 J Clin Aesthet Dermatol. 2020;13(3):41–44
J Clin Aesthet Dermatol. 2020;13(3):41–44
by Lin Gao, MD, PhD and Hanmei Kang, MD; Yan Li, MD; Meiheng Lu, MD; Wenting Song, MD; Yuanli Wang, MD; Kai Li, MD, PhD; Li Wang, MD; and Gang Wang, MD, PhD
Drs. Gao, Kang, Lu, Song, Y. Wang, Li, L. Wang, and G. Wang are with the Department of Dermatology at Xi Jing Hospital of the Fourth Military Medical University in Xi’an, China.
FUNDING: Shaanxi scientific research grant #2016KTZDSF02-05 and 2016SF-374 were awarded to Dr. G. Wang.
DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: Background. The early signs of skin aging usually occur in the periocular region.
Objectives. This retrospective analysis evaluated the efficacy and safety profile of a multisource 3DEEP radiofrequency (RF) technology (EndyMed, Caesarea, Israel) in combination with fractional skin resurfacing (FSR) for the treatment of periocular skin aging.
Methods. A total of 15 patients with periocular aging underwent monthly treatment sessions of 3DEEP and FSR for three months. Sessions were administered at the Department of Dermatology at Xijing Hospital in Xi’an, China. Indices of skin moisture level, transepidermal water loss (TEWL), skin elasticity, wrinkles, pore size, and skin texture were determined before and after treatment using the Visia® (Canfield Imaging Systems, New Jersey), Multiprobe Adapter (CK, Cologne, Germany) and Antera3D® (Miravex, Dublin, Ireland) systems.
Results. Skin moisture level, elasticity, wrinkles, pore size, and texture improved relative to baseline (p<0.01). There was no significant difference in TEWL before and after the treatments (p>0.05). Patient satisfaction was 86.67 percent. Patients experienced varying degrees of transient edema, erythema, scabbing, and occasional hyperpigmentation; all adverse effects resolved within 2 to 10 days post-treatment.
Conclusion. ENDYMED 3DEEP in combination with FSR appears to be safe and effective in treating periocular skin aging. Randomized controlled trials with a larger patient group are needed to confirm our findings.
KEYWORDS: Multisource phase-controlled radiofrequency, fractional radiofrequency, facial rejuvenation, 3DEEP
The eyelid is one of the thinnest areas of skin on the human body.1 Early visible signs of facial aging usually appear first in the periocular region. Periocular skin aging is a result of collagen deficiency, shifting gravity, photoaging, and skin atrophy.1,2 Its clinical symptoms include local hyperpigmentation, volume loss, infraorbital hollow development, dynamic and static wrinkles, thinning of the eyebrows, and deepening of the superior sulcus. Treatment of the periocular region should be done cautiously due to thinness of the skin and close anatomic proximity to the eyeballs. Current treatment options include surgery, laser therapy, radiofrequency (RF) treatment, topical agents, chemical peels, and fillers.2 Each approach has advantages and disadvantages; for instance, filler injections can restore volume loss effectively, but results only last for 6 to 9 months.3 Fractional ablative lasers can resurface the skin, but are limited by the occurrence of prolonged edema and the development of hyperpigmentation.4
In the past decade, RF technology has demonstrated efficacy and safety for facial skin tightening.5 Compared to other methods, RF treatment provides several unique benefits to patients. RF noninvasively targets dermal collagen to induce collagen remodeling and formation by heating the tissue.6 In addition, the melanin content of the skin does not affect its outcomes.7 Further, it can penetrate deeply into the dermis and increase tissue volume.7 Finally, the results of RF treatment (i.e., skin tightening), can persist for 6 to 12 months.8,9 RF devices can involve monopolar, bipolar, multipolar, or multigenerator heating mechanisms.10 In monopolar RF devices, energy is released from a single electrode into the skin, which can be painful for patients, and active skin cooling is required during the process.11 In bipolar and multipolar RF, energy flows between two poles through the skin superficially, which might also require cooling during the process.5,10
The 3DEEP multisource RF technology (EndyMed, Caesarea, Israel) uses an array of electrodes driven by six independent phase-controlled RF generators.5 The 3DEEP multisource RF allows practitioners to control the energy flow with minimal side effects; thus, no active cooling is required. In this retrospective analysis, we evaluated the efficacy and safety of the 3DEEP platform in combination with fractional skin resurfacing (FSR) for the treatment of periocular skin aging.
Materials and Methods
Subjects. The present study was a retrospective analysis. Fifteen patients with periocular aging were treated with 3DEEP multisource radiofrequency and FSR in the Department of Dermatology at Xijing Hospital from April 2017 to September 2017. The subjects ranged in age from 35 to 60 years, with an average age of 43±0.5 years old. Clinical symptoms included periocular wrinkles, periocular hyperpigmentation, sagging eyelids, and ptosis.
Exclusion criteria for treatment included pregnancy, skin ulceration, coagulation disorders, use of photosensitizing or anticoagulation agents, history of skin rejuvenation therapies, including botulinum toxin and filler injections, six months prior to the study, history of laser therapy or chemical resurfacing, pacemaker implantation, and systemic diseases including cardiovascular disease, epilepsy, active vitiligo, and psoriasis. The risk factors and potential contraindications to using this treatment were discussed with patients before informed consent was sought. Written consent forms were obtained from all patients prior to the study.
Treatment and evaluation. The multisource 3DEEP RF treatment platform was used in this study. The periocular region of the patients was cleaned and first treated with the iFine handpiece (EndyMed, Caesarea, Israel) with energy fluences of 3 to 4 W, which facilitates skin tightening in periorbital areas. A total of 6 to 10 passes (each pass is equal to 30 seconds of RF emission) was performed, with 5% lidocaine gel applied to the area before treatment. A second treatment with FSR was performed one hour after the first treatment. The energy fluences were 4 to 6 W, and the pulse width was 20ms. Patients were counseled to use moisturizer and protect themselves from sun exposure the first three days after treatment. Patients underwent three treatment sessions at monthly intervals.
Digitalized high-resolution photographs combined with data from the Visia (Canfield Imaging Systems, New Jersey), Multiprobe Adapter (CK, Cologne, Germany) and Antera3D (Miravex, Dublin, Ireland) systems were used to evaluate outcomes. Images were taken at baseline, immediately after treatment, and one month after each treatment. Clinical evaluations were performed by two independent dermatologists.
Indices of skin moisture level, transepidermal water loss (TEWL) and skin elasticity were determined before and after each treatment by Multiprobe Adapter analysis. The indices of wrinkles, pore size, skin texture, the maximum depth of wrinkles (MDW), and quantity of pores were determined before and after each treatment using Visia and Antera3D. The pain score was evaluated by Visual Analog Scale (0–10 points) immediately after treatment. A patient satisfaction survey was administered one month after the final treatment. Patients rated their satisfaction as unsatisfied, neutral, satisfied, or very satisfied. The total satisfaction rate was the sum of satisfied and very satisfied rates. Side effects were also recorded.
Statistical analysis. The SPSS version 19.0 software program (IBM Corp., Armonk, New York) was used for data analysis. A paired Student’s t-test was used to compare the efficacy before and after treatment, and p<0.05 was considered statistically significant.
Results
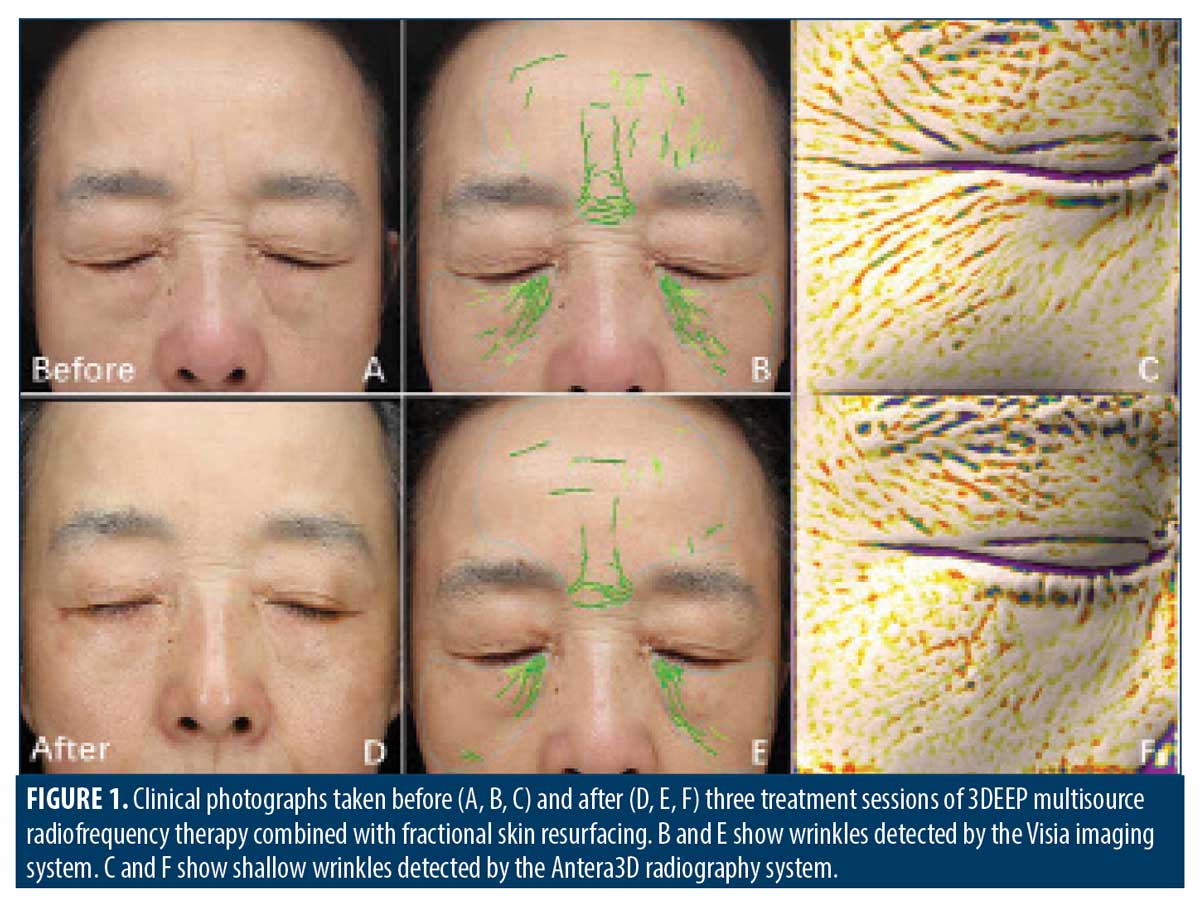
All subjects showed some degree of improvement in periocular wrinkles, skin texture, and elasticity after combined treatment with the iFine and FSR handpieces (Figure 1). Multiprobe Adapter analysis showed there were significant increases in the indices of skin moisture level and elasticity after the second treatment compared to baseline (p<0.01 or 0.001) (Table 1). There was no significant difference in TEWL before or after three passes of the combined treatments (p>0.05) (Table 1). There were significant increases in the MDW and indices of wrinkles, pore size, and texture after each treatment, relative to baseline (p<0.05 or 0.001) (Table 1). The pore number showed a significant decrease after the second treatment compared to baseline (p<0.05) (Table 1). According to the patient follow-up surveys, six patients reported feeling very satisfied, seven patients reported feeling satisfied, and two patients reported feeling neutral about their results (Figure 2). The overall patient satisfaction rate was 86.67 percent.


All patients tolerated the therapeutic regimen well. Some patients experienced varying degrees of transient pain, with a pain score ranging from 2 to 5 points during the treatment procedures. Variable degrees of transient edema, erythema, scabs, and hyperpigmentation were observed after each treatment, but these adverse effects resolved within 2 to 10 days after the treatment sessions. We did not observe scar formation or blisters in patients after the treatments.
Discussion
Several types of energy-based facial rejuvenation techniques have evolved rapidly over the past decade, including lasers, light-based devices, and non-light-based thermal tightening devices, such as RF systems. A laser or light-based energy interacts with the chromophores, such as hemoglobin, melanin, or water, within the skin to induce photomodulation.12 RF emits an electrical current that converts to thermal energy due to the natural electrical resistance of molecules in the tissue.13 Such will result in minimal tissue damage and allow epidermal melanin to remain intact, making it applicable to all skin types.14 An immediate skin contraction can be induced by RF due to collagen coagulation when heating the dermis 40°C to 48°C. Collagen denaturation-induced long-term tissue remodeling will occur around 55°C to 70°C.10,15–19 At a molecular level, RF can induce the upregulation of the expressions of many genes, including heat shock proteins, transforming growth factor beta, and vascular endothelial growth factor.10 Histologically, RF can instantly cause partial or complete collagen fibril helix denaturation, collagen contraction, and dermal edema induced by collagen injury. Long-term effects involve collagen and elastin remodeling and reorientation due to the stimulation of fibroblasts.10,20–22 RF technologies have evolved rapidly from monopolar, bipolar, and multipolar systems to multigenerator systems based on heating mechanisms. The energy that flows throughout the skin and the cells in the first-generation monopolar devices was uncontrolled, resulting in some significant side effects, including tissue necrosis.11 The 3DEEP multisource RF system overcomes these problems using six independent phase-controlled RF generators, which allows for selective heat conduction through the dermis and the fibrotic tissue within the skin.5 Currently, RF devices implemented with the 3DEEP multisource RF technology have demonstrated efficacy for face and neck skin tightening with few side effects.5,23 However, one limitation of RF technology is tissue-selective targeting, which cannot be easily addressed by current RF platforms. Combining modalities, such as RF and ultrasound or laser-based therapy, has provided some benefits to patients. Another strategy is to combine RF with the injection of fillers and toxins to achieve tissue recontouring.5
The early and most prominent features of the aging process first occur in the periocular region. Many factors contribute to periocular skin aging, including collagen deficiency, shifting gravity, photoaging, and skin atrophy.1,24,25 Eyelid hyperpigmentation, thinning of the eyebrows, volume loss, and development of dynamic and static wrinkles are the main clinical features inherent in periocular skin aging.1,25 The ENDYMED iFine handpiece is specifically designed to facilitate skin tightening of periocular areas. Our previous clinical observations revealed that such a treatment with the ENDYMED iFine handpiece could effectively improve skin laxity, but was less effective on wrinkles in periocular areas, with an injection of botulinum toxin required to correct the wrinkles.26 Literature reports have shown that ablative fractional laser technology can effectively improve wrinkles.27 The FSR handpiece functions using a mechanism similar to ablative fractional laser technology, delivering fractional RF energy to cause an array of microscopic thermal zones.28 The spatially defined thermal injury columns contain coagulated collagen, leading to skin shrinkage. The untreated areas serve as reservoirs to facilitate a rapid repair and remodeling process.29 In this study, we first used the iFine handpiece for skin tightening, followed by a second treatment using the FSR handpiece for targeting wrinkles in the periocular region. Our results indicated significant improvements in the indices of skin moisture level, skin elasticity, wrinkles, pore size, and skin texture using this treatment strategy. The limitations of this study include small sample size and lack of long-term efficacy evaluation.
Conclusion
The combination of the multisource 3DEEP RF treatment platform and FSR treatments appear safe and effective for improving signs of periocular aging. The underlying theory based on this strategy is that the 3DEEP RF treatment results in skin tightening and FSR improves wrinkles, leading to an overall rejuvenation of aging periocular skin. No serious adverse effects were observed. Randomized, controlled trials with a larger patient sample are needed to confirm our findings.
References
- Bernardini FP, Gennai A, Izzo L, et al. Superficial enhanced fluid fat injection (SEFFI) to correct volume defects and skin aging of the face and periocular region. J Aesthet Surg. 2015;35(5):504–515.
- Pak CS, Lee YK, Jeong JH, et al. Safety and efficacy of Utthera in the rejuvenation of aging lower eyelids: a pivotal clinical trial. J Aesthetic Plast Surg. 2014;38(5):861–868.
- Wei Qian, Yan-Kun Zhang, Qian Cao, et al. Clinical application of earlobe augmentation with hyaluronic acid filler in the chinese population. Aesthetic plastic Surgery. 2017;41(1):185–190.
- Mu YZ, Jiang L, Yang H, et al. The efficacy of fractional ablative carbon dioxide laser combined with other therapies in acne scars. Dermatol Ther. 2019, 32(6):1396–0296.
- Harth Y. Painless, safe, and efficacious noninvasive skin tightening, body contouring, and cellulite reduction using multisource 3DEEP radiofrequency. J Cosmet Dermatol. 2015;14(1):70–75.
- Wakade DV, Nayak CS, Bhatt KD. A study comparing the efficacy of monopolar radiofrequency and glycolic acid peels in facial rejuvenation of aging skin using histopathology and ultrabiomicroscopic sonography (ubm)–an evidence based study. Acta Medica. 2016, 59(1):14–17.
- Kaufman Joely, Goldberg David. Reviewing radiofrequency. Dermatology Times. 2007;28(9): 80–81.
- Hilal Gokalp. Efficacy of monopolar radiofrequency in middle and lower face laxity. J Turgut Ozal Med Cent. 2017;24(3):274–278
- Jones IT, Guiha I, Goldman MP, et al. A randomized evaluator-blinded trial comparing subsurface monopolar radiofrequency with microfocused ultrasound for lifting and tightening of the neck. Dermatol Ther. 2017, 43(12):1441–1447.
- Gentile RD, Kinney BM, Sadick NS. Radiofrequency technology in face and neck rejuvenation. J Facial Plast Surg Clin N Am. 2018;26(2):123–134.
- Weiss RA, Weiss MA, Munavalli G, et al. Monopolar radiofrequency facial tightening: a retrospective analysis of efficacy and safety in over 600 treatments. J Drugs Dermatol. 2006;5(8):707–712.
- Hong SE, Hong MK, Kang SR, et al. Effects of neodymium–yttrium–aluminum garnet (Nd:YAG) pulsed high-intensity laser therapy on full thickness wound healing in an experimental animal model . J Cosmet Laser Ther. 2016;18(8):6.
- Nestor MS, Bass A, Kleinfelder RE. Non-ablative radiofrequency for hyperhidrosis. Lasers, Lights and Other Technologies. 2018:389–394.
- Britt CJ, Marcus B. Energy-based facial rejuvenation advances in diagnosis and treatment. J JAMA Facial Plast Surg. 2017;19(1):64–71.
- Arnoczky SP, Aksan A. Thermal modification of connective tissue. Basic science considerations and clinical impressions. J Am Acad Orthop Surg. 2000;8(5):305–313.
- Dierickx C. The role of deep heating for non-invasive skinrejuvenation. J Lasers Surg Med. 2006;38(9):799–807.
- Sadick NS, Makino Y. Selective electro-thermolysis in aesthetic medicine: a review. J Lasers Surg Med. 2004;34(2):91–97.
- Sadick NS, Mulholland RS. A prospective clinical study tevaluate the efficacy and safety of cellulite treatment using the combination of optical and RF energies for subcutaneous tissue heating. J Cosmet Laser Ther. 2004;6(4):187–90.
- Childs S, Smirnovs M, Zelenchuk A, et al. Selective electro-thermolysisin aesthetic medicine: a review. J Lasers Surg Med. 2004;34(2):91–97.
- Chipps LK, Bentow J, Prather HB, et al. Novel nonablative radio-frequency rejuvenation device applied to the neck and jowls: clinical evaluation and 3-dimensional image analysis. J Drugs Dermatol. 2013;12(11):1215–1218.
- Sadick N, Sorhaindo L. The radiofrequency frontier: a review of radiofrequency and combined radiofrequency pulsed-light technology in aesthetic medicine. J Facial Plast Surg. 2005;21(2):131–138.
- Sadick NS, Trelles MA. A clinical, histological, and computer-based assessment of the Polaris LV, combination diode, and radiofrequency system, for leg vein treatment. J Lasers Surg Med. 2005;36(2):98–104.
- Elman M, Harth Y. Novel multi-source phase-controlled radiofrequency technology for non-ablative and micro-ablative treatment of wrinkles, lax skin and acne scars. J Laser Ther. 2011;20(2):139–144.
- Pak CS, Lee YK, Jeong JH, et al. Safety and efficacy of ulthera in the rejuvenation of aging lower eyelids: a pivotal clinical trial. J Aesthetic Plast Surg. 2014,38(5):861–868.
- Chopra K, Calva D, Sosin M, et al. A comprehensive examination of topographic thickness of skin in the human face. J Aesthet Surg J Nov. 2015;35(8): 1007–1013.
- Jeon IK, Chang SE, Park GH, et al. Comparison of microneedle fractional radiofrequency therapy with intradermal botulinum toxin a injection for periorbital rejuvenation. Dermatology. 2014; 227(4):367–372.
- Hantash BM, Bedi VP, Chan KF, et al. Ex vivo histological characterization of a novel ablative fractional resurfacing device. J Lasers Surg Med. 2007;39(2):57–95.
- Dahan S, Rousseaux I, Cartier H, et al. Multisource radiofrequency for fractional skin resurfacing—significant reduction of wrinkles. J Cosmet Laser Ther. 2013;15(2):91–97.
- Sadik N, Sato M, Palmisano D, et al. In vivo animal histology and clinical evaluation of multisource fractional radiofrequency skin resurfacing (FSR) applicator. J Cosmet Laser Ther. 2011;13(5):204–209.