Skin of color
Section Editors: Seemal R. Desai, MD, FAAD; Andrew Alexis, MD, FAAD, and Andrew Alexis, MD, FAAD
Dr. Desai is Clinical Assistant Professor in the Department of Dermatology at the University of Texas Southwestern Medical Center and is the President & Medical of Innovative Dermatology, PA in Dallas, Texas. He has served in numerous leadership roles within the American Academy of Dermatology, American Medical Association, Texas Dermatological Society, and Skin of Color Society. Disclosure: The author reports no relevant conflicts of interest in the preparation or content of this manuscript.
Message from Seemal R. Desai, MD, FAAD
Disorders of pigmentation, dyschromias, scarring from acne, and other conditions, along with a host of other dermatoses are treatment challenges that all dermatologists face on a daily basis. Dr. Andrew Alexis and I are honored to serve as the Section Editors of the new Skin of Color Special Section of The Journal of Clinical and Aesthetic Dermatology and would like to personally thank Dr. Jim Del Rosso for welcoming this increasingly relevant topic into this highly respected journal. We welcome your ideas, comments, and suggestions for future pieces that you think would be valuable in treating your patients with skin of color and hope that this first article on hyperpigmentation will pique your interest in the topic of skin of color and its diagnosis and management. Whenever approaching patients with skin of color, it is important to understand that no single therapy exists to achieve the perfect balance of skin lightening and maintaining cutaneous integrity. This mantra is most relevant in the treatment of hyperpigmentation, including melasma, postinflammatory pigmentary alteration, drug-induced causes, or other etiologies. The bottom line is that it is important to keep an open mind regarding a multi-therapy approach, possibly involving in-office based procedures, and/or newer more literature-based treatment modalities. (J Clin Aesthet Dermatol. 2014;7(8):13–17.)
Abstract
With an increasing number of multicultural patients and those of different backgrounds presenting in dermatology clinics, issues facing patients with higher Fitzpatrick skin classifications, often referred to as skin of color patients, are on the rise. Knowledge of the diagnostic dilemmas, cutting edge treatment options, and latest clinical research in the diagnosis and management of cutaneous anomalies in skin of color patients is of paramount importance. Of the most common complaints in patients with skin of color is hyperpigmentation. Despite the availability of multiple treatments for the condition, hyperpigmentation continues to present clinical management challenges for dermatologists. Difficulty may be traced to physician or patient reluctance to use certain agents or interventions, failure to identify and avoid contributing factors, and insufficient attention paid to the psychosocial aspects of the disease. This review addresses a variety of issues including the diagnosis and management of hyperpigmentation.
Evaluation of Hyperpigmentation
Hyperpigmentation may be localized, as in the case of post-inflammatory hyperpigmentation or melasma, or more diffuse in its presentation. Diffuse hyperpigmentation tends to be associated with metabolic causes, certain medications, malignancy, or autoimmune or infectious etiologies (Table 1). Since diffuse hyperpigmentation may be associated with malignancy or may be improved through treatment of the underlying disease process or insufficiency or elimination of the causative medication, it is important to identify the cause.
{kind=link}
Causes of Diffuse Hyperpigmentation
There are numerous causes of diffuse hyperpigmentation. The most common include metabolic causes and medications. When approaching a patient, especially those with skin of color, it is paramount to thoroughly document via history and physical, the timing, onset, and duration of symptoms. More importantly, it can be difficult to differentiate diffuse hyperpigmentation in a patient of ethnic skin background, mainly because you have to differentiate the patients “native” or “normal” pigment, and the abnormal skin color.
Metabolic causes of hyperpigmentation include vitamin deficiencies, such as vitamin B12 and folic acid. Checking laboratory studies for those vitamins in addition to serum cortisol, adrenocorticotropic hormone (ACTH), thyroid function, and iron.
A detailed medication history should be obtained on all patients, especially those with skin of color, who present with hyperpigmentation. First and foremost, discontinue the offending agent, and only then can an appropriate treatment algorithm for the specific patient be considered.
Although not as common, many cases of malignancy, especially related to melanoma, have been known to cause diffuse hyperpigmentation. This is more common in patients with metastatic disease and/or those patients who unfortunately present with melanoma of an unknown primary origin. Skin of color patients present an even tougher challenge in that they are often diagnosed late in the disease process and/or go undiagnosed for a longer period of time than perhaps an individual with a lighter skin type. Therefore, appropriate screening and management in patients with skin of color is extremely important. Finally, consider autoimmune and infectious etiologies as causes of hyperpigmentation, specifically the cutaneous changes of systemic sclerosis, human immunodeficiency virus, POEMS syndrome, and porphyria cutanea tarda.
Both localized and diffuse hyperpigmentation share the same basic pathogenesis, which, though not yet fully elucidated, is generally understood to involve inflammatory mediators, such as prostaglandins (including PGE2) and leukotrienes (including LTC4 and LTD4). These have been shown to stimulate epidermal melanocytes, which in turn produces a disruption in the skin’s basal layer. This leads to dermal deposition of melanin and subsequent macrophage activation.
Treatment Options for Localized Pigmentation
First and foremost, it is essential to identify and treat any underlying dermatoses. This means if a patient has seborrheic dermatitis and melasma, for example, it is extremely important to clear the seborrheic dermatitis first prior to pursuing aggressive pigmentary therapeutics. This is especially important because a number of dermatoses, especially facial conditions, can cause postinflammatory hyperpigmentation (PIH). By not addressing a concomitant problem, you risk ineffectively treating the overall improvement of skin quality and clearing the hyperpigmentation. It goes without saying that an emphasis on sun protection must be central to any discussion dealing with treating hyperpigmentation. Patients must use sunscreens, preferably containing physical blockers such as titanium dioxide or zinc oxide, on all sun-exposed skin on a daily basis. Chemical sunscreens, though very effective, can rarely cause an allergic contact or irritant contact dermatitis in patients with skin of color, which itself can cause PIH, thus further exacerbating the overall darkening of the skin. Additionally, patients should practice ultraviolet (UV) avoidance through the use of physical barriers, such as hats and clothing that will reduce exposure.
In the case of melasma or PIH, topical treatment options include retinoids, azelaic acid, hydroquinone, chemical peels, and cosmeceuticals. Reassurance and time are also essential elements of the treatment regimen that are sometimes overlooked by the physician and the patient.
Hydroquinone remains a workhorse of melasma and hyperpigmentation management and is often considered the topical “gold standard”. The supervised use of prescription topical hydroquinone had no more than a theoretical risk of malignancy, developing ochronosis, or other long-term safety side effects. There is no substantial evidence to prove carcinogenicity. Importantly, unsupervised use of hydroquinone and use of unapproved formulations is reportedly linked to ochronosis and unwanted side effects. Therefore, patient education is crucial. Take time to assure patients of the safety of the prescription agent you recommend—when used as you direct—and describe clearly the intended duration of therapy. Ideally, patients will not fear the use of hydroquinone, but they will have a healthy respect for the agent, reducing the risk for abuse and misuse.[1]
The selection of a particular retinoid may depend on the preference of the prescriber or patient. Recent research suggests that tazarotene 0.1% cream may offer better efficacy than adapalene 0.3% gel for the management of PIH.[2]
Findings come from a controlled, blinded trial involving 180 subjects with PIH related to acne. Investigators evaluated improvement of both PIH and acne among subjects, which included African Americans, Asians, and Hispanics. While 20 percent of patients in the tazarotene 0.1% cream group had complete resolution at Week 16, only seven percent of patients in the adapalene 0.3% gel group achieved complete resolution at this point.[3]
Another topical treatment option is azelaic acid (AzA), which may offer optimal benefit when combined with a topical corticosteroid. In a prospective, single-blinded, right/left comparison study, 40 Indian patients with melasma were instructed to apply AzA cream 20% to one half of the face for 24 weeks and to apply clobetasol 0.05% for eight weeks followed by AzA cream 20% for the next 16 weeks. Sequential therapy was associated with more significant improvement than monotherapy (p<0.01).[4]
Triple combination fixed therapy (fluocinolone acetonide 0.01%, hydroquinone 4%, tretinoin 0.05%) has become a standard intervention as well, with evidence suggesting that the combination is more effective than hydroquinone monotherapy. In a multicenter, randomized, controlled trial of Southeast and East Asian subjects (n=260), 129 individuals were assigned to the triple combination group, and 131 were assigned to treatment with hydroquinone alone. During the eight-week study, assessments of melasma (Global Severity Score [GSS], Melasma Area and Severity Index score [MASI]) and patient satisfaction were made. Triple combination therapy offered superior efficacy to monotherapy in GSS and other variables, although it was associated with more adverse effects.[5]
Newer cosmeceutical products have also been developed in recent years and have shown promising efficacy in treating hyperpigmentation. One such example was published in a 2013 study. The recent publication described efficacy and tolerability of three new skin brightener formulations containing SMA-432, a prostaglandin E2 inhibitor, compared with 4% hydroquinone. In this randomized, double-blind, half-face study that was conducted in female subjects with moderate-to-severe facial hyperpigmentation, SMA-432 exhibited a dose-dependent improvement in hyperpigmentation, and patient satisfaction was high with this newer product. Study participant questionnaires revealed 79 percent of patients reported improvement in the evenness of skin tone after 12 weeks; 95 percent reported improvement in overall skin condition after 12 weeks.[6] Numerous case reports and studies have been performed over the last decade highlighting the use of products, such as zinc, arbutin, kojic acid, vitamin C base compounds, and green tea extracts, as newer therapies for treating melasma patients. One prime example of a newer novel therapy for melasma that has recently appeared in the literature demonstrates the effects of topical methimazole. Topical methimazole is a potent peroxidase inhibitor under investigation for the management of hyperpigmentation. Peroxidase is important in the final steps of melanogenesis and in some tyrosinase free cells. Even at high concentrations, methimazole is not melanocytotoxic.[7] Kasraee et al showed 20 patients with no thyroid-stimulating hormone (TSH), free thyroxine, or free iodothyronine levels. The drug is odorless and very well tolerated. Another recent study from the European literature describes the use of 4-n-butylresorcinol as an effective treatment option for topical hyperpigmentation management. Similar to hydroquinone, 4-n-butylresorcinol is also a tyrosinase inhibitor.[8] Although more randomized, controlled, large cohort trials are needed to further elucidate the role of products, such as methimazole, zinc, arbutin, and others, these recent studies give hope to patients suffering from melasma that more novel therapies will be available for the treatment of this often devastating condition.
Procedures
Superficial chemical peels are generally effective for the management of PIH and melasma when properly applied. Standard options include glycolic acid 20–70%, salicylic acid 20–30%, trichloroacetic acid (TCA) 10–25%, or Jessner’s solution. Pretreatment with a course of hydroquinone 4% topically (if available) is thought to improve outcomes. Any patient using topical retinoids should discontinue their use for seven days prior to the peel. They may continue to use a noncomedogenic, sun protection factor (SPF) moisturizer.
Support for the use of glycolic acid peels comes from a study that involved 19 subjects randomized to apply a twice-daily regimen of 2% hydroquinone/10% glycolic acid gel, along with tretinoin 0.05% cream nightly or to undergo six consecutive glycolic acid peels (up to 68%) with no additional topical therapy. Overall, patients treated with peels alone showed a trend for more rapid and greater improvement.[9]
Salicylic acid peels have been shown useful in PIH, including for patients with darker skin types. In an open label trial, 25 patients were treated with five salicylic acid peels (20–30% concentration) provided at two-week intervals. Patients underwent two weeks of pretreatment with hydroquinone 4%. Four out of five patients with Fitzpatrick type V or VI had greater than 75-percent improvement in pigmentation.[10]
Laser therapy can be effective for hyperpigmentation with durable improvement. In one study of 27 female subjects, phototypes II to V, with mixed-type melasma refractory to previous therapies, low-fluence Q-switched Nd:YAG laser treatment was provided at 1.6 to 2J/cm2 with 5 or 6mm spot immediately following microdermabrasion. Daily application of a broad-spectrum sunscreen began immediately post-procedure. Additionally, subjects used a topical skin care regimen of hydroquinone with tretinoin or vitamin C. Treatments were repeated at four-week intervals. Most subjects showed more than 50-percent clearance of melasma one month after the first treatment. Side effects were limited to mild post-treatment erythema, which developed after the microdermabrasion and lasted approximately 30 to 60 minutes. Four subjects noted temporary exacerbation of melasma after inadvertent sun exposure, but this resolved within several weeks of resuming the topical skin care regimen. Remission lasted at least six months.[11]
In another study by Lee et al who evaluated the 1927nm thulium fiber fractional laser for patients with melasma, showed significant improvements in MASI scores and patient satisfaction with their outcomes. The split-face study where 25 patients underwent three consecutive laser treatments on half of the face also showed improvements of melasma on routine skin histology, which was noted.[12]
Clearly, many of the studies that use laser therapy for melasma and other forms of hyperpigmentation have small cohort sizes, which itself can be a limitation of the study. In addition, long-term follow-up past 6 to 9 months is needed for these patients to better evaluate risk of relapse. However, with the continued advent of new laser technology, these and other studies are helping clinicians make better and more effective therapeutic treatment plans for patients with skin of color.
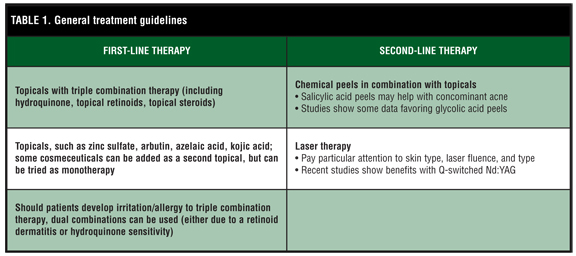
General Guidelines
In order to identify any underlying causes of hyperpigmentation or identify any factors that may hinder treatment, it is essential to obtain a detailed medication history for all patients. It is also important to assess any family history and/or personal history of melasma. If the patient has been treated for melasma in the past, ascertain what therapies were used and how the patient responded.
Allergic reactions to cosmetics and/or fragrance-based products may contribute to PIH. Consider patch-testing when there is suspicion for allergy.
Serial photography is essential in the clinical management of hyperpigmentation. Take good baseline photos and track response throughout the treatment process. Establish protocols for image capture to ensure quality over time. Use a simple, dark background that is non-distracting. These images can be especially helpful when patients think treatment is not working.
Convey to patients that you empathize with them, which will increase your credibility and rapport dramatically. Finally, a biopsy may be indicated if there is any question about the diagnosis. A 2mm punch biopsy will elucidate dermal versus epidermal versus other processes that may be occurring.
References
1. Nordlund JJ, Grimes PE, Ortonne JP. JEADV. 2006;20:781–787.
2. Tanghetti E, Harper JC, Oefelein MG. J Drugs Dermatol. 2012;11(12):1417–1421.
3. Taylor S, Grimes P, Lim J, et al. J Cutan Med Surg. 2009;13(4):183–191.
4. Sarkar R, Bhalla M, Kanwar AJ. Dermatology. 2002;205(3):249–254.
5. Chan R, Park KC, Lee MH, Lee ES. Br J Dermatol. 2008;159(3):697–703.
6. Makino ET, Mehta RC, Garruto J, et al. J Drugs Dermatol. 201312(3):s21–s26.
7. Malek J, Chedraoui A, Nikolic D, et al. Dermatol Ther. 2013;26(1):69–72.
8. Kolbe L, Mann T, Gerwat W, et al. J Eur Acad Dermatol Venereol. 2013;27(Suppl 1):19–23.
9. Burns RL, Prevost-Blank PL, Lawry MA, et al. Dermatol Surg. 1997;23(3):171–174.
10. Grimes PE. Dermatol Surg. 1999;25(1):18–22.
11. Kauvar AN. Successful treatment of melasma using a combination of microdermabrasion and Q-switched Nd:YAG lasers. Lasers Surg Med. 2012;44(2):117–124.
12. Lee HM, Haw S, Kim JK, et al. Dermatol Surg. 2013;39(6):879–888.