Andrea LaTorre, MD; Department of Dermatology, The Ohio State University Medical Center, Columbus, Ohio; Lana Alghothani, BS; The Ohio State University Medical Center, Columbus, Ohio; David Lambert, MD; The Ohio State University Medical Center, Columbus, Ohio; Kris R. Jatana, MD; Department of Otolaryngology—Head and Neck Surgery, Nationwide Children’s Hospital and The Ohio State University Medical Center, Columbus, Ohio; Sara Peters, MD; Department of Pathology, The Ohio State University Medical Center, Columbus, Ohio; Jill Foster, MD; and Robert Hill, MD; Department of Pathology, The Ohio State University Medical Center, Columbus, Ohio; Department of Ophthalmology, The Ohio State University Medical Center, Columbus, Ohio; Nationwide Children’s Hospital and The Eye Center of Columbus, Columbus, Ohio
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Malignancies of the ocular adnexa are rare, aggressive tumors with significant potential for local recurrence and metastases. Although basal cell carcinoma remains the most common malignancy of the eyelid, encompassing more than 90 percent of all periocular cancers, several other malignant neoplasms have been reported. Malignant ocular adnexal neoplasms are most commonly of sweat gland origin and include hidradenocarcinoma, mucinous eccrine adenocarcinoma, and apocrine adenocarcinoma of the glands of Moll. The different ocular adnexal adenocarcinomas share many of the same characteristics with regard to incidence, primary location, and rates of recurrence and metastases. As a result, these tumors are difficult to distinguish clinically and true diagnosis depends on histological findings. The highest incidence of the reported cases occurred during the sixth decade of life. The head, neck, and trunk are the most frequently reported primary locations. Ocular adnexal adenocarcinomas have a significant rate of metastasis to regional lymph nodes as well as distant sites. Standard treatment of care includes surgical excision of the tumor; however, these malignancies have a tendency to recur locally. The authors present a 14-year-old Caucasian girl with no significant past medical history who presented with a recurrent right lower eyelid tumor. She previously had multiple resections at an outside hospital; however, the margins could not be cleared. The patient was taken to the operating room for Mohs-type resection of the primary site as well as a right parotidectomy with facial nerve preservation and right modified radical neck dissection. The final pathology was consistent with a mucin-producing malignant tumor of ocular adnexa. Due to the great potential for local recurrence and metastases, the prognosis for ocular adnexal adenocarcinoma remains poor even with aggressive surgical management. The use of Mohs surgery for resection has increased as it has been linked to prolonged intervals of metastatic-free disease. (J Clin Aesthet Dermatol. 2012;5(4):44–47.)
Although rare, several types of ocular adnexal adenocarcinomas have been reported in the literature. The three most reported include hidradenocarcinoma, mucinous eccrine adenocarcinoma, and apocrine adenocarcinoma of glands of Moll, all of which are of sweat gland origin.[1] These tumors are difficult to distinguish clinically, as they share many characteristics with regard to incidence, primary location, and rates of recurrence and metastases; therefore, true diagnosis depends on histological findings. In this report, the authors briefly discuss the important aspects of each of these tumors, as it is essential to include these neoplasms in the differential diagnosis of a recurrent eyelid tumor.
Hidradenocarcinoma (HC) was first described by Keasby and Hadley in 1954 as a clear cell eccrine tumor.[2] The term hidradenocarcinoma is one of several, including malignant acrospiroma and clear cell hidradenocarcinoma,[3] used to describe an aggressive, malignant tumor of eccrine sweat glands. One of 13,000 biopsies sent to dermatopathology is consistent with a malignant eccrine tumor, six percent of which are HCs.[4] Of the cases reported, the highest incidence of a HC occurred during the sixth decade of life; however, at least one case has been documented in every decade.[5] The incidence of a HC is similar in men and women.[6] The head, neck, and trunk are the most frequently reported primary locations.[7] Furthermore, this tumor has a tendency to recur locally, with a rate ranging from 10 to 50 percent.[8] HC has a significant rate of metastasis to regional lymph nodes as well as distant sites, with rates reported to be as high as 60 percent.[9] It has also been estimated that approximately 40 percent of affected patients die from their metastatic disease.[10] HC has eccrine and apocrine histological features.[11] On histological analysis, both poroid and cuticular cells are commonly seen; poroid cells are characterized by dark nucleoli scattered within a pale blue nucleoplasm. Cuticular cells are similar to poroid cells, with the exception of paler and larger nuclei.[11] In addition, scattered atypical cells with visible mitoses are present.[11]
Mucinous eccrine adenocarcinoma (MEC) was first described by Lennox et al in 1952 as a rare eccrine gland adenocarcinoma.[12] MEC most commonly affects older patients, with a median age of onset of 63 years[13]; however, it tends to have a male predilection with a male-to-female ratio of 2:1.[13] Most frequently found on the face, MEC affects the eyelid in more than 40 percent of reported cases.[13] Although MEC has a high probability of recurring locally, with rates ranging from 30 to 40 percent,[13–15] the rate of distant metastases is relatively low.[14,15] However, MEC has been reported to invade tissues by direct extension as well as via regional lymph node invasion.[16,17] Characteristic histological features of MEC include two epithelial cell populations forming a nest of cells; dark cells with heavy mucin production are located in the periphery around centrally located pale cells with little mucin production.[18–20]
Very few cases of apocrine adenocarcinoma of glands of Moll have been reported in the literature; however, of those described, several cases have been characterized by having a slow indolent course and, as a result, a low malignant potential.[21] Nevertheless, others have described a much more aggressive behavior with high malignant potential and evidence of lymphatic and perineural invasion.[22] In addition, apocrine adenocarcinoma of glands of Moll tends to affect the older population, with most patients between 50 and 60 years of age.[21,22] On histological exam, the tumor is composed of two cell layers; the inner layer is characteristic of the secretory appearance of apocrine glands with areas of decapitation secretion, while the outer layer is composed of small spindle cells.[23]
Standard treatment of ocular adnexal adenocarcinoma includes surgical resection of the tumor. Various studies have advocated the use of Mohs surgical resection as it has been linked to increased lengths of metastatic-free disease.[8]
Case Report
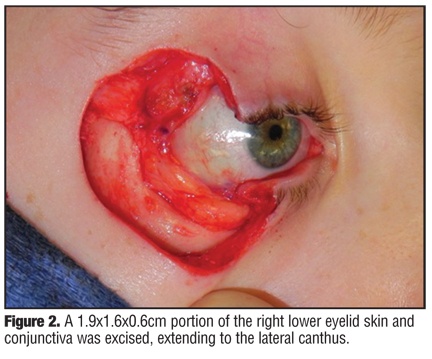
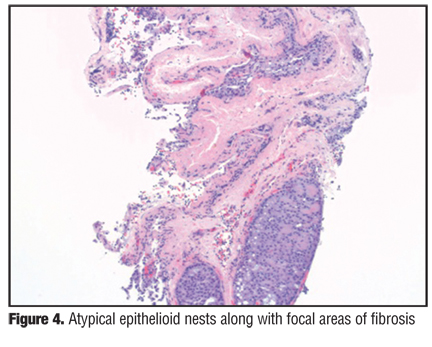
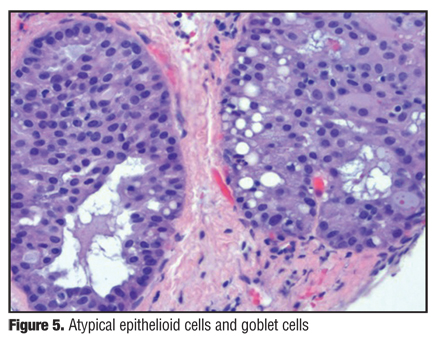
The authors present an otherwise healthy 14-year-old Caucasian girl with a recurrent right lower eyelid tumor (Figure 1) who presented to Nationwide Children’s Hospital and The Ohio State University Medical Center for further management. The patient underwent multiple resections of the mass at an outside hospital. Initially, the biopsies showed a benign neoplasm; however, the most recent pathology demonstrated adnexal malignancy. During the most recent resection performed at the outside hospital, sentinel lymph node biopsies (SLNBs) of the parotid and upper neck regions were completed. The SLNBs were negative; however, abnormal parotid tissue was present, positive for adnexal malignancy. In addition, there was a positive margin on the right lower eyelid resection. The patient received positron emission tomography (PET)/computerized tomography (CT) imaging, which did not localize the tumor, but rather showed diffuse bone marrow activity. A bone marrow aspiration was done and found to be normal. The patient was taken to the operating room (OR) for Mohs-type resection of the primary site as well as right parotidectomy with facial nerve preservation and right modified radical neck dissection (levels 1–5). A 1.9×1.6×0.6cm portion of the right lower eyelid skin and conjunctiva was excised, extending to the lateral canthus (Figure 2). A blue papule, measuring 0.4×0.2cm, was present within the excised skin. On pathological examination, focal areas of fibrosis were apparent in the dermis (Figure 3, Figure 4, and Figure 5). In addition, goblet cells were present within nests of atypical epithelioid cells. Lymph nodes of both the right parotid and right neck region were removed. No evidence of malignancy in the lymph nodes was demonstrated. However, atypical epithelioid cells, goblet cells, and fibrosis were apparent throughout a sample of parotid tissue. Pathology also demonstrated positive eyelid deep margins; therefore, the patient was taken back to the OR for a second resection of the primary site. During this procedure, a 3.0×2.2×0.4cm region was excised from the right lateral lower eyelid area. The Mohs-type margins were free of tumor and the patient returned to the OR the following day for reconstruction of the upper and lower eyelid defect. The final pathology was consistent with a mucin-producing malignant tumor of the ocular adenexa. All cranial nerves were intact postoperatively. Adjuvant radiation therapy was completed, and the patient is clinically free of disease 14 months after surgery (Figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
Although rare, especially in young persons, adeno-carcinoma of the ocular adnexa can be devastating. Most commonly affecting patients in the sixth decade of life, it is rarely seen in younger patients. Although uncommon, this malignant neoplasm should be included in the differential of abnormal growth in the pediatric population. It is essential that dermatologists, family physicians, and pediatricians alike are able to suspect a potentially malignant neoplasm in order to quickly refer the affected patient to appropriate specialists. Even with aggressive surgical management, the prognosis remains poor. Recently, however, the use of Mohs surgery for ocular adnexal adenocarcinoma resection has increased as it has been linked to prolonged intervals of metastatic-free disease.[8] Furthermore, as previously stated, the most common locations of the primary tumor include the head and neck, attributing to a cosmetic concern. Mohs surgery not only allows for complete removal of tumor and its margins, but is also tissue sparing. Due to the rarity of this tumor, SLNBs and regional lymphadenectomy have not been widely studied; however, they are recommended by some[11] and should be considered in the management. It is a challenge to manage tumors like the one presented, as the microscopic disease was not radiographically identified pre-operatively using CT, MRI, or PET-CT. Interestingly, no regional lymph nodes were involved despite microscopic metastatic disease to the parotid gland.
In this case, given the multiple recurrences, eyelid resections were performed by an oculoplastic surgeon and a Mohs surgeon present in the OR. The excised eyelid specimens were grossly subsectioned, inked, and mapped by the Mohs surgeon in both of the surgeries. Tissue was processed for Mohs-type paraffin sections, stained with hematoxylin and eosin, with interpretations done by a dermatopathologist. The lymph node and parotid resections were done by an otolaryngologist–head and neck oncologic surgeon who primarily managed the patient’s care. This case demonstrates the complex nature of diagnosing an eyelid tumor in a pediatric patient as well as the effectiveness of multispecialty management.
References
1. Shields J, Shields C. Eyelid, Conjunctival, and Orbital Tumors: An Atlas and Textbook. 2nd ed. Philadelphia: Lippincott; 2007.
2. Keasbey L, Hadley G. Clear cell hidradenoma; report of three cases with widespread metastases. Cancer. 1954;7:934–952.
3. Ohto M, Hiramoto M, Fujii M, Togo T. Nodular hidradenocarcinoma on the scalp of a young woman: case report and review of literature. Dermatol Surg. 2004;30:1265–1268.
4. MaCalamont TH. A call for logic in classification of adnexal neoplasms. Am J Dermatopathol. 1996;18:6.
5. Hernandez-Perez E, Cestoni-Parducci R. Nodular hidradenoma and hidradenocarcinoma. J Am Acad Dermatol. 1985;12:15–20.
6. Driscoll J, Gauerke S, Monahan B. Mechanistic and treatment implications of DNp63 expression in a rare case of metastatic hidradenocarcinoma. Case Rep Oncol. 2009;2:44–52.
7. Yavel R, Hinshaw M, Rao V, et al. Hidradenomas and a hidradenocarcinoma of the scalp managed using Mohs micrographic surgery and a multidisciplinary approach: case reports and review of the literature. Dermatol Surg. 2009;35:273–281.
8. Wildemore JK, Lee JB, Humphreys TR. Mohs surgery for malignant eccrine neoplasms. Dermatol Surg. 2004;30: 1574–1579.
9. Ashley I, Smith-Reed M, Chernys A. Sweat gland carcinoma: case report and review of the literature. Dermatol Surg. 1997;23:129–133.
10. Abenoza P, Ackerman AB. Hidradenomas. In: Abenoza P, Ackerman AB, eds. Neoplasms with Eccrine Differentiation. Philadelphia: Lea and Febiger; 1990:311–350; 485–487.
11. Ko CJ, Cochran AJ, Eng W, Binder SW. Hidradenocarcinoma: a histological and immunohistochemical study. J Cutan Pathol. 2006;33:726–730.
12. Lennox B, Pearse AG, Richards HG. Mucin secreting tumors of the skin. With special reference to the so-called mixed salivary tumor of the skin and its relation to hidroadenoma. J Pathol Bacteriol. 1952;64:865–880.
13. Wright JD, Font RL. Mucinous sweat gland adenocarcinoma of eyelid: A clinicopathologic study of 21 cases with histochemical and electron microscopic observations. Cancer. 1979;44:1757–1768.
14. Bindra M, Keegan DJ, Guenther T. Primary cutaneous mucinous carcinoma of the eyelid in a young male. Orbit. 2005;24:211–214.
15. Sudesh R, Siddique S, Pace L. Primary eyelid mucinous adenocarcinoma of eccrine origin. Ophthalmic Surg Lasers. 1999;30:394–395.
16. Wick MR, Goellner JR, Wolfe JT. Adnexal carcinomas of the skin. Cancer. 1985;56:1147–1162.
17. Stout AP, Cooley SG. Carcinoma of sweat glands. Cancer. 1951;4:521–536.
18. Wick MR, Coffin CM. Sweat gland and pilar carcinomas. In: Wick MR, ed. Pathology of Unusual Malignant Cutaneous Tumors. New York: Marcel Dekker, 1985:1–76.
19. Lever WF, Schaumberg-Lever G. Histopathology of the Skin. 7th ed. Philadelphia: JB Lippincott; 1990.
20. Santa Cruz DJ. Sweat gland carcinomas: a comprehensive review. Semin Diag Pathol. 1987;4:38–74.
21. Ni C, Wagoner M, Kieval S, Albert DM. Tumors of the Moll’s glands. Br J Ophthalmol. 1984;68:502–506.
22. Thompson SJ, Tanner NSB. Carcinoma of the apocrine glands at the base of eyelashes. A case report and discussion of histological diagnostic criteria. Br J Plast Surg. 1989;42: 598–602.
23. Shintaku M, Khoji T, Yoshida H, et al. Apocrine adenocarcinoma of the eyelid with aggressive biological behavior: report of a case. Pathol Int. 2002;52:169–173.