Leon H. Kircik, MD, Indiana University School of Medicine, Indianapolis, Indiana; Mount Sinai Medical Center, New York, New York; DermResearch, PLLC, Louisville, Kentucky
Abstract
Initiation of effective topical therapy as early as possible within the disease course is associated with improved patient experiences and better therapeutic outcomes in most dermatological diseases. Additionally, patient adherence is associated with better outcomes and lower long-term treatment costs, while poor adherence is directly linked to poor treatment results and patient dissatisfaction. Local cutaneous irritation associated with topical drug formulations has been an historical challenge to therapy initiation and adherence. Retinoids and benzoyl peroxide—essential elements of topical acne treatment—are two of the drugs most commonly associated with application-site adverse events. Novel approaches to product formulation incorporating microsphere technology may improve treatment tolerability, encourage adherence, and contribute to better long-term therapeutic outcomes. Microsphere technology eliminates the rapid delivery of high concentrations of active drug to the application site and instead facilitates controlled release of potentially irritating drugs. It is associated with improved treatment outcomes and minimal irritation. Microsphere formulations of topical tretinoin and benzoyl peroxide currently on the market have demonstrated good efficacy and tolerability and are expected to encourage adherence and long-term therapeutic benefit.
(J Clin Aesthet Dermatol. 2011;4(5):27–31.)
Initiation of effective therapy as early as possible within the disease course is associated with improved patient experiences and better therapeutic outcomes in most dermatological conditions.[1–5] Furthermore, data confirm that patient adherence is associated with better outcomes and lower long-term treatment costs.[6,7] Poor adherence is directly linked to poor treatment results and patient dissatisfaction.[5]
Irritation commonly associated with topical therapies is one of the most significant factors contributing to lack of adherence and therefore therapeutic withdrawal. The local application-site reactions may be linked to components of the formulation and/or to the active drug itself.[8] Among the most commonly used topicals, retinoids and benzoyl peroxide (BPO) are inherently irritating and historically associated with poor tolerability, resulting in limited patient adherence.[9,10] Still, current guidelines for the treatment of patients with mild-to-moderate acne emphasize the use of topical retinoids and either BPO alone or BPO in combination with clindamycin.[9,10] In fact, BPO and tretinoin are among the most commonly prescribed topical treatments for acne.[11] Recent concern about the development of bacterial resistance has led to increased dependence on topical BPO. Propionibacterium acnes—the commensal micro-organism that contributes to the development of acne vulgaris—has not developed resistance to BPO due to its unique mechanism of action.[12]
In the case of both tretinoin and BPO, irritation is concentration-dependent and is shown to be influenced by characteristics of the delivery system and formulation as well as the patients’ skin type. As such, numerous efforts have been made to reduce irritation by reducing the concentration of active drug or incorporating ingredients into the vehicle that are intended to hydrate and offset the irritating effects of the drugs.[8]
Nonetheless, therapy-associated irritation remains a prevalent problem that contributes to poor patient adherence.[12,13] A recent study of adherence in acne therapy represents the largest such study to date. Multivariate analysis of survey data showed that poor adherence was not directly correlated with young age (adherence was lowest in those younger than 15 years, but was also low in the age group from 15–25 years), the occurrence of side effects, and lack of patient satisfaction with treatment, among other factors.[13]
One approach to improving treatment tolerability is through controlled-release delivery of potentially irritating drugs. Facilitating the delayed release of topically applied drugs presented a challenge to drug formulators for some time. This obstacle has been overcome through the use of microsponge technology that releases the active agent slowly over time. Topical microsponge delivery is associated with improved therapeutic outcomes and minimal irritation.[14] Microsponges are biologically inert polymer particles that absorb, trap, or bind drugs or other chemical compounds. The macroporous beads, which typically measure 10 to 25µm in diameter, release active ingredient over time or in response to certain stimuli, such as change in pH, temperature, or physical manipulation when rubbed into the skin.[14]
Drugs that are not soluble in water can be entrapped in microsponge pores, which are extremely small; thus, the drug functions as microscopic particles, producing a greater surface area and increasing the rate of solubilization.[15]
In simplest terms, microspheres are formed through a quasi-emulsion solvent diffusion method. An organic internal phase consisting of drug, ethyl alcohol, polymer, and triethyl citrate (TEC)/trichloromethane is introduced to an external phase of distilled water and polyvinyl alcohol (PVA) that is allowed to emulsify and then is continuously stirred for two hours. This mixture is then filtered to obtain the microsponges.[15] Another way of synthesizing microspheres is free radical suspension polymerization.
Particle size, pore structure, diameter, volume, and release characteristics of the microsponge will determine the functional parameters. Particle size itself may influence the release rate of the active drug from the microsponge: The larger the particle size, the faster the release rate. The amount of the active ingredient in the particle also depends on the pore value. The diameter of the pores may affect the intensity and duration of the effectiveness of active ingredient. Resilience of the particle depends on cross-linking during polymerization. More than 10-percent cross-linking can slow down the release rate.[15]
The ratio of drug to polymer used during production is an important determinant of both production yield and the amount of drug trapped within microspheres. At a 1:1 drug-to-polymer ratio in a study of experimental BPO microsponges, researchers found a very low yield production (less than 15%) and achieved maximal production at a ratio of 13:1. Higher drug-to-polymer ratios produce higher drug-loading efficiency. However, even at the highest ratios of 11:1 and 13:1, drug-loading efficiency did not reach 100 percent. This may be attributed to dissolution of the drug in solvent or aqueous solution used. Also, increasing drug-to-polymer ratios are associated with decreasing particle size.[16]
Creation of an optimal formulation also depends on stirring rate, which is shown to influence particle size, size distribution, and subsequent drug release. The release mechanism of the active ingredient can be pressure-dependant, temperature-dependant, pH-dependant, or solubility-dependent.[15] In-vitro, eight-hour, release studies of 2.5%, 5%, and 10% BPO microsphere formulations indicated that the cumulative amount of drug present in the final formulation increased as drug concentration increased. At all concentrations, rate of drug release during the first hour was higher than the rate of release in the second hour. Flux remained constant for the last seven hours. This higher initial rate of drug release may be due to nonencapsulated active drug in the formulation. The constant flux observed during the next seven hours is attributed to the release of encapsulated drug.[16]
Microsphere technologies differ from microencapsulation and liposome technologies (Table 1). Microencapsulation involves the capture of drug within complete capsules that, upon application, rupture and disperse 100 percent of the active drug contained inside. Liposomes, by comparison to microspheres, tend to provide a relatively low rate of entrapment efficiency (approximately 30%). Microsponge technology does not require preservatives, whereas liposome technology does for microbiological stability. Liposomes also need ultrapure raw materials for quality control, which makes them more expensive, unlike microsponge technology.[15]
{kind=link}
Tretinoin Microsphere Formulations
Microsphere delivery formulations of tretinoin reached the market more than a decade ago with a significantly improved tolerability profile relative to standard formulations. In a study comparing the efficacy and tolerability of tretinoin 0.1% microsphere cream to that of adapalene 0.1% gel, tretinoin had increased dryness and peeling, but the incidence of erythema, burning/stinging, and itching was similar in both groups.[17] With a newer tretinoin 0.04% microsphere formulation, data show that cumulative irritancy was either similar to or lower than that associated with adapalene.[18]
Compared to tretinoin microsphere gel 0.1%, tretinoin microsphere gel 0.04% was associated with fewer patient reports of dryness during the early phase of treatment, while overall tolerability, as measured by incidence of peeling, burning/stinging, and itching, was similar between the two groups; the incidence of erythema was reduced in the tretinoin group.[19] Another study compared tretinoin microsphere gel 0.04% to tretinoin 0.025% cream in subjects with healthy skin. Subjects in the investigator-blind, evaluator-blind, randomized trial applied the topical medications in a split-face fashion for two weeks. There was no significant difference in tolerability between the two arms despite the fact that microsphere formulation had the higher tretinoin concentration, as indicated by measures of erythema, skin dryness, itching, and stinging.[18]
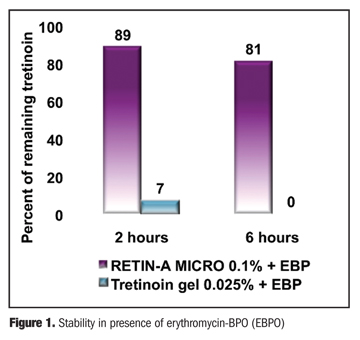
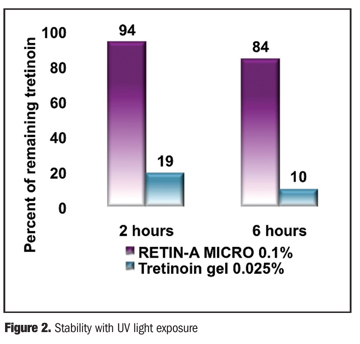
In addition to enhanced tolerability, microsphere formulations provide the benefit of improved drug stability.[20,21] Tretinoin has been shown to degrade significantly upon exposure to ultraviolet (UV) radiation as well as when combined with BPO. However, when microsphere-encapsulated tretinoin was exposed to UV and BPO, it was only minimally degraded. At two and six hours after exposure to UV radiation, 89 and 81 percent of the initial tretinoin remained stable, respectively. At two and six hours after being combined with clindamycin/BPO, 86 and 80 percent of the tretinoin remained stable, respectively (Figure 1). By contrast, for the tretinoin not in microspheres, just 19 and 10 percent of the UV-exposed tretinoin remained unchanged and 7 and 0 percent of the BPO-exposed tretinoin, remained, respectively, at two and six hours.[21] (Figure 2) These findings have been confirmed in vivo. A recent study shows that patients who cleansed the face with a BPO 5% wash each morning followed by topical tretinoin gel microsphere 0.04% had a response similar to that seen in individuals who used the same wash each morning and tretinoin microsphere gel together each evening.[22] Patients (n=247) 12 years of age or older participated in the 12-week study. These findings suggest that tretinoin was not degraded by BPO. The once-daily regimen was well tolerated and may be associated with better adherence than the two-times-a-day regimen.
{kind=link}
{kind=link}
Of note, treatment with topical tretinoin microsphere 0.1% gel is associated with a more significant reduction in facial shine, a common concern among acne patients. For the single-center, double-blind, split-face study, 35 subjects (ages 12–24 years) with moderate acne vulgaris and moderate facial oiliness, applied assigned medications for four consecutive days. At three hours after the final application, patients rated the reduction in facial “shine” as significantly greater on the sides treated with tretinoin gel microsphere 0.1% versus tretinoin cream 0.05%. Similarly, investigators noted significantly reduced facial shine at three and six hours post-treatment. Photographic analyses also showed that, while both treatments produced reductions in facial shine, decreases were greater on tretinoin gel microsphere 0.1%-treated sides.[23]
Benzoyl Peroxide Microsphere Formulations
As noted, BPO, which has been used in the topical treatment of acne for more than 60 years, has re-emerged as a key component of effective topical acne therapy because it is not associated with the development of P. acnes resistance. Also, recent research suggests that high concentrations of BPO may not be necessary for better therapeutic outcomes. In fact, at 2.5, 5, and 10% concentrations, BPO had equivalent efficacy in inflammatory acne. However, higher concentrations were associated with increasing incidence of adverse effects.[24]
The use of microsphere delivery of BPO has been associated with improved tolerability and good efficacy. In-vivo human studies have shown that entrapped BPO significantly reduced counts of P. acnes (p<0.001) and aerobic bacteria (p<0.001) and the free fatty acid/triglyceride ratio in skin lipids.[25] Controlled laboratory studies comparing various investigational formulations of BPO showed that topicals containing plain BPO particles had the highest release rates while BPO microspheres provided a low and consistent drug delivery.[26]
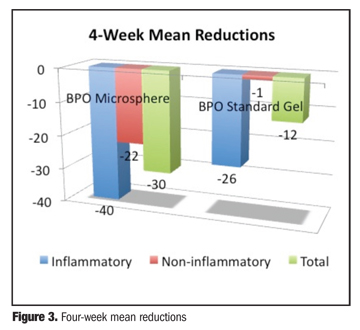
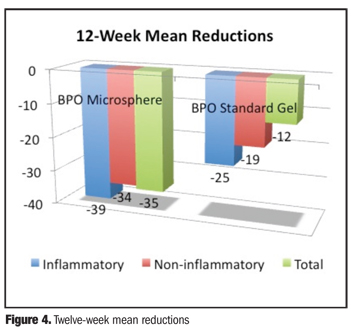
In a series of cases recently published, BPO microsphere gel was associated with favorable efficacy and a very low potential for irritation.[27] An investigator-blinded, randomized, multicenter, 12-week study involving 48 subjects age 12 and older with mild-to-moderate facial acne vulgaris compared BPO microsphere cream 5.5% twice daily to BPO gel 6% twice daily.[28] By Week 4, both the BPO microsphere cream 5.5% and BPO gel 6% groups demonstrated statistically significant mean percent reductions in inflammatory and total lesions (P<0.05) compared to baseline. BPO microsphere cream 5.5% showed a significant mean reduction in noninflammatory lesions, but BPO gel 6% did not. BPO microsphere 5.5% cream provided a greater, though not statistically significant, reduction in inflammatory, noninflammatory, and total lesions at both Week 4 (Figure 3) and Week 12 (Figure 4). Complete clearance or marked improvement of acne was observed by the investigators in 33 percent of subjects treated with BPO microsphere cream 5.5% and 16 percent of subjects treated with BPO gel 6% at Week 12.
{kind=link}
{kind=link}
Tolerability scores were significantly better for BPO microsphere cream 5.5% than for standard BPO gel 6%. In the BPO gel 6% group, there was a 79-percent incidence of skin tolerability reactions—stinging (22%), itching (26%), scaling (9%), dryness (13%), and erythema (9%). By contrast, the incidence of skin tolerability reactions was 37 percent in the BPO microsphere cream 5.5% group. These included stinging (4%), scaling (29%), and dryness (4%). One subject withdrew from the trial due to skin irritation after four days of application of BPO gel 6%.
Microsphere delivery can also be incorporated into wash formulations. In a study comparing BPO microsphere 5.5% wash to a gentle nonmedicated cleanser once daily in patients age 12 or older, tolerability as rated by investigators and subjects was very good for both products. BPO microsphere 5.5% wash tended to be associated with lower but not statistically significant ratings for erythema, dryness, and scaling as rated by investigators at Day 14 and Day 21. Basically, BPO microsphere 5.5% wash was as tolerable as a gentle nonmedicated cleanser.[29]
As in the case of tretinoin microsponges, BPO microsponges appear to reduce sebum accumulation and associated facial shine. In one split-face trial, subjects cleansed the face with a gentle skin cleanser, then applied BPO microsphere cream 5.5% to one half of the face and no product to the control side. Measurements were taken with a sebumeter at baseline and 30 minutes, two hours, four hours, and six hours after the regimen. Actively treated sides had greater surface sebum reduction at all timepoints.[30]
Conclusion
Although topical drug therapy is associated with benefits, such as reduced risk of systemic side effects, certain drugs have a tendency to induce local irritation. Novel formulations have attempted to improve tolerability through various means, including the avoidance of irritating excipients, the incorporation of moisturizing ingredients into the vehicle base, and the use of controlled-release microsphere delivery.
By facilitating controlled-release delivery of potentially irritating drugs, topical microspheres are associated with improved therapeutic outcomes and minimal irritation. Microsphere formulations of topical tretinoin and BPO currently on the market have demonstrated good efficacy and tolerability and are expected to encourage adherence and long-term therapeutic benefit. Microsphere encapsulation protects the stability of drugs; it makes tretinoin photostable and enables the use of convenient topical combination regimens with BPO. Furthermore, microspheres appear to absorb sebum from the skin’s surface, reducing oiliness, which is a common complaint among acne patients. This apparent effect is not shown to increase the incidence of skin dryness or irritation, which are consistently rated as lower with microsphere formulations compared to standard formulations. Studies and clinical experience confirm the efficacy and improved tolerability of topical tretinoin and BPO microsphere formulations. Microsponge technology can be used with any topical treatment and should be more widely available, especially with potentially irritating molecules.
References
1. Goodman G. Acne and acne scarring—the case for active and early intervention. Aust Fam Physician. 2006;35(7):503–504.
2. Tristani-Firouzi P, Krueger GG. Efficacy and safety of treatment modalities for psoriasis. Cutis. 1998;61(2 Suppl):11–21.
3. Feldman SR. Approaching psoriasis differently: patient-physician relationships, patient education and choosing the right topical vehicle. J Drugs Dermatol. 2010;9(8):908–911.
4. Richards HL, Fortune DG, Griffiths CE. Adherence to treatment in patients with psoriasis. J Eur Acad Dermatol Venereol. 2006;20(4):370–379.
5. Lee IA, Maibach HI. Pharmionics in dermatology: a review of topical medication adherence. Am J Clin Dermatol. 2006;7:231–236.
6. Zaenglein AL. Making the case for early treatment of acne. Clin Pediatr (Phila). 2010;49(1):54–59.
7. Balkrishnan R, Kulkarni AS, Cayce K, Feldman SR. Predictors of healthcare outcomes and costs related to medication use in patients with acne in the United States. Cutis. 2006;77(4):251–255.
8. Kircik, LH, Bikowski JB, Cohen DE, et al. Vehicles matter, Vol 1. Practical Dermatology. 2010;7(6 Suppl):1–16.
9. Gollnick H, Cunliffe W, Berson D, et al, Global Alliance to Improve Outcomes in Acne. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49(1 Suppl):S1–S37.
10. Thiboutot D, Gollnick H, Bettoli V, et al, Global Alliance to Improve Outcomes in Acne. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60(5 Suppl):S1–S50.
11. Ghali F, Kang S, Leyden J, et al. Changing the face of acne therapy. Cutis. 2009;83(2 Suppl):4–15.
12. Del Rosso JQ. Selection of therapy for acne vulgaris: balancing concerns about antibiotic resistance. Cutis. 2008;82(5 Suppl):12–16.
13. Dréno B, Thiboutot D, Gollnick H, et al, Global Alliance to Improve Outcomes in Acne. Large-scale worldwide observational study of adherence with acne therapy. Int J Dermatol. 2010;49(4):448–456.
14. Embil K, Nacht S. The Microsponge Delivery System (MDS): a topical delivery system with reduced irritancy incorporating multiple triggering mechanisms for the release of actives. J Microencapsul. 1996;13(5):575–588.
15. Chadawar V, Shaji J. Microsponge delivery system. Curr Drug Deliv. 2007;4(2):123–129.
16. Jelvehgari M, Siahi-Shadbad MR, Azarmi S, Martin GP, Nokhodchi A. The microsponge delivery system of benzoyl peroxide: preparation, characterization and release studies. Int J Pharm. 2006;308(1-2):124–32.
17. Nyirady J, Grossman RM, Nighland M, et al. A comparative trial of two retinoids commonly used in the treatment of acne vulgaris. J Dermatolog Treat. 2001;12(3):149–157.
18. Leyden JJ, Grossman R, Nighland M. Cumulative irritation potential of topical retinoid formulations. J Drugs Dermatol. 2008;7(8 Suppl):S14–S18.
19. Berger R, Rizer R, Barba A, et al. Tretinoin gel microspheres 0.04% versus 0.1% in adolescents and adults with mild to moderate acne vulgaris: a 12-week, multicenter, randomized, double-blind, parallel-group, phase IV trial. Clin Ther. 2007;29(6):1086–1097.
20. Nyirady J, Lucas C, Yusuf M, Mignone P, Wisniewski S. The stability of tretinoin in tretinoin gel microsphere 0.1%. Cutis. 2002;70(5):295–298.
21. Nighland M, Yusuf M, Wisniewski S, Huddleston K, Nyirady J. The effect of simulated solar UV irradiation on tretinoin in tretinoin gel microsphere 0.1% and tretinoin gel 0.025%. Cutis. 2006;77(5):313–316.
22. Pariser D, Bucko A, Fried R, et al. Tretinoin gel microsphere pump 0.04% plus 5% benzoyl peroxide wash for treatment of acne vulgaris: morning/morning regimen is as effective and safe as morning/evening regimen. J Drugs Dermatol. 2010;9(7):805–813.
23. Nyirady J, Nighland M, Payonk G, et al. A comparative evaluation of tretinoin gel microsphere, 0.1%, versus tretinoin cream, 0.025%, in reducing facial shine. Cutis. 2000;66(2):153–156.
24. Fakhouri T, Yentzer BA, Feldman SR. Advancement in benzoyl peroxide-based acne treatment: methods to increase both efficacy and tolerability. J Drugs Dermatol. 2009;8(7):657–661.
25. Wester RC, Patel R, Nacht S, et al. Controlled release of benzoyl peroxide from a porous microsphere polymeric system can reduce topical irritancy. J Am Acad Dermatol. 1991;24(5 Pt 1):720–726.
26. Nokhodchi A, Jelvehgari M, Siahi MR, Mozafari MR. Factors affecting the morphology of benzoyl peroxide microsponges. Micron. 2007;38(8):834–840.
27. Bikowski J, Del Rosso JQ. Benzoyl peroxide microsphere cream as monotherapy and combination treatment of acne. J Drugs Dermatol. 2008;7(6):590–595.
28. Smith SR, Kempers S. A study of 5.5% benzoyl peroxide microsphere cream versus 6% benzoyl peroxide gel in the treatment of acne vulgaris. Cosmet Dermatol. 2006;19:537–542.
29. Del Rosso JQ, Kircik L. Comparison of the tolerability of benzoyl peroxide microsphere cream wash versus gentle cleanser when used in combination with clindamycin and tretinoin gel: a multicenter, investigator-blind, randomized study. Poster presented at: American Academy of Dermatology 67th Annual Meeting; San Francisco, California; March 6–10, 2009.
30. Del Rosso JQ. Benzoyl peroxide formulations: what is the science supporting microsphere vehicle technology and clinical use. J Clin Aesthet Dermatol. 2009;2(9):46–54.