Philip R. Cohen, MD
The University of Houston Health Center, University of Houston, Houston, Texas; The Department of Dermatology, The University of Texas M.D. Anderson Cancer Center, Houston, Texas; and The Department of Dermatology, University of Texas–Houston Medical School, Houston, Texas
Disclosure: The author reports no relevant conflicts of interest. No sources of funding were used to assist in the preparation of this review.
Abstract
Objective: To describe the clinical features of idiopathic polydactylous longitudinal erythronychia. Introduction: Longitudinal erythronychia presents as a linear red band on the nail plate. Idiopathic polydactylous longitudinal erythronychia is a rarely described manifestation of longitudinal erythronychia in which one or more linear red bands present on the nails of multiple digits without any associated subungual malignant tumor, dermatological condition, or systemic disease. Methods: As part of a total body skin examination, the fingernails and toenails were evaluated for linear red bands. Results: One or more asymptomatic linear red bands (longitudinal erythronychia) was observed on multiple digits of the hands in one percent (3 men of 134 men and 112 women) of patients examined during a period of 75 days. The author also noted similar changes of his own nails. Between 3 to 10 digits were affected. Multiple linear red bands per nail were usually narrow (less than 1mm wide), whereas a single band on a nail often ranged from 4 to 6mm wide. The intensity of an individual wider linear red band was position-dependent in three individuals in whom the distal portion appeared less prominent when the affected digit was held upward above the level of the patient’s heart—pseudolongitudinal erythronychia. Other nail changes in these patients included distal subungual hyperkeratosis, fissuring at the free end of the nail, leukonychia, red lunula, and splinter hemorrhages. Discussion: Idiopathic polydactylous longitudinal erythronychia is a benign, usually asymptomatic, condition of undetermined etiology characterized by one or more linear red bands originating at the proximal nail fold or distal lunula and extending to the free edge of the nail. It appears to be more prevalent in men over 50 years of age and its incidence was noted to be one percent of adults attending a dermatology clinic. Patients are either unaware of the nail changes or seek medical attention because of the nail plate appearance. Other nail changes can concurrently be observed including pseudolongitudinal erythronychia in which the distal intensity of an individual wider red band is less pronounced when the digit is held upward. Idiopathic polydactylous longitudinal erythronychia has not been associated with benign or malignant subungual tumors, dermatological conditions, or systemic diseases. Conclusion: Idiopathic polydactylous longitudinal erythronychia may represent as a benign, possibly age-related, nail change without any associated local or systemic adverse sequellae. (J Clin Aesthet Dermatol. 2011;4(4):22–28.)
Longitudinal erythronychia is a linear red band that usually extends from the proximal nail fold to the distal tip of the nail plate. It is classified based on the number of affected digits and the number of red bands on those digits (Table 1). Longitudinal erythronychia can be idiopathic or associated with benign or malignant subungual tumors, dermatological conditions, or systemic diseases.[1,2]
{kind=link}
Idiopathic polydactylous longitudinal erythronychia presents as either Type IIA (polydactylous—single band) longitudinal erythronychia or Type IIB (polydactylous—multiple bands) longitudinal erythronychia.[1,2] Single or multiple linear red bands, not associated with any local or systemic disorder, are observed on the nails. This paper reports four individuals with this unique nail condition (3 patients attending a dermatology clinic and the author) and summarizes the features of idiopathic polydactylous longitudinal erythronychia.
Materials and Methods
An evaluation of fingernails and toenails for linear red bands, as part of the total body skin examination, during the patient’s visit to a dermatology clinic was conducted for 75 days from July 5, 2010, to September 17, 2010.
Report of Cases
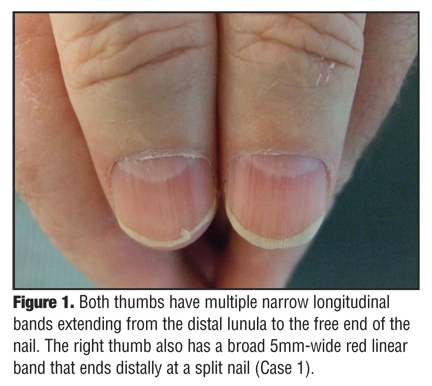
Case 1. A 56-year-old man had asymptomatic red longitudinal bands, which he had never noticed, on both of his thumbnails and all fingernails; none were on his toenails. The right thumbnail had a broad red band of 5mm width that ended at a site of distal nail splitting; both thumbnails had multiple small red linear streaks extending from the distal lunula to the free end of the nail (Figure 1). The fingernails each had 2 to 5 narrow, less than 1mm, red, linear streaks that extended from the proximal nail fold to the free end of the nail plate (Figure 2).
{kind=link}
{kind=link}
Case 2. A 60-year-old man had asymptomatic red longitudinal bands that extended from the proximal nail fold, transversed the lunula, and reached the distal-free edge on his right second (1 band), third (3 bands), and fourth (2 bands) fingernails; descriptive illustrations of his nail changes have previously been reported.[2] The patient had never previously noted these nail changes. The red linear streaks on the middle and ring fingers were 1mm wide. The single red linear streak on the index finger was 4mm wide and very prominent when his right hand was held in a dependent downward position. However, when he raised his right arm upward above his heart, the intensity of the red longitudinal band was only preserved proximally and was markedly diminished distally. It could only be faintly observed from the mid-nail plate to the distal-free edge. In contrast, the intensity of the red streaks on the third and fourth fingernails was preserved.
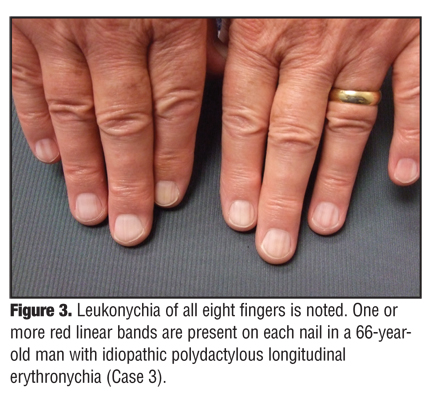
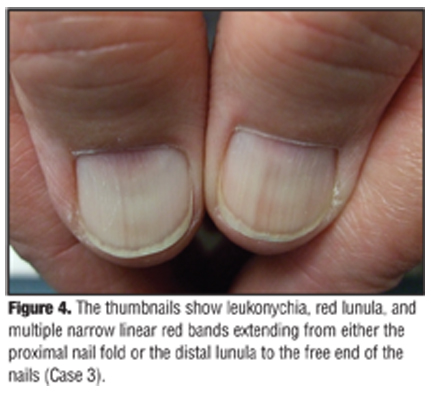
Case 3. A 66-year-old man had leukonychia of all 20 nails (Figure 3). He also had red lunula that was readily observed on both thumbnails and also noted on his left middle fingernail and right index fingernail (Figure 4).[3] He was previously unaware of these nail changes. Asymptomatic red longitudinal bands were present on the nails of all digits of both hands. His thumbnails both have red longitudinal streaks that extend from either the proximal nailfold (laterally) or the lunula (centrally) and reach the free edge of the nails (Figure 4). His left thumbnail has more than six red linear streaks ranging from 1mm to less than 1mm in width of which the two central streaks are darker. His right thumbnail has two prominent red streaks (both less than 1mm wide) and several less intense streaks.
{kind=link}
{kind=link}
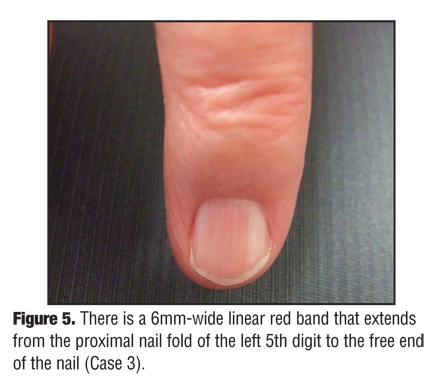
The fingernails on his left hand have one or more red longitudinal bands: his second digit has three bands, his third has three, his fourth has two, and his fifth has one. Similarly, the fingernails on the right hand have two or more red longitudinal bands. Most of the red linear streaks are less than or equal to 1mm wide. However, the red band on the left little finger is 6mm wide (Figure 5) and the red bands on the right fifth digit are 2mm wide (central streak) and 3mm wide (lateral streak that extends to the lateral nail fold).
{kind=link}
The intensity of the wider red longitudinal band on the left little finger is variable depending on the position of the hand. When the left hand is held downward below the heart, the red linear streak is prominent. Yet, when the left hand is held upward above the heart, the intensity of the red linear streak is diminished distally and is less apparent from the mid-nail to its free edge. In contrast, the red linear streaks of the nails on the second, third, and fourth digits are unchanged and equally intense when the left hand is raised (Figure 6).
{kind=link}
Case 4. The author, an otherwise healthy 51-year-old dermatologist, discovered asymptomatic, linear, red bands on his own fingernails while he was preparing a review article on the subject.[2] His past medical history is remarkable for recurrent, running-associated, subungual hematomas of the right great toenail and left second toenail following the completion of an annual marathon.[4,5]
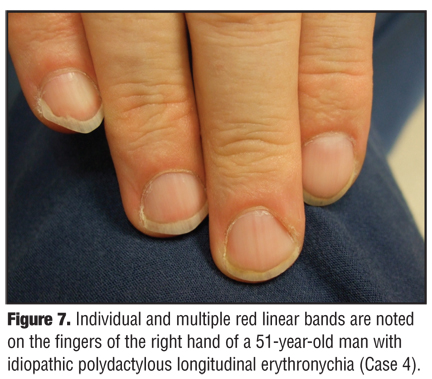
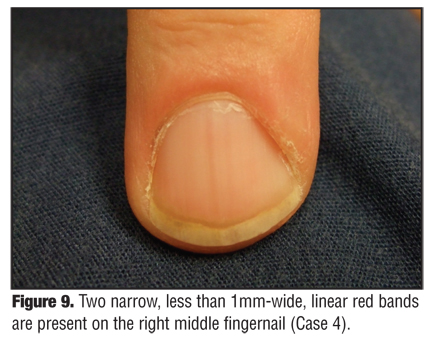
Examination of his fingernails showed asymptomatic longitudinal red bands on the nails of the second, third,and fifth digits of both hands (Figure 7). The left hand has three linear red streaks on the index fingernail and two linear red streaks on the middle and pinky fingernails; all were less than 1mm wide. The index fingernail (Figure 8) and middle fingernail (Figure 9) on the right hand have one linear streak (5mm in width) and two linear streaks (each less than 1mm in width), respectively; the fourth and fifth fingernails have at least four red linear streaks (each less than 1mm wide). When the right hand is held upward (above the level of the heart), the intensity of the distal red longitudinal band on the right index finger is diminished.
{kind=link}
{kind=link}
{kind=link}
Results
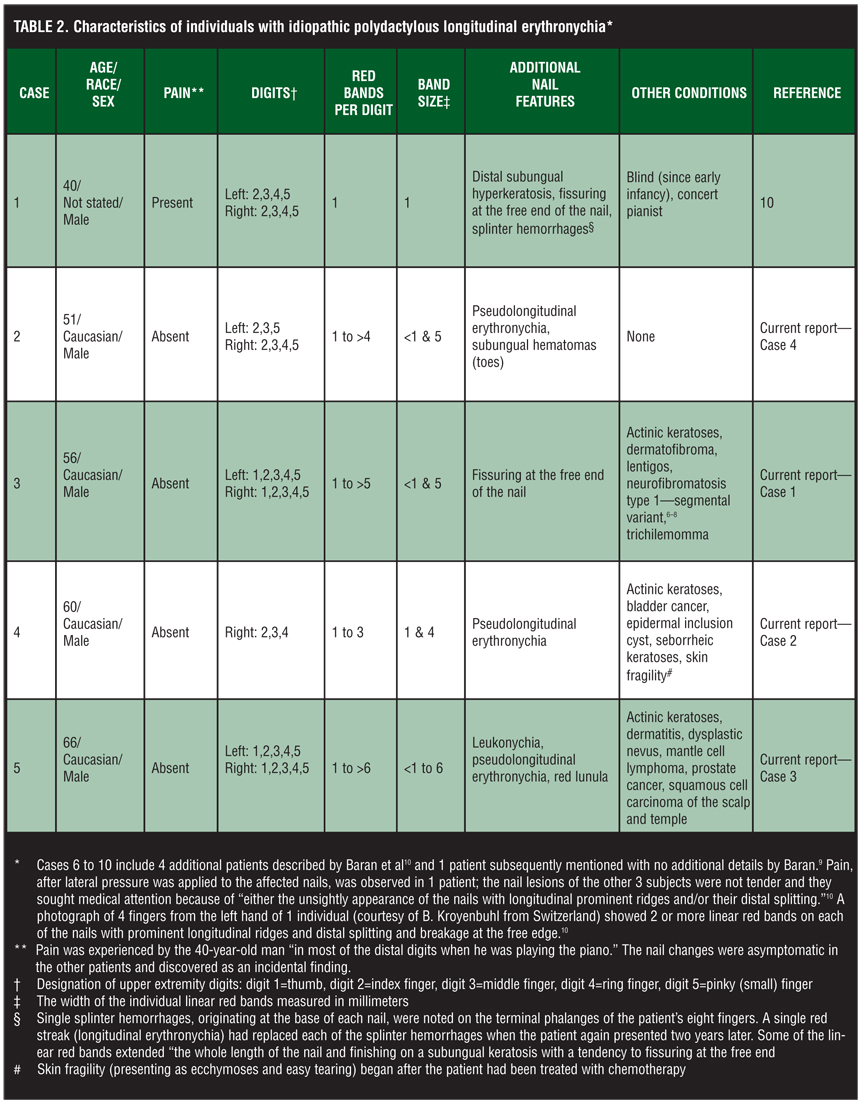
A total of 246 patients (134 men and 112 women) were seen at the 18 visits during the 10.5 weeks of examinations. Linear red bands were observed on multiple nails in three patients. In addition, linear red bands were also noted on the fingernails of the dermatologist doing the examinations. The clinical features of these individuals (and those previously reported with idiopathic polydactylous longitudinal erythronychia) are summarized in Table 2.[6–10]
{kind=link}
Discussion
Polydactylous longitudinal erythronychia presents with either single or multiple linear red bands on the nails of multiple digits. This nail finding has more frequently been reported in patients with either associated dermatological conditions or systemic diseases (Table 3).[1,9–15] In contrast, monodactylous longitudinal erythronychia usually appears as a single, linear red band on only one digit and is typically associated with benign—or less commonly malignant—subungual tumors.[16–18] Occasionally, it is observed either on the thumbnail of the paralyzed arm in patients with hemiplegia or as a consequence of postsurgical scar of the distal digit or as an idiopathic finding.[18–22]
{kind=link}
Idiopathic polydactylous longitudinal erythronychia was introduced by Baran et al as “a newly described entity” in the July 2006 issue of the British Journal of Dermatology.[10] The authors reported five individuals with this “rare condition.” Their correspondence included clinical photographs of the fingernails from two patients and a detailed account of one patient (including pathology and magnetic resonance imaging studies). A subsequent paper by Baran refers to another patient; however, no details are provided.[9]
Idiopathic polydactylous longitudinal erythronychia has been reported in 10 individuals, including those presented herein. At least five of the patients have been men ranging in age from 40 to 66 years (median 56 years). The incidence of this condition was one percent overall (3 of 246 patients), but was two percent of the men evaluated (3 of 134 patients).
The 40-year-old man described in detail by Baran et al was a concert pianist who had been blind since early infancy.[10] Other dermatological and medical conditions noted in patients with idiopathic polydactylous longitudinal erythronychia are actinic keratoses, dermatofibroma, dermatitis, dysplastic nevi, epidermal inclusion cysts, lentigos, neurofibromatosis type 1—segmental variant, seborrheic keratoses, skin fragility, trichilemmoma and cancer (bladder, mantle cell lymphoma, prostate, and squamous cell carcinoma of the skin). It is likely that these conditions are not associated with the subsequent development of idiopathic polydactylous longitudinal erythronychia.
This nail condition is usually asymptomatic. At least 7 of the 10 patients had no tenderness of the affected digits. The appearance of the nail (“with longitudinal prominent ridges and/or their distal splitting”) prompted three individuals to seek medical attention.[10] The nail change had not previously been noticed by three of the patients until they were made aware of the condition at their dermatology appointment. Similarly, the observation of this condition in the author was a coincidental discovery.
However, in two patients, idiopathic polydactylous longitudinal erythronychia presented with pain. The pianist had tenderness “in most of the distal fingers when he was playing the piano.”[10] A second person also experienced pain, which occurred after lateral pressure was applied to the affected nails.[10]
Idiopathic polydactylous longitudinal erythronychia has only been observed, thus far, on the digits of the upper extremities. It usually presents bilaterally and typically affects at least 3 or 4 fingernails. The thumbnails were also involved in two patients.
The red linear streaks originate from the proximal nail fold or the distal margin of the lunula and extend to the free edge of the nail plate. Only the pianist had one linear red band on each of his eight digits (excluding his thumbs) that had replaced a splinter hemorrhage, which had been noted two years previously.[10] The number of bands per nail was variable in the other patients. Each of the affected nails had one or more red longitudinal band; one person had more than six bands on a single nail.
The width of the linear red bands varies. Typically, a small width (less than or equal to 1mm) is noted when there are several longitudinal bands on the same nail. And, when only a single linear band is present, the width ranged from 4 to 6mm.
The distal intensity of the wider, single red longitudinal band was noted to be position-dependent in three patients. Pseudolongitudinal erythronychia is a descriptive term to describe the position-dependent variable distal intensity of the red linear band. A confluent longitudinal wider red band is observed on the fingernail when the ipsilateral arm is positioned downward, below the level of the patient’s heart; however, when that hand is elevated and held upward above the level of the heart, the intensity of the distal half of the red linear band that was initially visible is now markedly diminished or absent. Yet, the intensity of the thinner, red linear streaks on the patient’s adjacent fingernails remains unchanged. These observations prompt consideration that pseudolongitudinal erythronychia may, in part, be secondary to a localized vascular phenomenon.
Associated nail changes, similar to those observed in monodactylous longitudinal erythronychia, included distal subungual hyperkeratosis (in 1 patient) and fissuring at the free end of the nail presenting as either distal nail plate splitting or breaking at the nail plate’s free edge or both (in 3 patients). One patient, the pianist, also initially presented with splinter hemorrhages, which subsequently developed—over a two-year period—into linear red bands.10 Other changes concurrently occurring in the affected nails of one patient with idiopathic polydactylous longitudinal erythronychia were leukonychia and red lunula.
Idiopathic polydactylous longitudinal erythronychia is favored to represent a benign nail change that is often only discovered incidentally. This is in contrast to monodactylous longitudinal erythronychia, which may be associated with a benign subungual tumor (onychopapilloma), but can be related—albeit rarely—with either a subungual squamous cell carcinoma or subungual amelanotic malignant melanoma.[1,17,18] Therefore, it is not surprising that most patients with idiopathic polydactylous longitudinal erythronychia have not undergone biopsy of the nail bed of an affected digit.
However, Baran’s pianist had two biopsies of the longitudinal erythronychia on his left third finger performed: One was a punch biopsy at the proximal end of the red band in the lunula and the second was a shave biopsy of the distal subungual keratosis. The punch biopsy showed a lichenoid reaction: There was a “thin epithelium without basal alteration, underlined by a band-like infiltrate of lymphocytes associated with numerous vessels. The infiltrate did not obscure the interface or extend into the epithelium. There was some extravasation of red blood cells into the dermis, but hemosiderin was absent.”[10] The shave biopsy demonstrated a mass characterized by orthokeratosis and parakeratosis.10
Conclusion
Idiopathic polydactylous longitudinal erythronychia is a benign condition of undetermined etiology characterized by one or more linear red bands originating at the proximal nail fold or distal lunula and extending to the free edge of the nail. Typically, the condition is asymptomatic and patients are either unaware of the nail changes or seek medical attention because of the cosmetic appearance of their nail plates. The linear red bands usually appear on the fingernails of both hands; however, they can also be present on the thumbnails. Multiple bands on the same nail are typically less than or equal to 1mm in width, yet individual bands can be from 4 to 6mm wide.
Pseudolongitudinal erythronychia has been observed to affect the wider single red linear band in patients with idiopathic polydactylous longitudinal erythronychia. The intensity of the distal portion of the band becomes markedly diminished or absent when the nail of the affected digit is held above the level of the heart. The pathogenesis of pseudolongitudinal erythronychia remains to be established and may be related to a localized vascular phenomenon.
The incidence of idiopathic polydactylous longitudinal erythronychia in patients attending a dermatology clinic for other reasons was found to be approximately one percent. The condition appears to be observed more commonly in men over the age of 50 years. Similar to the benign clinical behavior associated with multiple black or brown linear bands in patients with polydactylous longitudinal melanonychia striata, the discovery of idiopathic polydactylous longitudinal erythronychia (with or without concurrent pseudolongitudinal erythronychia) appears to not be associated with any adverse sequellae. However, due to the paucity of published individuals with this condition, additional observations and reports of patients with this condition are encouraged.
References
1. Jellinek NJ. Longitudinal erythronychia: suggestions for evaluation and management. J Am Acad Dermatol. 2011;37:74–79.
2. Cohen PR. Longitudinal erythronychia: individual or multiple linear red bands of the nail plate—a review of clinical features and associated conditions. Am J Clin Dermatol. 2011. In press.
3. Cohen PR. Red lunula: case report and literature review. J Am Acad Dermatol. 1992;26:292–294.
4. Cohen PR, Schulze KE, Nelson BR. Subungual hematoma [clinical snapshot]. Dermatol Nurs. 2007;19(1):83–84.
5. Cohen PR. What caused these painful purple toes? Subungual hematoma [Derm Dx]. Skin & Aging. 2009;17(9):54–58.
6. Hagar CM, Cohen PR, Tschen JA. Segmental neuro-fibromatosis: case reports and review. J Am Acad Dermatol. 1997;37:864–869.
7. Dang JD, Cohen PR. Segmental neurofibromatosis of the distal arm in a man who developed Hodgkin lymphoma. Int J Dermatol. 2009;48:1105–1109.
8. Dang JD, Cohen PR. Segmental neurofibromatosis and malignancy. SKINmed. 2010;8:156–159.
9. Baran R. The red nail—always benign? Actas Dermosifiliogr. 2009;100 (Suppl 1):106–113.
10. Baran R, Dawber RPR, Perrin C, Drape JL. Idiopathic polydactylous longitudinal erythronychia: a newly described entity. [Letter] Br J Dermatol. 2006;155:219–221.
11. Munro CS, Cox NH. An acantholytic dyskeratotic epidermal naevus with other features of Darier’s disease on the same site of the body. Br J Dermatol. 1992;127;168–171.
12. Hoffman MD, Fleming MG, Pearson RW. Acantholytic epidermolysis bullosa. Arch Dermatol. 1995;131:586–589.
13. Dhitavat J, Macfarlane S, Dode L, et al. Acrokeratosis verruciformis of Hopf is caused by mutation in ATP2A2: evidence that it is allelic to Darier’s disease. J Invest Dermatol. 2003;120:229–232.
14. Cohen PR. The lunula. J Am Acad Dermatol. 1996;34: 943–953.
15. Siragusa M, Del Gracco S, Ferri R, Schepis C. Longitudinal red streaks on the big toenails in a patient with pseudobulbar syndrome. [letter] J European Academy of Dermatology and Venereology. 2001;15:85–86.
16. Rashid RM, Torres-Cabala C, Chon S. Longitudinal erythronychia: the value of cosmetic alterations in nail findings. SKINmed. 2011;9:60–61.
17. Baran R, Perrin C.: Longitudinal erythronychia with distal subungual keratosis: onychopapilloma of the nail bed and Bowen’s disease. Br J Dermatol. 2000;143:132–135.
18. de Berker DA, Perrin C, Baran R. Localized longitudinal erythronychia: diagnostic significance and physical explanation. Arch Dermatol. 2004;140:1253–1257.
19. Siragusa M, Schepis C, Palazzo R, et al. Skin pathology findings in a cohort of 1,500 adult and elderly subjects. Int J Dermatol. 1999;38:361–366.
20. Siragusa M, Schepis C, Cosentino ELL, et al. Nail pathology in patients with hemiplegia. Br J Dermatol. 2001;144:557–560.
21. Abimelec P, Dumontier C. Basic and advanced nail surgery (part 2: indications and complications) (Chapter 24). In: Scher RK, Daniel CR III, eds. Nails: Diagnosis, Therapy, Surgery. 3rd ed. Philadelphia: Elsevier Saunders; 2005:291–308.
22. Gee BC, Millard PR, Dawber RPR. Onychopapilloma is not a distinct clinicopathological entity. [Letter] Br J Dermatol. 2002;146:156.