Jason J. Emer, MD; The Mount Sinai School of Medicine, Department of Dermatology, New York, New York
Abstract
Anti-tumor necrosis factor therapy has shown remarkable safety and efficacy in the treatment of many autoimmune and inflammatory disorders, although limited published data exists regarding these treatments in patients with concomitant human immunodeficiency virus and/or acquired immune deficiency syndrome. The use of tumor necrosis factor inhibition is associated with an increased risk of severe infections, including tuberculosis and risk of worsening hepatitis B virus, but its effect on viral infections is conflicting. Currently, package inserts for the three anti-tumor necrosis factor medications (infliximab, etanercept, and adalimumab) affirm that caution should be exercised when considering their use in patients with chronic infection or a history of recurrent infection, as clinical trials for these medications have historically excluded patients with chronic viral infections. With the increasing prevalence of chronic viral infections in patients who are candidates for anti-tumor necrosis factor therapy, there is reason for additional research to assess the safety, efficacy, and potential role of tumor necrosis factor inhibition in this population. This article is an up-to-date review of the emerging use of biologic therapies in patients infected with the human immunodeficiency virus and concurrent psoriatic or rheumatological disease.
(J Clin Aesthetic Dermatol. 2009;2(4):29–35)
***********************************************************************************************************************************
Retroviruses were first implicated in psoriasis more than 20 years ago,[1] followed by the observation that psoriasis may appear for the first time or pre-existing psoriasis may worsen and be difficult to control in patients with human immunodeficiency virus (HIV) infection.[2] There is a paradoxical exacerbation of psoriasis, a T-cell mediated disease, in patients with HIV in which circulating CD4+ T-cells are depleted that has not been fully understood.[3] Reports have described patients with HIV whose psoriasis resolved after combination antiretroviral therapy[4–7] and in which disease worsened after stopping retroviral treatment,[8] implicating a direct role for HIV in disease exacerbation. Often, patients with psoriasis and HIV have more severe disease that is refractory to multiple therapies and have a higher prevalence of associated rheumatological syndromes or psoriatic arthritis.[9,10] Psoriasis in HIV has a more sudden onset with a higher frequency of severe pustular or guttate forms.[11] Joint involvement is more aggressive and more prevalent with associated severe nail dystrophy and palmoplantar keratoderma.[12]
Tumor necrosis factor and HIV infection
An over-expression of serum tumor necrosis factor (TNF) has been shown in all stages of HIV infection, with the highest level of expression detected in concomitant opportunistic infections such as tuberculosis (TB).[13,14] HIV infection induces TNF expression in culture, and exogenous TNF enhances HIV expression possibly through the actions of nuclear factor (NF)-kB.[15] Elevated serum TNF levels have been linked with increased viral replication and subsequent increased viral load, depletion of CD4+ T-cells, and clinical signs and symptoms of worsening HIV infection, such as fever, cachexia, aphthous ulcers, fatigue, and dementia.[16,17] Both thalidomide and pentoxifylline (weak TNF inhibitors) have been shown to reduce viral load when administered to asymptomatic HIV-infected patients and to those with active TB infections. Treatment with thalidomide was shown to lower serum TNF levels, but treatment with pentoxifylline was not.[18,19] In a randomized, controlled trial in patients with HIV and aphthous ulcers, thalidomide was associated with dramatic oral healing, but serum TNF levels did not decline or correlate with this clinical finding.[20] In-vitro studies with a small-molecule inhibitor of TNF (LMP-420) showed that inhibition of TNF transcription and subsequent biosynthesis can inhibit the replication of HIV-1 in primary cultures of human cells.[21] Theoretically, there appears to be a favorable effect of anti-TNF therapy in patients with HIV.
Anti-TNF Therapy
With the introduction of biological agents in recent years, an increasing patient number is being treated with anti-TNF therapy for various autoimmune and inflammatory conditions. Progressively more patients have concurrent viral infections, such as HIV, hepatitis B virus (HBV), and hepatitis C virus (HCV). While some dermatologists believe this brings new hope in the treatment of various conditions, such as psoriasis, psoriatic arthritis, Crohn’s disease, Reiter’s disease, and rheumatoid arthritis in patients with concurrent viral infections, others are concerned of the increased risks associated without controlled clinical trials to verify safety and efficacy and to help guide treatment and laboratory monitoring.[22]
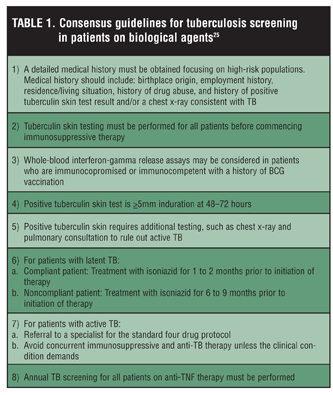
Screening for TB. Consensus agrees that exclusion of any bacterial infections and screening for TB is mandatory before initiating therapy with anti-TNF medications. Most cases of reported TB infection are of infliximab-associated TB, although disseminated TB has been seen in all three anti-TNF agents.[23] Perlmutter et al[24] recently reported three cases of TB induced by anti-TNF therapy despite a rigorous screening policy. After intense literature review, their suggested guidelines for TB screening prior to anti-TNF thrapy included the standard tuberculin skin and chest x-ray testing as well as the newer, alternative option—the QuantiFERON®-TB Gold test (QFT-G; Cellestis Inc., Valencia, California). For those with positive tuberculin screening tests, they recommended referral to a pulmonologist to rule out active disease and possible initiation of anti-TB therapy. For those with latent TB and concurrent immunosuppression, they recommend at least four weeks of isoniazid therapy prior to initiation of anti-TNF therapy and up to 12 weeks of therapy for those starting infliximab. For those with latent TB without concurrent immunosuppression, they recommend a complete course of nine months of isoniazid therapy before initiating anti-TNF therapy. Yearly TB screening for all patients on biological therapies and referral to a specialist if seroconversion occurs during therapy was also recommended. Further, Doherty et al[25] recently published a consensus statement with recommendations for TB screening of psoriasis patients being treated with biological agents (Table 1). No clear recommendations were made on which particular anti-TNF agent should be used in the setting of latent TB.
{kind=link}
Screening for chronic viral infections. There are few guidelines on whether or not to screen for or treat chronic viral infections, such as HIV, HBV, and HCV, prior to initiation of a biological agent.26 Many have suggested that in viral hepatitis, TNF inhibits viral replication and stimulates T-cell mediated cell responses to clear virus from infected hepatocyte cells. As a result, TNF inhibition might be expected to encourage viral replication by allowing the evasion of host defense mechanisms. Others contribute cytokines, such as TNF, to liver injury, hepatocyte apoptosis, and the pathogenesis of liver fibrosis.[27,28] To date, only a few case reports and small studies have been published regarding the safety and efficacy of anti-TNF therapy in patients with chronic viral infections with varying results. Most reports indicate that there is a risk of reactivating HBV infection and that use in HCV infection may be safe and beneficial.[29,30] It is known that patients with HIV are often co-infected with HBV or HCV, which raises concerns about the long-term safety of anti-TNF therapy in this population.[31,32] HIV has been shown to modify the natural history of HCV with an unusually rapid progression to cirrhosis with severe HCV viremia and liver damage.[33]
Nathan et al[34] formulated clinical guidelines for the treatment of patients with biological agents who are infected with HBV and HCV. Their recommendations included screening all patients for HBV and HCV prior to treatment with any biological agent, but the presence of HBV or HCV should not preclude therapy at least with infliximab. Further, they explained there is no evidence that anti-TNF therapies accelerate the course of HCV and that ongoing monitoring of disease activity and consideration of liver biopsy is therefore recommended in HCV-positive patients receiving long-term anti-TNF therapy. Those patients with HBV infection could have preventative treatment with antiviral therapy and/or frequent monitoring of HBV DNA levels and liver enzymes throughout and after treatment.
Hepatitis C Virus and Anti-TNF Therapy
Domm et al[29] recently published a literature review on the impact of anti-TNF antagonist treatment in chronic viral infections. For treatment of patients with HCV, etanercept was safe and not associated with any serious toxic effects, supported by evidence from a number of case reports and a Phase 2, double-blind, placebo-controlled trial by Zein et al[35] where etanercept was tested as additional therapy with ribavirin and interferon. For treatment with infliximab, it was concluded that patients with signs and symptoms of liver dysfunction (elevated liver enzymes) should be evaluated for the presence of liver injury and should discontinue treatment if jaundice and/or marked liver enzyme elevations (greater than 5 times the upper limit of normal) develop. The overall conclusion was that for carefully selected patients, anti-TNF therapy in the setting of HCV was well tolerated without any apparent influence on the underlying viral infection and all anti-TNF therapies (specifically infliximab and adalimumab) should be administered with caution. Frequent interval monitoring of serum aminotransferases and HCV viral load were recommended.
Hepatitis B Virus and Anti-TNF Therapy
For the treatment of HBV, both treatments with infliximab and etanercept showed cases of fulminant HBV reactivation. The majority of cases were reported after infliximab use, most likely secondary to the difference in pharmacological and biochemical actions of the monoclonal antibody (infliximab) functioning to neutralize soluble and transmembrane-bound TNF as compared to the fusion protein (etanercept) that can only bind soluble TNF. Any HBV reactivation was treated successfully with lamivudine therapy, thus it was concluded that physicians should consider antiviral therapy in patients with HBV (with or without active viral replication) and initiated treatment should continue for 3 to 6 months after stopping anti-TNF therapy.
HIV and Anti-TNF Therapy
Overall, rigorous screening methods should be commenced when considering the treatment of any patient with a biological agent, especially those with concurrent chronic viral disease, such as HIV, HBV, or HCV. No current guidelines exist regarding the screening and monitoring of patients with HIV who are on biological therapies. Currently, a regimen with minimal complications, such as topical therapy and phototherapy is considered first line in patients with HIV and psoriasis.[10,36–40] The use of phototherapy is widely accepted for the treatment of psoriasis associated with HIV infection and for other HIV-associated skin diseases, such as pruritus and eosinophilic folliculitis.[41] Regimens using ultraviolet light B (UVB) or psoralens plus UVA (PUVA) have been recommended for HIV patients with psoriasis.42 Often, physicians select phototherapy alone or in combination with an oral retinoid as a treatment of choice for moderate-to-severe psoriasis even though phototherapy in large, accumulated doses has been shown to increase the viral load in patients who are not on antiretroviral therapy.[43]
Most clinicians avoid the use of systemic treatments, such as methotrexate or cyclosporine, because of the theoretical increased risk of immunosuppression and threat of favoring viral replication and progression of the underlying viral disease. Even so, some speculate that these systemic therapies can be given without increasing the risk of adverse events.[44–51] The ability of cyclosporine to lower the CD4+ T-cell counts has been described,[52] although other studies have been published on the use of cyclosporine on the early stages of HIV infection with encouraging results.[44,53] Acitretin may be the safest oral agent for systemic therapy in patients with HIV, as it is not immunosuppressive and has been used successfully in HIV-associated Reiter’s syndrome and psoriasis.[54,55] Although generally well tolerated, retinoids have a negative effect on the lipid profile, which may become a contraindication or cause for suspension of treatment. Further, infectious and neoplastic complications, alcohol and other drug abuse, and associations with other chronic viral infections, such as HBV and HCV, occur with greater frequency in patients with HIV, limiting the use of various immunosuppressants in this population. The most recent studies have demonstrated that long-term use of methotrexate is safe and efficacious in patients infected with HIV.[50]
Biological therapies may offer another option in the armamentarium of therapeutic options for patients with concomitant HIV and autoimmune or inflammatory conditions, such as psoriasis or psoriatic arthritis. The experience of some physicians suggest that these therapies do not significantly increase rates of morbidity and mortality,[56] nor do they have a negative effect on the CD4+ T-cell count or viral load.[57] Biological therapy decreases host defenses against infection, the impact of which has not been elucidated in patients with a concomitant immunosuppressive disease such as HIV since controlled clinical trials have historically excluded this patient population. The majority of reports leading to serious adverse events has occurred in patients concurrently receiving other medications that suppress the immune system, such as patients with rheumatic disease being treated with a combinational therapy consisting of a biologic medication and oral prednisone, methotrexate, sulfasalazine, leflunomide, or mycophenolate mofetil.
Etanercept and Infliximab in Patients with HIV
Multiple case reports have documented the use of etanercept and infliximab in patients with HIV, the majority of which have indicated that the administration of biologic therapy does not appear to increase morbidity or mortality rates.[56] Some studies have shown that anti-TNF therapy may improve the symptoms of HIV-associated fatigue, fever, aphthous ulcers, cachexia, and dementia, as well as help manage rheumatic and psoriatic disease. Initial concerns were over the theoretical risk that immunosuppressive medications increased the risk of opportunistic infections, sepsis, and progression of HIV disease. However, this risk has been primarily seen in patients treated concurrently with other immunosuppressive medications who had uncontrolled HIV and/or AIDS (i.e., CD4+ T-cell count < 200 cells/mm3 and viral load > 60,000 copies/mm3) or who were not on highly active antiretroviral therapy (HAART) when indicated. Nonetheless, caution should be advised, as a HIV-negative patient treated with infliximab and cyclophosphamide for rheumatoid arthritis developed a reduction of CD4+ T-cells during treatment.[58]
Etanercept. To date, the use of etanercept in patients with HIV has been studied in three clinical studies[59–61] and documented in four case reports.[62–65] In all cases, the HIV patients were treated with anti-TNF therapy for refractory rheumatic disease. In the majority of cases, the therapy was well tolerated and absolute CD4+ T-cell count and HIV viral load were monitored frequently. Few patients reported any clinical deterioration or disease progression related to HIV. No opportunistic infections, including active TB, or malignancies were observed unless the patient was on concomitant immunosuppressive therapy for rheumatic disease or had uncontrolled HIV.
One case reported on a 45-year-old man with extensive psoriasis and psoriatic arthritis who had failed several disease-modifying medications (corticosteroids, hydroxychloroquine, and minocycline) and was started on etanercept 25mg subcutaneous twice weekly for severe unremitting disease. Within three weeks, his psoriasis had dramatically improved and his joint inflammation had stabilized. His immunologic and viral parameters remained stable for four months, but his clinical course was complicated by frequent polymicrobial infections. Etanercept was discontinued despite continued improvements in his psoriasis, psoriatic arthritis, and functional status. He later died due to respiratory arrest during a hospitalization for recalcitrant pseudomonal knee infections.[63]
In a Phase 1 study by Wallis et al,[60] 16 patients with HIV-associated TB were treated with etanercept 25mg subcutaneous twice weekly for four weeks in addition to the standard TB therapy and co-trimoxazole to prevent opportunistic infections. Adjunctive treatment with etanercept did not interfere with the response to treatment for pulmonary TB and a trend toward an even superior response to TB treatment was shown. HIV infection did not appear to be impaired by the anti-TNF treatment, as no effect was shown on the viral load and improvement was modestly seen in CD4+ T-cell counts. The authors concluded that etanercept may be safely administered during the initial treatment of pulmonary TB in HIV-infected patients, although caution must be taken when considering the use of a biologic agent in the setting of HIV. The author’s rationale was that excessive serum TNF in TB accompanying HIV infection is responsible for many of the clinical manifestations seen in the setting of accelerated CD+ T-cell count decline.
The first case of a patient co-infected with HIV and HCV treated with etanercept was recently reported. The 42-year-old hemophiliac suffered from severe psoriatic arthritis associated with psoriatic skin lesions that did not respond to a combination of methotrexate and cyclosporine. Treatment with etanercept 25mg subcutaneous twice weekly achieved remission of the skin and joint symptoms. The patient’s clinical improvement was constant during the two-year follow up, and no serious infections or other side effects had occurred. HCV and HIV status remained stable, with all viral parameters within the normal range.[64]
With regard to the use of etanercept in patients with HIV, although the safety and efficacy has not been fully evaluated, it seems reasonable based on case reports that the use of biologic therapy may be considered in patients with HIV. A recent review of the use of etanercept in psoriasis and psoriatic arthritis concluded that it is an effective and safe treatment for patients infected with HIV or HCV.[66,67]
Strict guidelines may be required for patient safety, as most of these studies imply that there is an increased risk of infection in patients who are on other simultaneous immunosuppressive therapies or who have uncontrolled immunologic and viral parameters. Stringent caution should be exercised, and clinical studies will need to be performed to further elucidate this issue.
Infliximab. All controlled trials using infliximab as therapy have excluded patients with HIV. Two retrospective studies,[68,69] one open-label trial,[70] and six case reports[71–76] have been published with regard to the use of infliximab in HIV-positive patients. In all cases, immunologic and viral parameters were monitored and the majority of the patients had failed other immunosuppressive medications treating a rheumatologic disease prior to the use of biologic therapy. Overall, the conclusions were that infliximab was safe and effective when used in HIV patients with a normal CD4+ T-cell count (>200 cells/mm3) and viral load (<60,000 copies/mm3) prior to therapy and who were not on any other concurrent immunosuppressive treatment. No changes were observed in CD4+ T-cell counts or HIV viral loads, and for the majority of cases, the antiretroviral medication remained unchanged even after the initiation of infliximab therapy. The vast conclusions were that further studies are needed to elucidate the efficacy and safety of infliximab for the treatment of rheumatologic disorders in patients with HIV.
Bartke et al[73] treated a 46-year-old patient with worsening psoriasis and psoriatic arthritis after beginning HAART therapy for HIV infection. The patient’s psoriatic flare was uncontrolled despite treatment with acitretin, prednisone, methotrexate, phototherapy, topical corticosteroids, and tazarotene. Treatment was initiated with infliximab at a dose of 3mg/kg and rapid improvement was seen. The patient’s viral load remained undetectable and the CD4+ T-cell count increased.
Sellam et al[75] used infliximab to treat two HIV patients with severe psoriasis and psoriatic arthritis refractory to methotrexate and corticosteroids. One patient was highly immunocompromised with a CD4+ T-cell count of 16 cells/mm3 and a viral load of 300,000 copies/mm3 at the initiation of infliximab therapy. It was necessary to change the HAART therapy on multiple occasions due to side effects and increased viral load. After four years of infliximab and concurrent methotrexate therapy, the patient achieved a viral load of 5,900 copies/mm3 and CD4+ T-cell count of 233 cells/mm3. Both patients had considerable joint and skin improvement with no infectious or neoplastic complications.
Gaylis[72] treated a 41-year-old man with HIV and severe Reiter’s disease refractory to combinational treatment with corticosteroids and methotrexate. While on HAART therapy, the patient reported a viral load of less than 500 copies/mm3 and CD4+ T-cell count of 770 cells/mm3. Infliximab was started at 3mg/kg, methotrexate was maintained, and the corticosteroids were tapered. The patient noted dramatic improvement in the joints and skin after initiation of infliximab therapy. After six months of treatment, the patient had a viral load of 400 copies/mm3 and CD4+ T-cell count of 814 cells/mm3. No side effects were noted over 18 months of therapy.
Adalimumab in Patients with HIV
Adalimumab is another monoclonal anti-TNF antibody with similar clinical profile to infliximab. Only one retrospective series has highlighted the use of adalimumab in patients with HIV and refractory rheumatic disease.[62] It was noted that adalimumab was well tolerated without any adverse effects on CD4+ T-cell count and HIV viral load. The authors concluded that anti-TNF agents may be given if the patient’s underlying HIV infection is well controlled and the patient is not severely immunocompromised.
Conclusion
Although the use of anti-TNF medications in HIV infection has been minimally described in the literature, the data speculates that there may be a role for anti-TNF therapy in patients with HIV and concomitant psoriasis and/or rheumatic disease. Based on the available knowledge that therapy with anti-TNF medications in HIV-infected patients does not appear to increase morbidity and mortality, it is realistic that more controlled, clinical studies are needed to assess the safety and efficacy of this treatment option in patients who have HIV and possibly other chronic viral diseases, such as HBV and HCV. TNF inhibition in HIV should be reserved for highly selected patients who have failed other treatment options and are well controlled under antiretroviral therapy until the potential for long-term effects, such as opportunistic infections, malignancies, and loss of HIV control, have been more clearly determined.
References
1. Rodahl E. Retroviruses and chronic arthritis. Possible significance of some recent observations. Scand J Rheumatol. 1989;18(6):335–339.
2. Duvic M, Johnson TM, Rapini RP, et al. Acquired immunodeficiency syndrome-associated psoriasis and Reiter’s syndrome. Arch Dermatol. 1987;123(12):1622–1632.
3. Namazi MR. Paradoxical exacerbation of psoriasis in AIDS: proposed explanations including the potential roles of substance P and gram-negative bacteria. Autoimmunity. 2004;37(1):67–71.
4. Vittorio Luigi De Socio G, Simonetti S, Stagni G. Clinical improvement of psoriasis in an AIDS patient effectively treated with combination antiretroviral therapy. Scand J Infect Dis. 2006;38(1):74–75.
5. Buchness MR. Treatment of skin diseases in HIV-infected patients. Dermatol Clin. 1995;13(1):231–238.
6. Duvic M, Crane MM, Conant M, et al. Zidovudine improves psoriasis in human immunodeficiency virus-positive males. Arch Dermatol. 1994;130(4):447–451.
7. Obuch ML, Maurer TA, Becker B, Berger TG. Psoriasis and human immunodeficiency virus infection. J Am Acad Dermatol. 1992;27(5 Pt 1):667–673.
8. Vano-Galvan S, Jaen P. Severe psoriasis due to cessation of antiretroviral therapy in a patient with human immunodeficiency virus. Isr Med Assoc J. 2008;10(7):557–558.
9. Mallon E, Bunker CB. HIV-associated psoriasis. AIDS Patient Care STDS. 2000;14(5):239–246.
10. Mamkin I, Mamkin A, Ramanan SV. HIV-associated psoriasis. Lancet Infect Dis. 2007;7(7):496.
11. Leal L, Ribera M, Daudén E. Psoriasis and HIV infection. Actas Dermosifiliogr. 2008;99(10):753–763.
12. Cuellar ML, Espinoza LR. Rheumatic manifestations of HIV-AIDS. Baillieres Best Pract Res Clin Rheumatol. 2000;14(3):579–593.
13. Aukrust P, Liabakk NB, Müller F, et al. Serum levels of tumor necrosis factor-alpha (TNF alpha) and soluble TNF receptors in human immunodeficiency virus type 1 infection–correlations to clinical, immunologic, and virologic parameters. J Infect Dis. 1994;169(2):420–424.
14. Whalen C, Horsburgh CR, Hom D, et al. Accelerated course of human immunodeficiency virus infection after tuberculosis. Am J Respir Crit Care Med. 1995;151(1):129–135.
15. Duh EJ, Maury WJ, Folks TM, et al. Tumor necrosis factor alpha activates human immunodeficiency virus type 1 through induction of nuclear factor binding to the NF-kappa B sites in the long terminal repeat. Proc Natl Acad Sci U S A. 1989;86(15):5974–5978.
16. Dezube BJ, Lederman MM, Chapman B, et al. The effect of tenidap on cytokines, acute-phase proteins, and virus load in human immunodeficiency virus (HIV)-infected patients: correlation between plasma HIV-1 RNA and proinflammatory cytokine levels. J Infect Dis. 1997;176(3):807–810.
17. Valdez H, Lederman MM. Cytokines and cytokine therapies in HIV infection. AIDS Clin Rev. 1997–1998:187–228.
18. Marriott JB, Cookson S, Carlin E, et al. A double-blind placebo-controlled phase II trial of thalidomide in asymptomatic HIV-positive patients: clinical tolerance and effect on activation markers and cytokines. AIDS Res Hum Retroviruses. 1997;13(18):1625–1631.
19. Wallis RS, Nsubuga P, Whalen C, et al. Pentoxifylline therapy in human immunodeficiency virus-seropositive persons with tuberculosis: a randomized, controlled trial. J Infect Dis. 1996;174(4):727–733.
20. Jacobson JM, Greenspan JS, Spritzler J, et al. Thalidomide for the treatment of oral aphthous ulcers in patients with human immunodeficiency virus infection. National Institute of Allergy and Infectious Diseases AIDS Clinical Trials Group. N Engl J Med. 1997;336(21):1487–1493.
21. Haraguchi S, Day NK, Kamchaisatian W, et al. LMP-420, a small-molecule inhibitor of TNF-alpha, reduces replication of HIV-1 and Mycobacterium tuberculosis in human cells. AIDS Res Ther. 2006 Mar 31;3:8.
22. Desai SB, Furst DE. Problems encountered during anti-tumour necrosis factor therapy. Best Pract Res Clin Rheumatol. 2006;20(4):757–790.
23. Ellerin T, Rubin RH, Weinblatt ME. Infections and anti-tumor necrosis factor alpha therapy. Arthritis Rheum. 2003;48(11):3013–3022.
24. Perlmutter A, Mittal A, Menter A. Tuberculosis and tumour necrosis factor-alpha inhibitor therapy: a report of three cases in patients with psoriasis. Comprehensive screening and therapeutic guidelines for clinicians. Br J Dermatol. 2009;160(1):8–15. Epub 2008 Oct 22.
25. Doherty SD, Van Voorhees A, Lebwohl MG, et al. National Psoriasis Foundation consensus statement on screening for latent tuberculosis infection in patients with psoriasis treated with systemic and biologic agents. J Am Acad Dermatol. 2008;59(2):209–217. Epub 2008 May 15.
26. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. J Am Acad Dermatol. 2008;58(5):826–850.
27. Walsh MJ, Vanags DM, Clouston AD, et al. Steatosis and liver cell apoptosis in chronic hepatitis C: a mechanism for increased liver injury. Hepatology. 2004;39(5):1230–1238.
28. Herbein G, O’Brien WA. Tumor necrosis factor (TNF)-alpha and TNF receptors in viral pathogenesis. Proc Soc Exp Biol Med. 2000;223(3):241–257.
29. Domm S, Cinatl J, Mrowietz U. The impact of treatment with tumour necrosis factor-alpha antagonists on the course of chronic viral infections: a review of the literature. Br J Dermatol. 2008;159(6):1217–1228. Epub 2008 Sep 25.
30. Roux CH, Brocq O, Breuil V, et al. Safety of anti-TNF-alpha therapy in rheumatoid arthritis and spondylarthropathies with concurrent B or C chronic hepatitis. Rheumatology (Oxford). 2006;45(10):1294–1297. Epub 2006 Apr 7.
31. Cooley L, Sasadeusz J. Clinical and virological aspects of hepatitis B co-infection in individuals infected with human immunodeficiency virus type-1. J Clin Virol. 2003;26(2): 185–193.
32. Sulkowski MS. Viral hepatitis and HIV coinfection. J Hepatol. 2008;48(2):353–367. Epub 2007 Dec 4.
33. Soto B, Sánchez-Quijano A, Rodrigo L, et al. Human immunodeficiency virus infection modifies the natural history of chronic parenterally acquired hepatitis C with an unusually rapid progression to cirrhosis. J Hepatol. 1997;26(1):1–5.
34. Nathan DM, Angus PW, Gibson PR. Hepatitis B and C virus infections and anti-tumor necrosis factor-alpha therapy: guidelines for clinical approach. J Gastroenterol Hepatol. 2006;21(9):1366–1371.
35. Zein NN, Etanercept Study Group. Etanercept as an adjuvant to interferon and ribavirin in treatment-naive patients with chronic hepatitis C virus infection: a phase 2 randomized, double-blind, placebo-controlled study. J Hepatol. 2005;42(3):315–322.
36. Meola T, Soter NA, Ostreicher R, et al. The safety of UVB phototherapy in patients with HIV infection. J Am Acad Dermatol. 1993;29(2 Pt 1):216–220.
37. Stern RS, Mills DK, Krell K, et al. HIV-positive patients differ from HIV-negative patients in indications for and type of UV therapy used. J Am Acad Dermatol. 1998;39(1):48–55.
38. Houpt KR, Beer JZ, Horn TD, et al. Ultraviolet therapy of HIV-infected individuals: a panel discussion. Semin Cutan Med Surg. 1997;16(3):241–245.
39. Beer JZ, Zmudzka BZ. UVB and PUVA therapies in HIV patients: are they safe? Photodermatol Photoimmunol Photomed. 1997;13(3):91–92.
40. Akaraphanth R, Lim HW. HIV, UV and immunosuppression. Photodermatol Photoimmunol Photomed. 1999;15(1): 28–31.
41. Kuwano Y, Watanabe R, Fujimoto M, et al. Treatment of HIV-associated eosinophilic pustular folliculitis with narrowband UVB. Int J Dermatol. 2006;45(10):1265–1267.
42. Morison WL. PUVA therapy is preferable to UVB phototherapy in the management of HIV-associated dermatoses. Photochem Photobiol. 1996;64(2):267–268.
43. Breuer-McHam J, Marshall G, Adu-Oppong A, et al. Alterations in HIV expression in AIDS patients with psoriasis or pruritus treated with phototherapy. J Am Acad Dermatol. 1999;40(1):48–60.
44. Calabrese LH, Lederman MM, Spritzler J, et al. Placebo-controlled trial of cyclosporin-A in HIV-1 disease: implications for solid organ transplantation. J Acquir Immune Defic Syndr. 2002;29(4):356–362.
45. Stock P, Roland M, Carlson L, et al. Solid organ transplantation in HIV-positive patients. Transplant Proc. 2001;33(7–8):3646–3648.
46. Tourne L, Durez P, Van Vooren JP, et al. Alleviation of HIV-associated psoriasis and psoriatic arthritis with cyclosporine. J Am Acad Dermatol. 1997;37(3 Pt 1):501–502.
47. Allen BR. Use of cyclosporin for psoriasis in HIV-positive patient. Lancet. 1992;339(8794):686.
48. Galeazzi M, Giannitti C, Manganelli S, et al. Treatment of rheumatic diseases in patients with HCV and HIV infection. Autoimmun Rev. 2008;8(2):100–103.
49. Maurer TA, Zackheim HS, Tuffanelli L, Berger TG. The use of methotrexate for treatment of psoriasis in patients with HIV infection. J Am Acad Dermatol. 1994;31(2 Pt 2):372–375.
50. Masson C, Chennebault JM, Leclech C. Is HIV infection contraindication to the use of methotrexate in psoriatic arthritis? J Rheumatol. 1995;22(11):2191.
51. Chernyshov P. Testing for HIV prior to methotrexate administration. Is it an obligatory procedure? Int J Dermatol. 2006;45(8):998–999.
52. Baker BS, Griffiths CE, Lambert S, et al. The effects of cyclosporine A on T lymphocyte and dendritic cell subpopulations in psoriasis. Transplant Proc. 1988;20(3 Suppl 4):72–77.
53. Kiyohara A, Takamori K, Niizuma N, Ogawa H. Successful treatment of severe recurrent Reiter’s syndrome with cyclosporine. J Am Acad Dermatol. 1997;36(3 Pt 1): 482–483.
54. Blanche P. Acitretin and AIDS-related Reiter’s disease. Clin Exp Rheumatol. 1999;17(1):105–106.
55. Buccheri L, Katchen BR, Karter AJ, Cohen SR. Acitretin therapy is effective for psoriasis associated with human immunodeficiency virus infection. Arch Dermatol. 1997;133(6):711–715.
56. Ting PT, Koo JY. Use of etanercept in human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) patients. Int J Dermatol. 2006;45(6):689–692.
57. Calabrese LH, Zein N, Vassilopoulos D. Safety of antitumour necrosis factor (anti-TNF) therapy in patients with chronic viral infections: hepatitis C, hepatitis B, and HIV infection. Ann Rheum Dis. 2004;63(Suppl 2):ii18–ii24.
58. Wachi K, Prasertsuntarasai T, Kishimoto M, Uramoto K. T-cell lymphopenia associated with infliximab and cyclophosphamide. Am J Med Sci. 2005;330(1):48–51.
59. Sha BE, Valdez H, Gelman RS, et al. Effect of etanercept (Enbrel) on interleukin 6, tumor necrosis factor alpha, and markers of immune activation in HIV-infected subjects receiving interleukin 2. AIDS Res Hum Retroviruses. 2002;18(9):661–665.
60. Wallis RS, Kyambadde P, Johnson JL, et al. A study of the safety, immunology, virology, and microbiology of adj