Lidiane Pereira Marques, MD; Beatriz Moritz Trope, MD, PhD; Juliana Carnevale Pina, MD; Tullia Cuzzi, MD, PhD; Marcia Ramos-e-Silva, MD, PhD
Dr. Marques is from Federal University of Rio de Janeiro. Dr. Trope is Dermatologist, Sector of Dermatology and Post-Graduation Course in Dermatology, HUCFF and School of Medicine. Dr. Carnevale is Post Graduation Student, Sector of Dermatology and Post-Graduation Course in Dermatology, HUCFF and School of Medicine, Federal University of Rio de Janeiro. Dr. Cuzzi is Associate Professor, Sector of Pathology and Post-Graduation Course in Dermatology, HUCFF and School of Medicine, Federal University of Rio de Janeiro. Dr. Ramos-e-Silva is Associate Professor and Head, Sector of Dermatology and Post-Graduation Course in Dermatology, HUCFF and School of Medicine, Federal University of Rio de Janeiro, Brazil
Abstract
Acrokeratoelastoidosis of Oswaldo Costa, or inverse papular acrokeratosis, is a rare genodermatosis first described in 1952 by Oswaldo Costa, a Brazilian dermatologist. It is characterized by flesh-colored papules on the lateral aspects of the palms and soles and dorsum of hands. The histological features are hyperkeratosis, hyalinized and homogenous collagen, and a decrease in and fragmentation of the elastic fibers (elastorrhexis). In the absence of elastic fiber fragmentation, a similar clinical presentation is diagnosed as focal acral hyperkeratosis. Many cases of inverse papular acrokeratosis of Oswaldo Costa may have been considered focal acral hyperkeratosis since it can be difficult to find the elastorrhexis. The authors report a case of a 51-year-old woman with inverse papular acrokeratosis of Oswaldo Costa with poor response to topical treatments. (J Clin Aesthetic Dermatol. 2010;3(6):51–53.)
A 51-year-old black woman from Rio de Janeiro complained of “small bumps on feet,” present for seven years. She sought medical consultation and used several creams with discreet improvement and subsequent worsening. Two years earlier she noticed similar lesions on her hands. She knows of no other cases in the her family and does not have a history of consanguinity. There was no history of exposure to arsenic, and she had no other symptoms.
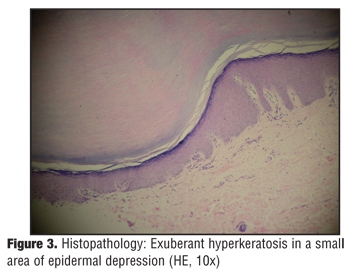
She presented with flesh-colored papules on the medial and lateral borders of the hands and feet (Figure 1 and Figure 2). She did not present with palmoplantar desquamation, hyperhydrosis, vesicles, crusts or ungual alterations, or dermatological lesions on other sites. Histopathology showed more exuberant hyperkeratosis in small areas of epidermal depression. Orcein stain revealed a decrease and fragmentation of the elastic fibers. The histopathological picture was compatible with acrokeratoelastoidosis (Figure 3).
{kind=link}
{kind=link}
{kind=link}
Discussion
The most important characteristic of marginal keratoderma is the involvement of the borders or palmoplantar transition areas, which are called inverse when they compromise the dorsum of the hands and feet.[1]
Inverse papular acrokeratosis was the denomination given by the Brazilian dermatologist Oswaldo Costa to replace the name lichenoid akrokeratoelastoidosis, previously coined by him in 1952.[2,3] Also known as acrokeratosis of Oswaldo Costa, it is a genodermatosis in which the basic lesion is a horny, translucid papule encrusted in the epidermis or slightly elevated and round with variable dimensions and a smooth or slightly depressed surface, sometimes separated by small epidermal grooves. Common locations are the anterior sides of fists; lateral and medial borders of hands and feet; pre-tibial regions; and occasionally dorsum of fingers, toes, and feet. Traumatic factors, such as handwashing clothes and irritation from shoes, can increase the dimensions of inverse papular acrokeratosis.[2]
Inverse papular acrokeratosis is more frequent in black women, and its onset usually occurs between 20 and 30 years of age and can be sporadic or transmitted by autosomal dominant inheritance with great morphological variability of expression. Usually, no subjective symptoms are observed.[2–4]
Histopathology reveals horny hyperplasia as well as elastorrhexis and collagen homogenization. Hyperkeratosis causes depression in the underlying epithelial planes, forming a concavity. One observes areas of collagen homogenization in the superficial dermis with thin elastic and reduced and fragmented fibers. Electron microscopy shows disaggregation of elastic fibers with microfibrillar fragmentation. There are reports of presence of fibroblasts with dense cytoplasmatic granules, leading to the hypothesis of elastic fiber synthesis blocking by the fibroblasts.
The importance of the elastic fiber fragmentation in the differential diagnosis with another entity (in which the clinical aspects resemble inverse papular acrokeratosis) called acral focal hyperkeratosis, described by Dowd et al[5] in 1983, is worth mentioning. Histological alterations, however, are restricted to epidermis (hyperkeratosis), without alterations of elastic fibers (elastorrhexis) in the reticular dermis.[5–8]
Asymptomatic inverse papular acrokeratosis, sometimes presenting with a discreet clinical picture, reduces the chances of diagnosis in such conditions, which is why reports in the literature on this condition are scarce. Knowledge of inverse papular acrokeratosis is important for differentiation from verruca plana, primary cutaneous amyloidosis, acrokeratosis verruciformis of Hopf, focal acral hyperkeratosis, and other keratoderma.[9,10] The group of marginal keratoderma comprises several illnesses, many not being distinct diseases, but merely clinical variants.
Histopathology helps in the diagnosis of inverse papular acrokeratosis of Oswaldo Costa due to the specific alterations described by him.[2]
The correct diagnosis of inverse papular acrokeratosis of Oswaldo Costa enables physicians to educate patients regarding the benignity of this condition since treatment with keratolytics is usually inefficient. Being a genodermatosis, Acrokeratosis de Oswaldo Costa has only symptomatic and palliative treatment, with emollients and keratolytic agents, salicylates, sulphur, and urea formulas, as well as topical and systemic isotretinoin. In the vast majority of cases, the patient’s complaint is purely aesthetic, since there is no functional damage.
Authors’ Note
Oswaldo Costa, a dermatologist born in Minas Gerais, Brazil, was a persistent researcher of acrokeratoses. His 577-page thesis on the subject contributed to the knowledge of palmo-plantar keratoderma, the enrichment of dermatology, and Brazilian science.
References
1. Stevens HP, Leigh IM. The inherited keratodermas of palms and soles. In: Freedberg IM, Eisen AZ, Wolff K, et al. Fitzpatrick’s Dermatology in General Medicine. 5 ed. Philadelphia: MacGraw-Hill; 1998:604–612.
2. Costa OG. Acrokeratosis (palmo-plantar keratodermas) thesis for the exam for full professor of the dermatology and syphilographic clinics of the school of medicine of the University of Minas Gerais; Belo Horizonte, State of Minas Gerais, Brazil; 1962.
3. Costa OG. Acrokeratoelastosis. Arch Dermatol. 1954;70: 228–231.
4. Johansson EA, Kariniemi AL, Niemi KM. Palmoplantar keratoderma of punctate type: acrokeratoelastoidosis Costa. Acta Derm Venereol. 1980;60(2):149–153.
5. Dowd PM, Harman RR, Black MM. Focal acral hyperkeratosis Br J Dermatol. 1983;109(1):97–103.
6. Erkek E, Kocak M, Bozdogan O, et al. Focal acral hyperkeratosis: a rare cutaneous disorder within the spectrum of Costa acrokeratoelastoidosis. Pediatr Dermatol. 2004;21(2):128–130.
7. Cunha Filho RR, Almeida Jr HL. Hiperceratose focal acral associada à hipocromia de dermatóglifos. An Bras Dermatol. 2008;83(5):441–443.
8. Hafner O, Gerstel C. Focal acral hyperkeratosis. Hautarzt. 1999;50(8):586–589.
9. Tsai S, Kageyama N, Warthan M, et al. Acrokeratoelastoidosis. Int J Dermatol. 2005;44(5):406–407.
10. Rongioletti F, Betti R, Crosti C, et al. Marginal papular acrokeratodermas: a unified nosography for focal acral hyperkeratosis, acrokeratoelastoidosis and related disorders. Dermatology. 1994;188(1):28–31.
OX40/OX40L Costimulatory Pathway: A Potential Therapeutic Target for Allergic Contact Dermatitis?