Khosro Sadeghani, MD; Joseph R. Kallini, MD; Amor Khachemoune, MD, FAAD, FACMS
Division of Dermatology, Department of Medicine, Facey Medical Center, Mission Hills, California;
Department of Dermatology, Saint Louis University, St. Louis, Missouri; Veterans Affairs Hospital, Brooklyn, New York
Abstract
The authors describe a 33-year-old man with human immunodeficiency virus who developed erythematous macules on the palms and soles with subsequent headaches, papilledema, and iritis. They review the salient characteristics of neurosyphilis with a focus on human immunodeficiency virus-positive individuals. The incidence of syphilis has increased since the year 2000 in African Americans, Hispanics, and men who have sex with men. Treponema pallidum is the causative agent of this disease—a fastidious, slowly growing, microaerophilic spirochete. Sexual contact is the most common mode of transmission. The rapid plasma reagin, Venereal Disease Research Laboratory assay, and fluorescent treponemal antibody absorption assay are commonly used to diagnose syphilis. The mainstay treatment is penicillin. Special considerations exist in the natural history and management of syphilis in the setting of human immunodeficiency virus. (J Clin Aesthet Dermatol. 2014;7(8):35–40.)
Syphilis in the setting of human immunodeficiency virus (HIV) infection can pose many unique problems. HIV-positive individuals are two to five times more likely to transfer syphilis to other contacts through open syphilitic sores. The cutaneous features of syphilis in HIV can be drastically different from the expected erythematous macules and papules on the palms and soles; some patients may even present with hypopigmented lesions. Also, due to the infectivity of syphilis in HIV-positive patients, the Centers for Disease Control and Prevention (CDC) recommends cerebrospinal fluid (CSF) analysis, regardless of the stage of syphilis, to evaluate for neurosyphilis.[1]
In this article, the authors present an HIV-positive patient with uncommon manifestations of syphilis, discuss the salient characteristics of this disease, and outline current treatment guidelines.
Case presentation
A 33-year-old man was referred to dermatology clinic for evaluation of a pruritic eruption on his palms and soles that started about 4 to 5 weeks earlier. The patient believes that the rash started a few days after initiating prednisone for management of ulcerative colitis. Two months ago, the patient noted a nonspecific eruption on the torso and lower extremities that completely resolved in less than two weeks. The patient also complains of a recent-onset headache. He denies fever, chills, and weight loss. The patient takes prednisone and mesalamine for management of ulcerative colitis. The patient is sexually active with multiple male partners and uses barrier protection occasionally. He denies a prior history of sexually transmitted diseases.
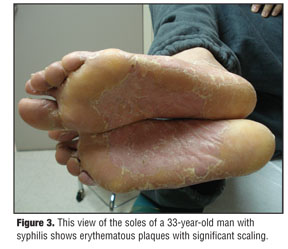
Skin examination revealed diffuse erythema with desquamative scaling on his dorsal hands (Figure 1), palms (Figure 2), and soles (Figure 3). Postinflammatory hyperpigmentation on the torso was also present, likely secondary to the eruption from two months prior. Differential diagnosis of the palmoplantar eruption included eczematous dermatitis, psoriasis, drug eruption, tinea manuum and tinea pedis with onychomycosis, and syphilis.
Skin biopsy of one scaly plaque showed psoriasiform dermatitis with parakeratosis and a perivascular lymphocytic infiltrate. Periodic acid-Schiff (PAS) staining was negative. However, rapid plasma reagin (RPR) was reactive. The fluorescent treponemal antibody–absorption (FTA-ABS) assay was positive, although spirochetal microorganism staining in the skin biopsy specimen was negative. HIV antibody was reactive.
The patient was referred to a neurologist and ophthalmologist for his headache. The ophthalmologist found bilateral papilledema and iritis. Lumbar puncture showed positive Venereal Disease Research Laboratory (VDRL) in the cerebrospinal fluid (CSF). A diagnosis of neurosyphilis was made. The patient was admitted to the hospital and a peripherally inserted central catheter (PICC) was placed. He was treated with 3 million units (MU) of intravenous (IV) penicillin G every four hours for a total of 14 days. Afterwards, the patient was given one dose of 2.[4]MU of intramuscular (IM) penicillin G benzathine and penicillin G procaine (bicillin). The palmar eruption improved dramatically.
{kind=link}
{kind=link}
{kind=link}
Discussion
Prior to the Second World War, syphilis was a ubiquitous illness and a leading cause of external genital ulceration. The incidence of syphilis declined significantly with the subsequent use of penicillin. The incidence of syphilis dramatically decreased in the 1970s and increased promptly again in the 1980s. Illegal drug use, particularly crack cocaine, appears to have played a major role in that resurgence.[2,3] In the developed world, the rate of syphilis declined rapidly with the widespread use of penicillin. In 2000, the incidence of syphilis reached its lowest since 1941 at 2.1 cases per 100,000.[4,5] The rates of syphilis have been increasing in the United States, England, Australia, and Europe, primarily among men who have sex with men.[6,7]
Although the incidence of syphilis in the United States declined 89.[7] percent during 1990 to 2000, the rate increased annually from 2001 to 2009, before decreasing once again in 2010. In 2001 to 2004, rates of primary and secondary syphilis began rising, particularly in African Americans, Hispanics, and men who have sex with men. The incidence of syphilis in African American and Hispanic individuals, as well as in homosexual men, is significantly higher than in other populations.[6] By 2004, the prevalence of syphilis among African Americans was 5.6 times higher than in Caucasians. Additionally, 64 percent of all cases reported in the United States were among men who have sex with men, with a rise from 3.0 cases per 100,000 people in 2001 to 7.9 in 2010.[5] Men who have sex with men constitute a high-risk group for the acquisition of syphilis and HIV.[8]
Treponema pallidum, the organism responsible for this disease, is a fastidious, microaerophilic spirochete that grows slowly both in vivo and in vitro (with a doubling time of greater than 30 hours). Sexual contact is the most common mode of acquiring syphilis. The sites of inoculation are usually the genital organs. Lips, tongue, and abraded areas of the skin have been described as well, although anecdotal reports cite kissing as the potential route in these cases. Healthcare providers and laboratory workers have apparently become infected with T. pallidum through accidental contact with infected secretions when appropriate protective gear (gloves) was not used.[9] About half of individuals who have sexual contact with an infected partner acquire the disease, with an estimated median infective dose of 50 bacteria.[10,11] T. pallidum penetrates mucosal surfaces and abraded skin, followed by attachment to host cells and multiplication of the microorganism. Treponemes disseminate to the regional lymph nodes and internal organs within a few hours.[12]
The lipoproteins and glycolipids present under the outer membrane of T. pallidum have been shown to activate the innate inflammatory response via toll-like receptor 4 (TLR4).[13] Toll-like receptors (TLRs) are a group of glycoproteins that function as surface transmembrane receptors involved in the innate immune response to exogenous pathogenic microorganisms.[14] Lipoproteins of T. pallidum are thought to gain access to TLRs on the surface of macrophages, which galvanizes their production of tumor necrosis factor.[15–17] These findings support the concept that the lipoproteins of spirochetes are the principal components responsible for activation of the innate immune response of the host.
If the patient is treated adequately, immunoglobulin M (IgM) antibody levels decline in the next 1 to 2 years, but IgG antibody usually persists during the lifetime of the patient. Despite the treponeme-specific antibody response, syphilis may still evolve through all of its different stages. The reason why the disease progresses despite abundant antibody responses is not clear, but suggests that humoral immunity is insufficient to clear active infection and that cellular immunity is required.[15] In addition, numerous treponemes are needed to activate the phagocytic response, and small numbers of treponemes may escape recognition.[17]
The patient described in this case report has cutaneous manifestations of the second stage of syphilis. The secondary stage of this disease results from the hematogenous and lymphatic dissemination of treponemes after a few weeks or months of inoculation (mean of 3–10 weeks). The skin lesions of secondary syphilis are called syphilids. These are generalized, nonpruritic, erythematous macules and papules that occur in 80 percent or more of cases. The presence of lesions on the palms and soles is strongly suggestive of secondary syphilis. However, generalized syphilids can spare the palms and soles.[18] Cutaneous lesions can range from 1 to 2mm to 15 to 20mm in diameter and vary in color from pink to violaceous to red-brown. Mucosal lesions range from small, superficial ulcers that resemble painless aphthae to large gray plaques. Condylomata lata—painless verrucous papules and erosions—are often observed in the moist regions of the anogenital area due to local spreading of the microorganisms.
Secondary syphilis also presents with systemic symptoms, including low-grade fever, malaise, sore throat, adenopathy, weight loss, and muscle pain. Lymph node enlargement is present in the majority of patients. Focal neurologic findings occasionally occur.[19]
Unusual presentations of secondary syphilis can imitate numerous diseases. Secondary syphilis may mimic cutaneous lymphoma, eczematous derrmatitis, and fungal infection.[20–22] Syphilis may also mimic drug eruptions, erythema multiforme, lichen planus, tinea versicolor, seborrheic dermatitis, mycosis fungoides, other lichenoid lesions, vesiculobullous lesions, and palmoplantar psorisiform dermatitis.[23,24]
Secondary syphilis may also mimic mycosis fungoides (MF) both clinically and pathologically in HIV patients. Atypical lymphoid infiltrates suggestive of MF have been reported in HIV-positive patients.[22] The clinician should obtain Warthin-Starry stains to search for treponemes in tissue specimens as well as serology tests for syphilis in MF-like eruptions in HIV-positive patients. Palomoplantar keratoderma associated with ocular involvement (conjuctivitis, uveitis, interstitial keratitis, and retinitis) also has been reported in patients with HIV.[25]
The estimated risk for symptomatic early neurosyphilis in patients with early syphilis coinfected with HIV is 1.7 percent. Forty-seven percent of neurosyphilitic cases occur in the secondary stage. Twenty-four percent of the cases occur in the early latent stage, while 18 percent occur in latent disease.[26]
In the setting of HIV infection, virulent T. pallidum can promote the induction of HIV gene expression in cells, possibly resulting in increased systemic HIV levels and more rapid progression of HIV infection.[27] The pathogenesis of syphilis in HIV may relate to a decrease in both cell-mediated and humoral immune response to T. pallidum. Decreased T-helper cell function results in decreased activation of B-cells, resulting in diminished immunoglobulin formation. In addition to decreased T-cells, the macrophages of HIV-infected patients suffer from functional deficits. Furthermore, it appears that T. pallidum itself may induce further immunosuppression, resulting in a synergistic decrease in the host response of HIV-infected individuals.[28]
A case series from Massachusetts General Hospital reported four men with concurrent HIV and syphilis who all had symptoms of neurosyphilis. Only 5 out of 140 HIV-negative patients with syphilis, on the other hand, had CSF-positive VDRL, suggesting that syphilis has a more aggressive natural history in the setting of HIV. Three ways in which the disease progression is altered include the following: 1) decreased latency period before the onset of neurosyphilis, 2) increased severity of the manifestations of neurosyphilis, and 3) inadequate treatment of patients with coinfection.[28] There are three known forms of neurosyphilis that occur in HIV-infected individuals—asymptomatic neurosyphilis, acute syphilitic meningitis, and meningovascular neurosyphilis. These rarely progress to classic tabes dorsalis. Acute meningovascular syphilis and syphilitic meningitis usually involve cranial nerves VII and VIII.
Similar to the authors’ patient, another case of erythematous palmoplantar macules and papules occurred in a 44-year-old HIV-infected man with a VDRL of 1:64. In this patient, the rash erupted as a result of immune reconstitution after the initiation of antiretroviral therapy, during which his CD4 count rose from 92cells/mm3 to 196cells/mm3. A single dose of intramuscular benzathine penicillin decreased the VDRL titer and improved the eruption.[29]
Under light microscopy, cutaneous syphilitic macules and papules are characterized by moderately intense perivascular inflammatory infiltrates in which plasma cells and macrophages predominate. In addition, neutrophils are visualized in the papillary dermis and may be seen in the epidermis. Spirochetes are very scant and may be seen within the epidermis and around superficial vessels.[30,31] The lesions either undergo no epidermal change or may be accompanied by slight vacuolar change at the dermoepidermal junction. However, papules and plaques usually show dense superficial and deep infiltrates consisting of lymphocytes, macrophages, and plasma cells distributed in a band-like pattern in the papillary dermis and cuffed around blood vessels. Psoriasiform epidermal hyperplasia and hyperkeratosis may also be seen. As lesions age, macrophages become more numerous so that granulomatous foci are often present, mimicking sarcoidosis.[31]
Uveitis is a reemerging complication of HIV patients coinfected with syphilis and may be the first presenting symptom. It is now the most common complication of secondary and tertiary syphilis.[32] One group diagnosed uveitis in 14 such patients out of 2,410 cases that presented to its referral center, which was greater than the prior rate of 0.11 per 1,000 in this academic center. In the study, all HIV-positive patients had signs of diffuse uveitis, while only one HIV-negative patient had panuveitis. Of the HIV-infected patients with ocular manifestations, the average age was 46. Ninety-three percent were male; 86 percent were heterosexual. Their mean CD4 cell count was 418cells/mL. Interestingly, less than half of such patients with ocular manifestations had positive CSF VDRL studies. Coinfected patients also had more complications than HIV-negative patients, such as tractional retinal detachment and cystoid macular edema.[33]
The diagnosis of neurosyphilis in HIV is challenging. Most reports have shown serologic titers that are higher than expected, as well as false-negative serologic test results and delayed appearance of seroreactivity. Some authors argue the need for more sensitive screening tools, such as recombinant antigen-based immunologic tests.[34] Nevertheless, both treponemal and nontreponemal serologic tests for syphilis can be interpreted in the usual manner for patients coinfected with HIV.[35] Treponemal tests include treponemal pallidum particle agglutination (TPPA) or FTA-ABS. Nontreponemal tests include VDRL and RPR. Nontreponemal tests have been traditionally used for initial screening due to higher sensitivity, followed by confirmation with treponemal tests. Reverse sequence testing is a more recent screening method in which treponemal tests are used initially and followed by nontreponemal testing. Although this technique may theoretically raise the level of false positives, it has been proposed to more readily detect latent syphilis that initial RPR and VDRL may miss. One study shows that the overall false-positive rate by reverse screening is the same as that reported by the CDC (0.6%) and is slightly higher than traditional screening (0.0%). However, another study showed the utility of the reverse algorithm in detecting two additional patients with latent syphilis not found by the conventional approach.[36] When clinical findings are suggestive of syphilis, but serologic tests are nonreactive or their interpretation is unclear, alternative tests (e.g., biopsy of a cutaneous lesion, darkfield examination, and PCR of lesion material) might be useful for diagnosis. Neurosyphilis should always be considered in the differential diagnosis of neurologic disease in HIV-infected persons.
Parenteral penicillin G has been an effective treatment for syphilis for more than 50 years. No tendency toward penicillin resistance has been detected in T. pallidum.[37] The most current treatment guidelines recommend 2.4MU of benzathine penicillin G administered intramuscularly for primary, secondary, and early latent syphilis in adults (defined as latent syphilis for less than one year).[35]
However, the recommendations differ for HIV-infected individuals. Compared with HIV-negative patients, HIV-positive patients who have early syphilis are at increased risk for neurological complications and have higher rates of serologic treatment failure with currently recommended regimens. Many experts believe that HIV-positive patients co-infected with syphilis should be treated with a course of antibiotics strong enough to treat neurosyphilis.[35] The regimen in this case is 18 to 24MU of IV aqueous crystalline penicillin G daily, administered as 3 to 4MU every four hours or continuous infusion for 10 to 14 days. Alternative regimens include 2.4MU of IM procaine penicillin once daily plus probenecid 500mg orally four times a day, both for 10 to 14 days. The durations of the recommended and alternative regimens for neurosyphilis are shorter than the duration of the regimen used for late syphilis in the absence of neurosyphilis. Therefore, 2.4MU of IM benzathine penicillin once weekly for up to three weeks can be considered after resolution of the other neurosyphilis treatment regimens to provide a comparable total duration of therapy. Careful follow-up after therapy is essential.[35] Penicillin therapy has even shown to reverse ocular involvement.[33]
Some authors question the efficacy of current treatment guidelines for neurosyphilis in HIV. The group at Massachussets General Hospital experienced treatment failure in three of four patients, each receiving 20 to 24MU of IV penicillin for 10 to 21 days.[28] Another study shows that the risk of persistent symptoms of neurosyphilis six months after treatment is 0.5 percent.[38] Another study of 541 cases by Rolfs et al39 (101 of which were HIV positive) showed that 18 percent of early syphilis serologically failed therapy at six months after a single dose of 2.4MU IM.[1] Of 131 patients, 32 (24 %) were positive for T. pallidum in the CSF at enrollment and 7 of 35 (20%) remained positive after treatment.[39]
The introduction of sexual health initiatives and clinics has been shown to improve HIV prevention.[40] For example, Avahan is a large-scale HIV prevention program in India that provides biannual syphilis screenings. A study of this population showed dramatic improvement in the seroreactivity of participants.[41]
All women should be screened serologically for syphilis early in pregnancy. Most states mandate screening all women at the first prenatal visit. Some evidence suggests that additional therapy can be beneficial for pregnant women in some settings (e.g., a second dose of benzathine penicillin 2.4MU IM administered 1 week after the initial dose for women who have primary, secondary, or early latent syphilis). When syphilis is diagnosed during pregnancy, consultation with obstetric specialists must be obtained. For treatment of syphilis during pregnancy, no adequate alternatives to penicillin exist. Pregnant women who have a history of penicillin allergy should be desensitized and treated with penicillin.[37]
For patients allergic to penicillin, treatment includes 100mg of oral doxycycline twice daily for 14 days, 500mg of oral tetracycline four times daily for 14 days, 1g of IM or IV ceftriaxone once daily for 8 to 10 days, or a single oral dose of 2g of azithromycin.
Conclusion:
The incidence of syphilis has declined since the institution of penicillin in 1941, reached a low in 2000, and increased since then in African Americans, Hispanics, and men who have sex with men. T. pallidum is the causative agent. Sexual contact is the most common mode of transmission. Cutaneous syphilis presents with low-grade fever, malaise, sore throat, adenopathy, weight loss, muscle pain, and a generalized nonpruritic papulosquamous eruption. HIV-positive patients who have early syphilis are at increased risk for neurologic complications and might have higher rates of serologic treatment failure. The currently recommended regimen is 18 to 24MU of IV penicillin G daily, administered as 3 to 4MU every four hours or continuous infusion for 10 to 14 days. A 33-year-old HIV-positive man presented with an eruption on his palms and soles with headaches, papilledema, and iritis consistent with neurosyphilis.
References
1. Centers for Disease Control and Prevention. Syphilis. http://www.cdc.gov/std/syphilis/stdfact-syphilis.htm. Accessed August 19, 2013.
2. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. www.cdc.gov/STD/syphilis2006 short.pdf. Accessed March 13, 2013.
3. Rolfs RT, Nakashima AK. Epidemiology of primary and secondary syphilis in 1981–1989. JAMA. 1990;264:1432–1437.
4. Zajdowicz T. STD/HIV Program. Chicago Dept of Public Health.
5. Centers for Disease Control and Prevention. Primary and secondary syphilis. http://www.cdc.gov/std/stats10/ syphilis.htm. Accessed January 21, 2013.
6. Gottlieb SL, Pope V, Sternberg MR, et al. Prevalence of syphilis seroreactivity in the United States: data from the National Health and Nutrition Examination Surveys (NHANES) 2001–2004. Sex Transm Dis. 2008(5):507–511.
7. Norris SJ. Polypeptides of Treponema pallidum: progress toward understanding their structural, functional, and immunologic roles. Treponema pallidum Polypeptide Research Group. Clin Microbiol Rev. 1993;57(3):750–779. Review. Erratum in: Clin Microbiol Rev. 1994;58(2):291.
8. Centers for Disease Control and Prevention. HIV and syphilis infection among men who have sex with men—Bangkok, Thailand, 2005–2011. MMWR Morb Mortal Wkly Rep. 2013;62(25):518–520.
9. Singh AE, Romanowski B. Syphilis: reviewed with emphasis on clinical and epidemiologic and some biologic features. Clin. Microbiol. Rev. 1999;12:187–209.
10. Magnuson HJ, Eagle H, Fleischman R. The minimal infectious inoculum of Spirochaeta pallida (Nichols strain) and a consideration of its rate of multiplication in vivo. Am J Syph Gonorrhea Vener Dis. 1948;32(1):1–18
11. Magnuson HJ, Thomas EW, Orlansky S. Inoculations syphilis in human volunteers. Medicine. 1956;35:33–82.
12. Aral SO, Holmes KK. Social and behavioral determinants of the epidemiology of STDs: industrialized and developing countries. In: Holmes KK, Sparling PF, Mardh P-A, et al, eds. Sexually Transmitted Diseases. New York: McGraw-Hill; 1999:39–76.
13. Schröder NW, Eckert J, Stübs G, Schumann RR. Immune responses induced by spirochetal outer membrane lipoproteins and glycolipids. Immunobiology. 2008;213:329–340.
14. Valins W, Amini S, Berman B. The expression of toll-like receptors in dermatological diseases and the therapeutic effect of current and newer topical toll-like receptor modulators. J Clin Aesthet Dermatol. 2010;3:20–29.
15. Peeling RW, Hook EW. The pathogenesis of syphilis: the great mimicker. J. Pathol. 2006;208:224–232.
16. Musher DM, Hague-Park M, Gyorkey F, et al. The interaction between Treponema pallidum and human polymorphonuclear leukocytes. J Infect Dis. 1983;147(1):77–86.
17. Thomas DD, Navab M, Haake DA, et al. Treponema pallidum invades intercellular junctions of endothelial cell monolayers. Proc Natl Acad Sci U S A. 1988;85(10):3608–3612.
18. Baughn RE, McNeely MC, Jorizzo JL, Musher DM. Characterization of the antigenic determinants and host components in immune complexes from patients with secondary syphilis. J Immunol. 1986;136(4):1406–1414.
19. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. Philadelphia, PA: Saunders; 2012.
20. Acharya V, Varghese GK, Roy A. Secondary syphilis mimicking cutaneous lymphoma. J Indian Med Assoc. 2011;109(3):196–197.
21. Mattei PL, Johnson RP, Beachkofsky TM, et al. Pruritic rash on trunk. J Fam Pract. 2011;60(9):539–542.
22. Liotta EA, Turiansky GW, Berberian BJ, et al. Unusual presentation of secondary syphilis in 2 HIV-1 positive patients. Cutis. 2000;66(5):383–386, 389.
23. Paz A, Potasman I. Oral lesions as the sole presenting symptom of secondary syphilis. Travel Med Infect Dis. 2004;2(1):37–39.
24. Patel A, Heath TC, Bowden FJ, Currie B. An unusual presentation of secondary syphilis in the Northern Territory. Australas J Dermatol. 1994;35(1):23–27.
25. Kirby JS, Goreshi R, Mahoney N. Syphilitic palmoplantar keratoderma and ocular disease: a rare combination in an HIV-positive patient. Cutis. 2009;84(6):305–310.
26. Centers for Disease Control and Prevention. Symptomatic early neurosyphilis among HIV-positive men who have sex with men—four cities, United States, January 2002-June 2004. MMWR Morb Mortal Wkly Rep. 2007;56(25):625–628.
27. Theus SA, Harrich DA, Gaynor R. Treponema pallidum lipoprotein and seemed that the lipoprotein and analogues induced human immunodeficiency virus type gene expression in monocyte via NF-B.vaccination. J. Infect. Dis. 1998;177:941–950.
28. Johns DR, Tierney M, Felsenstein D. Alteration in the natural history of neurosyphilis by concurrent infection with the human immunodeficiency virus. N Engl J Med. 1987;316(25): 1569–1572.
29. Vasudevan B, Verma R, Pragasam V, et al. A rare case of secondary syphilis manifesting as immune reconstitution syndrome in an HIV-positive patient. J Int Assoc Provid AIDS Care. 2013. [Epub ahead of print].
30. Mckee PH. Pathology of the Skin: With Clinical Correlations. 2nd ed. St. Louis, MO: Mosby-Year Book; 1996.
31. James WD, Berger T, Elston D. Andrews’ Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia: Saunders; 2011.
32. Aldave AJ, King JA, Cunningham ET Jr. Ocular syphilis. Curr Opin Ophthalmol. 2001;12(6):433–441.
33. Restivo L, Abbouda A, Nardella C, et al. Uveitis heralding previously unknown luetic and HIV infection. Syphilitic uveitis in an Italian referral center. Ann Ist Super Sanita. 2013;49(2):133–137.
34. Scythes JB, Jones CM. Syphilis in the AIDS era: diagnostic dilemma and therapeutic challenge. Acta Microbiol Immunol Hung. 2013;60(2):93–116.
35. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted disease treatment guidelines. MMWR Recomm Rep. 2006;55(RR-11):1–94.
36. Binnicker MJ, Jespersen DJ, Rollins LO. Direct Comparison of the traditional and reverse syphilis screening algorithms in a population with a low prevalenceof syphilis. J Clin Microbiol. 2012;50(1):148–150.
37. Centers for Disease Control and Prevention. Diseases characterized by genital, anal, or perianal ulcers. http://www.cdc.gov/std/treatment/2010/genital-ulcers.htm# syphilis. Accessed January 21, 2013.
38 Centers for Disease Control and Prevention. (2007, June 20). Symptomatic early neurosyphilis among HIV-positive men who have sex with men—four cities, United States, January 2002–June 2004. MMWR Morb Mortal Wkly Rep. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5625a1.htm
39 Rolfs RT, Joesoef MR, Hendershot EF, et al. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The Syphilis and HIV Study Group. N Engl J Med. 1997;337(5):307–314.
40 Snow AF, Vodstrcil LA, Fairley CK, et al. Introduction of a sexual health practice nurse is associated with increased STI testing of men who have sex with men in primary care. BMC Infect Dis. 2013;13(1):298.
41 Parthasarathy MR, Narayanan P, Das A, et al. Integrating syphilis screening in a large-scale HIV prevention program for key populations: the Avahan experience from India. J Infect Dev Ctries. 2013;7(6):484–488.