain barrier, which may lead to central nervous system AEs, such as headache or vertigo.[27] Thus, an effective antibiotic would pass easily through the gastric and/or intestinal mucosa and be lipophilic enough to be well distributed to sebaceous follicles.[27] Drugs with a higher lipophilic/hydrophilic partition coefficient (measured as the ratio of octanol/water concentration) leave the aqueous spaces more rapidly and enter the lipid-rich target tissues.[29]
Tetracycline
Tetracycline (molecular weight, 444)[30] has high solubility, but relatively poor permeability,[19] resulting in 77 to 88-percent absorption of the oral medication compared with intravenous administration (Table 1).[31] Food reduces the absorption of tetracycline by about 50 percent.[32,33] Dietary iron, calcium, magnesium, and aluminum chelate tetracycline in the GI tract, thus reducing its absorption.[34] Tetracycline has a large volume of distribution (108L), but is not highly lipophilic and therefore may not optimally penetrate the follicular unit, which contains large amounts of lipid-rich sebum.[15]
{kind=link}
Doxycycline
Doxycycline (molecular weight, 462)[30] exhibits greater solubility, permeability, and lipophilicity compared with tetracycline,19 and as a result is less affected by dietary components (Table 1). Food reduces absorption of doxycycline by approximately 20 percent,[33] and iron, calcium, magnesium, and aluminum may also reduce its absorption through chelation.[27]
Despite its higher permeability, doxycycline is less extensively metabolized than tetracycline,[19] with 29 to 55 percent of the administered doxycycline dose being excreted in bile and urine as unchanged drug.[27] Doxycycline also has a lower volume of distribution than tetracycline (50–80L).[15] Although more lipophilic than tetracycline,[35] concentrations of doxycycline in serum are about fivefold higher than in soft tissues.[36]
Minocycline
Minocycline (molecular weight, 457)[30] is highly soluble, highly permeable, very lipophilic, and extensively metabolized (Table 1).[19] High solubility and permeability minimize the effects of food on absorption.[17,37] In a study of minocycline immediate release (IR) under fed and fasted conditions, mean area under the curve (AUC) was 2.2mg/h/L with food and 2.11mg/h/L fasted. Mean maximum observed plasma concentration (Cmax) and time to Cmax (tmax) were each 0.65mg/L at 120 minutes. In a second study, food, milk, and iron reduced absorption of minocycline by 13, 27, and 77 percent, respectively.[32] As with tetracycline and doxycycline, antacids with calcium or magnesium reduce minocycline absorption,[15] and aluminum reportedly also reduces absorption.[38]
The volume of distribution with minocycline is higher (80–115L) than with doxycycline,[15] and minocycline is tenfold more lipophilic than tetracycline and fivefold more lipophilic than doxycycline.[35] In contrast to tetracycline and doxycycline, minocycline concentrations in skin are 47-percent higher than in serum because minocycline rapidly mobilizes from the blood into tissues, including lipid-rich sites.[39]
Lipophilicity is believed to enhance the access of minocycline into the target sebaceous follicles via penetration into sebaceous glands.[29] However, lipophilicity also enables minocycline to easily cross the blood-brain barrier, potentially leading to acute vestibular AEs, especially with IR minocycline formulations with rapid access to the systemic circulation.[13] The extended-release (ER) formulation of minocycline causes absorption and distribution to occur more slowly with a lower Cmax and a lower cumulative drug exposure over a given time period (i.e., AUC).[5] This slowing of absorption and distribution may result in a reduction in acute vestibular AEs without a reduction in efficacy.[5,13]
Impact of Absorption on Treatment Outcomes
Doxycycline and minocycline are low-molecular-weight[30] and highly soluble and permeable drugs,[19] with minocycline exhibiting greater permeability due to greater lipophilicity.[29] Tetracycline is also a low-molecular-weight drug,[30] but is far less permeable,[19] which is why food inhibits tetracycline to a greater extent than it does doxycycline (22%) or minocycline (12%).[28]
These pharmacokinetic differences between tetracycline, doxycycline, and minocycline have the potential to influence their relative effectiveness and tolerability. In a nine-week, parallel-group, comparative trial, 60 adult acne patients with P. acnes counts ?10,000 colony-forming units/cm2 received minocycline IR 200mg/d, doxycycline 200mg/d, or tetracycline 1,000mg/d for six weeks.[28]
P. acnes counts were measured at baseline, after six weeks, and for three additional weeks after treatment was discontinued. Minocycline IR 200mg was associated with a tenfold greater reduction in P. acnes levels at Week 6 compared with doxycycline or tetracycline. After treatment discontinuation (Week 9), P. acnes levels remained lower in patients treated with minocycline IR than in those treated with either doxycycline or tetracycline.
Minocycline treatment may have an advantage compared with tetracycline or doxycycline because enhanced tissue penetration may be accompanied by a lower incidence of emergence of resistant P. acnes strains.[5] In an in-vitro analysis of 73 P. acnes strains, resistance (minimum inhibitory concentration [MIC] ?5µg/mL) to erythromycin alone was detected in 35 strains, resistance (MIC ?2µg/mL) to tetracycline alone in 15 strains, and resistance to both tetracycline and erythromycin in 15 strains.[40] Minocycline was active against all strains, exhibiting a lower MIC than either tetracycline or doxycycline.[40]
On the other hand, minocycline IR formulations have been associated overall with a somewhat higher incidence of AEs compared with doxycycline. In a 2005 systematic review of clinical trials,[21] AEs were reported in 0 to 61 percent of patients treated with doxycycline and 11.7 to 83.3 percent of patients treated with minocycline (only the IR formulation was available at that time). With doxycycline, GI AEs (4–51.7%) were the most frequent AEs, followed by skin reactions (range: 0.42–30.5%). The most frequent published case reports on doxycycline relate to esophageal erosion, an AE that typically is not reported with either IR or ER formulations of minocycline.
With minocycline IR, central nervous system reactions were the most frequent AEs (<3–67%), followed by GI events. Discontinuations due to acute vestibular AEs were reported in 1.7 to 8.8 percent of patients. The most frequent published case reports of AEs associated with minocycline IR have included hyperpigmentation, drug hypersensitivity, and autoimmune effects.[21]
Although pharmacokinetic variables suggest differences in efficacy, tolerability, and food effects among tetracyclines, few studies have compared the efficacy of individual tetracyclines head to head, and there have been no dose-response studies examining the association between pharmacokinetic variables and outcomes with oral antibiotics used to treat acne other than ER minocycline.[11] Dose-response studies performed during the development of minocycline ER illustrate ways in which pharmaco-kinetic variables can impact treatment outcomes, optimize efficacy, and reduce the occurrence of AEs. These studies evaluated the effects of drug dissolution rate and body weight on efficacy, tolerability, and food effects.
Dose-Response Studies
Extended release versus immediate release. Clinical and pharmacokinetic data with multiple formulations of minocycline IR indicate that the occurrence of vestibular AEs correlates with the dissolution rate and Cmax of minocycline.[27] Additional data suggest that vestibular AEs are more frequent in patients with lower body weight unless the dose is adjusted to body weight.[25] The occurrence of vestibular AEs appeared to be related to a rapid influx of minocycline into the blood, which produces high spikes in serum concentrations following administration of minocycline IR.[27] These spikes likely facilitate penetration of the blood-brain barrier, potentially increasing the risk of vestibular AEs. The ER formulation of minocycline slows the rate of drug release and systemic drug exposure. A weight-based dosing schedule was developed to minimize the impact of differences in body weight on treatment outcomes and AEs.
Rate of dissolution. In a randomized, multiple-dose, crossover trial,[29] 28 healthy adults received minocycline ER 135mg or minocycline IR 100mg once daily for six days, before undergoing 14-day washout and switching to the alternative treatment. Blood assays for determination of pharmacokinetic parameters were assessed before and for 72 hours after the final dose. Twenty-seven subjects completed the study. Minocycline ER Cmax occurred later (3.5–4h) than minocycline IR Cmax (2.25–3h). At steady state, minocycline ER Cmax was lower than minocycline IR Cmax (2.63µg/mL vs. 2.92µg/mL, respectively). The mean minocycline ER AUC from 0 to 24 hours was lower than that of minocycline IR (33.32µg•h/mL and 46.35µg•h/mL, respectively).
Although the sample size for this study was small, the results nonetheless provide useful information about the mean and median values for a population, but are of limited utility for characterizing individual patient variability within a population. Interpatient variability can account for differences in individual response to an antibiotic compared with the anticipated response for the majority of the population. As the classic S curve of dose response predicts, a patient who absorbs the drug poorly may experience poor efficacy at a dose that is otherwise effective for the median of a population; whereas, a patient who absorbs the drug with unusual rapidity may experience AEs at a dose that is otherwise well tolerated by the median of a population.
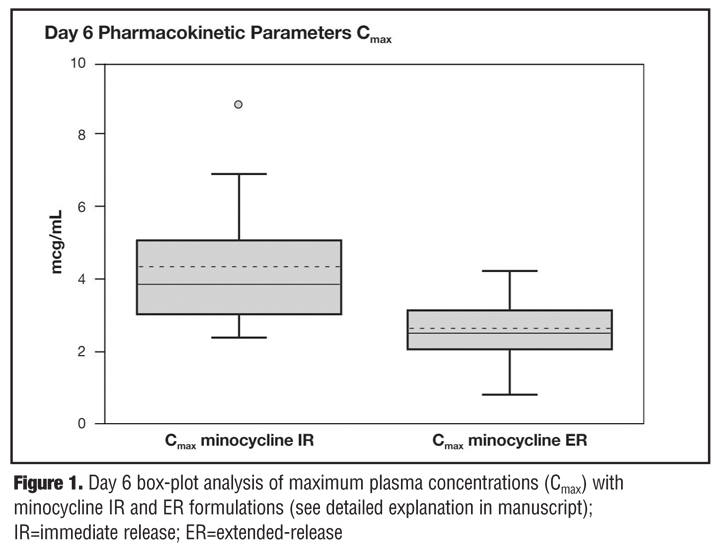
Important differences between minocycline ER and IR with respect to AUC and Cmax can be displayed to great effect using a box-plot analysis, wherein the upper border of the box represents the value of a pharmacokinetic parameter for the 75th percentile, the lower edge the 25th percentile, and the midline of the box the median of a population. The resulting box gives the range for 75 percent of the study population. The bars above and below the box represent the highest and lowest values not more than 1.5 times the range within the box. Outliers include patients with pharmacokinetic values greater than 1.5-fold above or below the upper or lower limit of the intrabox range but less than threefold times that distance. Extreme outliers have values threefold above or below the range within the box plot.
Figure 1 is a box-plot display of the Cmax data for the two minocycline formulations derived from the 28-subject study described above.[41] The box for the ER formulation is smaller than that of IR formulation; 75 percent of subjects receiving minocycline ER have a Cmax between 2 and 3µg/mL compared with a broader range for subjects receiving the IR formulation. With the IR formulation, there was one (3.7%) extreme outlier with a Cmax of 8.9µg/mL. In addition, there were two subjects (7.4%) with values >6µg/mL with the IR formulation compared with two subjects (7.4%) with values >4µg/mL with the ER formulation. There were no extreme outliers following administration of minocycline ER. Spearman rank correlation (P<0.001) showed a significant degree of concordance in Cmax levels for the two formulations. For example, the extreme outliers who had the lowest and the highest Cmax with the IR formulation also had the lowest and the highest Cmax with the ER formulation.
{kind=link}
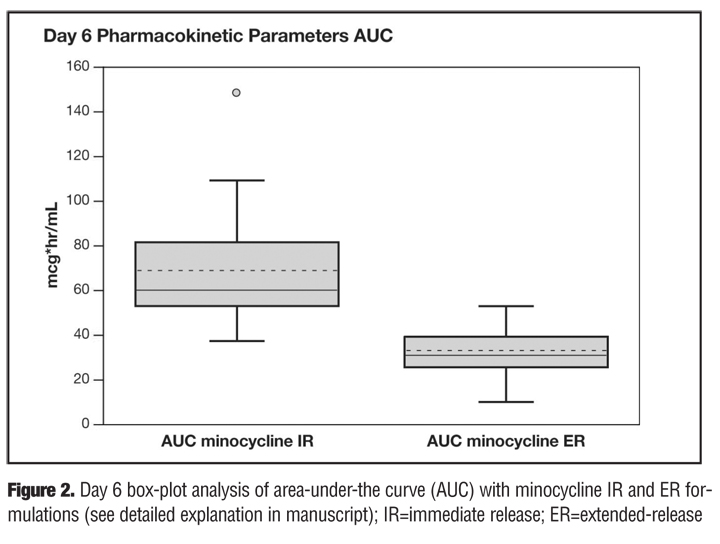
Figure 2 is a box-plot display of the steady-state AUC over a 24-hour period. ER minocycline showed a very small box compared with the IR formulation.[41] The IR formulation had one (3.7%) extreme outlier for high absorption; this subject was the same person who was also an extreme outlier for Cmax with the IR formulation and also had the second highest AUC with ER minocycline. The subject with the lowest AUC with minocycline IR also had the lowest AUC value with the ER formulation. The Spearman rank correlation was again significant (P<0.001), indicating a high degree of concordance between AUC and the ER and IR formulations.
{kind=link}
Collectively, these data suggest that patients receiving either minocycline formulation would be expected to derive therapeutic benefits from therapy but that patients treated with minocycline ER would be less likely to have extreme elevations in Cmax and AUC and therefore be more likely to better tolerate therapy. Only one subject had a low AUC following administration of minocycline ER. This subject might be predisposed to exhibit a poor clinical response with the ER formulation because of lower GI absorption. In cases with suboptimal response, assuming good compliance and an adequate treatment duration, an escalation of the daily minocycline ER dose may be required because the patient may be an innate “low minocycline absorber.”
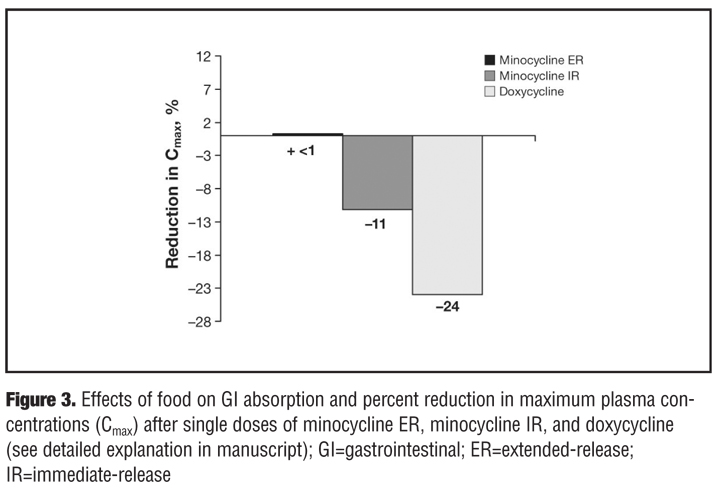
Effects of food. In a small randomized, single-dose crossover trial,[29] 24 healthy adults (12 women) aged ?18 years received consecutive single oral doses of minocycline ER 135mg under fasted conditions and after a meal that included dairy, separated by a seven-day washout period. The population included African-American (n=12), Caucasian (n=10), Hispanic (n=1), and Asian (n=1) subjects.[42]
The tmax for minocycline ER was 3.52 hours under fed conditions and 3.69 hours under fasted conditions. Cmax was 1.85µg/mL under fed conditions and 1.84µg/mL under fasted conditions. These data suggest that food intake has little effect on the absorption of minocycline ER (<1% decrease in absorption under fed conditions) (Figure 3). In contrast, there was an 11-percent reduction in minocycline IR absorption and a 24-percent reduction in doxycycline absorption after a meal. The AUC of minocycline ER was 38.4µg/mL•h under fed conditions and 39.1µg/mL•h under fasted conditions. Terminal half-lives under fed and fasted conditions were 16.6 and 16.3 hours, respectively, for minocycline ER.[42]
{kind=link}
AEs included headache (n=5), dizziness (n=1), drowsiness (n=1), syncope (n=1), and lightheadedness (n=1) with minocycline ER. These results suggest that food has less impact on the absorption and tolerability of minocycline ER than on minocycline IR.
Weight-based dosing. In a small, blinded, crossover study, 32 female patients (aged 21–55 years) received minocycline ER or generic minocycline IR for four days before undergoing a 14-day washout and switching to the alternative treatment. Both minocycline formulations were administered on a weight-based schedule: 100mg/d, 50–69kg (n=20); 150mg/d, 70–89kg (n=7); and 200mg/d, ?90kg (n=5). Minocycline IR was released from its capsule more rapidly (90% within 45 min) than minocycline ER (30–53% in 1h, 54–84% in 2h, and >85% in 4h).[43]
There was no difference between the two minocycline formulations with respect to general AEs (e.g., headache, malaise) or GI AEs. However, vestibular AEs (e.g., vertigo, dizziness, blurred vision) were significantly less frequent with ER minocycline (P=0.0003). In all, five vestibular AEs were reported with minocycline ER and 27 were reported with minocycline IR.[43]
In a Phase II dose-ranging study,[14] 233 patients aged 12 to 30 years with acne vulgaris were randomized to receive minocycline ER tablets 1, 2, or 3mg/kg or placebo once daily for 12 weeks. The efficacy of minocycline ER was positive across all of the weight-based dosing groups. Percentage reductions in inflammatory lesions were 56.8 percent in the 1mg/kg group, 49.3 percent in the 2mg/kg group, and 46.6 percent in the 3mg/kg group. The difference between minocycline ER 1mg/kg and placebo was significant at Week 12 (P=0.015 vs. placebo). The overall occurrence of any AE was similar in patients in the 1mg/kg group (53%) and 2mg/kg (56%) groups and slightly higher in the 3mg/kg group (65%). The incidence of acute vestibular AEs increased with dose from 10.2 percent in the 1mg/kg group to 16.4 percent in the placebo group, 23.7 percent in the 2mg/kg group, and 28.3 percent in the 3mg/kg group. AEs leading to treatment discontinuation were reported less frequently in the 1mg/kg group (n=4) than in the 2mg/kg (n=7) or 3mg/kg groups (n=14). These results indicated that efficacy, defined as reduction in inflammatory lesions, was similar across dosage ranges, but that use of a lower dose based on body weight resulted in fewer acute vestibular AEs.
A pooled analysis of patients treated with minocycline ER 1mg/kg as monotherapy in the aforementioned Phase II dose-ranging trial and in two Phase III trials was conducted to characterize efficacy and tolerability in a total of 1,038 patients with moderate-to-severe acne vulgaris. In these trials, 674 patients received minocycline ER 1mg/kg once daily and 364 received placebo.[13] Minocycline ER was administered in a 45mg dose to patients weighing 45 to 59.54kg, 90mg to patients weighing 60 to 90.45kg, and 135 mg to patients weighing 90 to 136.36kg.
Minocycline ER therapy resulted in a mean 45.5-percent reduction in inflammatory lesion counts compared with a 32.4-percent reduction in the placebo group (P<0.001). Evaluator’s Global Severity Assessment ratings indicated that 16.6-percent of patients in the minocycline ER group were “clear” or “almost clear,” compared with 8.7 percent in the placebo group. Noninflammatory lesion counts decreased by 14.9% and 6.3% in the minocycline ER and placebo groups, respectively.[13]
Adverse events were reported by similar percentages of the minocycline ER (56.2%) and placebo (54.1%) groups. Vestibular AEs generally occurred with similar frequency in patients treated with minocycline ER and placebo: nausea (9.5 vs. 11.3%, respectively), vomiting (2.1 vs. 2.5%), tinnitus (1.5 vs. 1.4%), and vertigo (1.2 vs. 0.8%). Urticaria occurred infrequently (1.5 vs. 0.3%).[13] Dizziness was reported with minocycline ER more frequently than with placebo (8.8 vs. 4.7%), but the incidence was generally lower than that reported with minocycline IR.[21] Collectively, these results support the hypothesis that an ER minocycline formulation administered using a weight-based dosing schedule can improve tolerability. The results also suggest that efficacy when treating acne may be maintained by using weight-based dosing of minocycline ER, likely due to its high lipophilicity.
Conclusion
Although there are many effective therapies available for the management of acne vulgaris, oral antibiotics differ in pharmacokinetic and pharmacodynamic characteristics that may influence their efficacy and AE profiles. To optimize antibiotic therapy in patients with acne, clinicians are encouraged to be aware of how the pharmacokinetics of individual agents can influence outcomes in individual patients.
Antibiotics differ in the extent to which they are absorbed, are distributed, and penetrate follicular tissues. Antibiotics with good absorption are less likely to be affected by concurrent administration with food. Metal cations ingested in meals, medication, or dietary supplements may reduce absorption of a given drug through chelation. Antibiotics that can be taken with food are less likely to cause GI AEs that can limit their utility and are more likely to promote adherence because patients do not need to consciously separate ingesting the medication from meals or snacks. Nonetheless, all currently available tetracyclines may have their GI absorption reduced by intake of aluminum, calcium, magnesium, and iron, although minocycline is affected primarily by iron.
Differences in the antibiotic formulation can markedly alter outcomes, particularly with respect to tolerability. Clinical and pharmacokinetic study data on minocycline IR and ER formulations suggest that rapid absorption increases the occurrence of acute vestibular AEs, whereas slower absorption improves tolerability. Accurate weight-based dosing of minocycline ER has been shown to maintain effectiveness in reducing inflammatory acne lesions while decreasing cumulative drug exposure and minimizing the risk of dose-related AEs.
Acknowledgments
Jeffrey Coleman, MA, and Robert Gatley, MD, of Complete Healthcare Communications, Chadds Ford, Pennsylvania, provided editorial support for this manuscript, with funding from Medicis, The Dermatology Company, Scottsdale, Arizona.
References
1. Dreno B, Bettoli V, Ochsendorf F, et al. European recommendations on the use of oral antibiotics for acne. Eur J Dermatol. 2004;14:391–399.
2. Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60:S1–S50.
3. Leyden JJ. Therapy for acne vulgaris. N Engl J Med. 1997;336:1156–1162.
4. Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49:S1–S37.
5. Del Rosso JQ, Kim G. Optimizing use of oral antibiotics in acne vulgaris. Dermatol Clin. 2009;27:33–42.
6. Jeremy AH, Holland DB, Roberts SG, et al. Inflammatory events are involved in acne lesion initiation. J Invest Dermatol. 2003;121:20–27.
7. Mouser PE, Baker BS, Seaton ED, Chu AC. Propionibacterium acnes-reactive T helper-1 cells in the skin of patients with acne vulgaris. J Invest Dermatol. 2003;121:1226–1228.
8. Webster GF. Acne vulgaris. BMJ. 2002;325:475–479.
9. Sapadin AN, Fleischmajer R. Tetracyclines: nonantibiotic properties and their clinical implications. J Am Acad Dermatol. 2006;54:258–265.
10. Webster G, Del Rosso JQ. Anti-inflammatory activity of tetracyclines. Dermatol Clin. 2007;25:133–135, v.
11. Ochsendorf F. Systemic antibiotic therapy of acne vulgaris. J Dtsch Dermatol Ges. 2006;4:828–841.
12. Garner SE, Eady EA, Popescu C, et al. Minocycline for acne vulgaris: efficacy and safety. Cochrane Database Syst Rev. 2003:CD002086.
13. Fleischer AB, Jr., Dinehart S, Stough D, Plott RT. Safety and efficacy of a new extended-release formulation of minocycline. Cutis. 2006;78:21–31.
14. Stewart DM, Torok HM, Weiss JS, Plott RT. Dose-ranging efficacy of new once-daily extended-release minocycline for acne vulgaris. Cutis. 2006;78:11–20.
15. Agwuh KN, MacGowan A. Pharmacokinetics and pharmacodynamics of the tetracyclines including glycylcyclines. J Antimicrob Chemother. 2006;58:256–265.
16. Oracea™ (doxycycline, USP). Full Prescribing Information, CollaGenex Pharmaceuticals, Inc., Newtown, PA, 2006.
17. Custodio JM, Wu CY, Benet LZ. Predicting drug disposition, absorption/elimination/transporter interplay and the role of food on drug absorption. Adv Drug Deliv Rev. 2008;60: 717–733.
18. Fleisher D, Li C, Zhou Y, et al. Drug, meal and formulation interactions influencing drug absorption after oral administration. Clinical implications. Clin Pharmacokinet. 1999;36:233–254.
19. Wu CY, Benet LZ. Predicting drug disposition via application of BCS: transport/absorption/ elimination interplay and development of a biopharmaceutics drug disposition classification system. Pharm Res. 2005;22:11–23.
20. Gollnick HP, Finlay AY, Shear N. Can we define acne as a chronic disease? If so, how and when? Am J Clin Dermatol. 2008;9:279–284.
21. Smith K, Leyden JJ. Safety of doxycycline and minocycline: a systematic review. Clin Ther. 2005;27:1329–1342.
22. Guillemot D, Carbon C, Balkau B, et al. Low dosage and long treatment duration of beta-lactam: risk factors for carriage of penicillin-resistant Streptococcus pneumoniae. JAMA. 1998;279:365–370.
23. Burgess DS. Pharmacodynamic principles of antimicrobial therapy in the prevention of resistance. Chest. 1999;115: 19S–23S.
24. Crawford WW, Crawford IP, Stoughton RB, Cornell RC. Laboratory induction and clinical occurrence of combined clindamycin and erythromycin resistance in Coryne-bacterium acnes. J Invest Dermatol. 1979;72:187–190.
25. Gump DW, Ashikaga T, Fink TJ, Radin AM. Side effects of minocycline: different dosage regimens. Antimicrob Agents Chemother. 1977;12:642–646.
26. Lennernas H. Intestinal permeability and its relevance for absorption and elimination. Xenobiotica. 2007;37:1015–1051.
27. Del Rosso J. Clinical significance of brand versus generic formulations: focus on oral minocycline. Cutis. 2006;77: 153–156.
28. Leyden JJ, Kaidbey K, Gans EH. The antimicrobial effects in vivo of minocycline, doxycycline and tetracycline in humans. J Dermatol Treat. 1996;7:223–225.
29. Plott RT, Wortzman MS. Key bioavailability features of a new extended-release formulation of minocycline hydrochloride tablets. Cutis. 2006;78:6–10.
30. O’Neil MJ, Smith A, Heckelman PE, Budavari S. The Merck Index: An Encyclopedia of Chemicals, Drugs, and Biologicals. 13th ed. Hoboken, NJ: John Wiley & Sons; 2001.
31. Fabre J, Milek E, Kalfopoulos P, Merier G. [Tetracycline kinetics in man. Digestive absorption and serum concentration]. Schweiz Med Wochenschr. 1971;101: 593–598.
32. Leyden JJ. Absorption of minocycline hydrochloride and tetracycline hydrochloride. Effect of food, milk, and iron. J Am Acad Dermatol. 1985;12:308–312.
33. Welling PG, Koch PA, Lau CC, Craig WA. Bioavailability of tetracycline and doxycycline in fasted and nonfasted subjects. Antimicrob Agents Chemother. 1977;11:462–469.
34. Neuvonen PJ. Interactions with the absorption of tetracyclines. Drugs. 1976;11:45–54.
35. Cunha BA, Garabedian-Ruffalo SM. Tetracyclines in urology: current concepts. Urology. 1990;36:548–556.
36. Gnarpe H, Dornbusch K, Hagg O. Doxycycline concentration levels in bone, soft tissue and serum after intravenous infusion of doxycycline. A clinical study. Scand J Infect Dis Suppl. 1976:54–57.
37. Smith C, Woods CG, Woods MJ. Absorption of minocycline. J Antimicrob Chemother. 1984;13:93.
38. Solodyn® [package insert]. Scottsdale, AZ: Medicis, The Dermatology Company; 2010.
39. Macdonald H, Kelly RG, Allen ES, et al. Pharmacokinetic studies on minocycline in man. Clin Pharmacol Ther. 1973;14:852–861.
40. Ross JI, Snelling AM, Eady EA, et al. Phenotypic and genotypic characterization of antibiotic-resistant Propionibacterium acnes isolated from acne patients attending dermatology clinics in Europe, the USA, Japan and Australia. Br J Dermatol. 2001;144:339–346.
41. Data on File (NDA 50-808; Section 2.7.6.4). Medicis Pharmaceutical Corporation, Scottsdale, AZ; 2006.
42. Data on File (NDA 50-808; Section 2.7.6.2; Study AAI-US-190). Medicis Pharmaceutical Corporation, Scottsdale, AZ; 2006.
43. Data on File (NDA 50-808; Section 3.2.P.8.3). Medicis Pharmaceutical Corporation, Scottsdale AZ; 2006