Michael H. Gold, MD, Gold Skin Care Center, Nashville, Tennessee, Tennessee Clinical Research Center, Nashville, Tennessee; Bruce E. Katz, MD, Juva Skin & Laser Center, New York, New York; Joel L. Cohen, MD, AboutSkin Dermatology and DermSurgery, Englewood, Colorado; Julie Biron, Tennessee Clinical Research Center, Nashville, Tennessee
Disclosure: Dr. Gold performs research for Neocutis, is a consultant for and speaks on behalf of Neocutis, and is a shareholder in the company. Dr. Katz reports no relevant conflicts of interest. Dr. Cohen has participated as a clinical research investigator for Neocutis. Ms. Biron reports no relevant conflicts of interest. This study was funded by Neocutis, Inc., San Francisco, California.
Abstract
The present study investigated the use of a novel hyaluronic acid serum in combination with a cream comprising a mixture of human growth factors in conjunction with the micro laser peel procedure for skin rejuvenation. After preconditioning the face with the hyaluronic acid serum followed by the cream twice daily for one month, 15 female volunteers between 35 to 65 years of age with demonstrable facial wrinkling received a micro laser peel on the entire face using an erbium-doped yttrium aluminium garnet laser. Immediately following the laser procedure, the subjects applied the test products twice daily until the second laser peel one month later. Immediately following the second procedure, the subjects reapplied the test products for another month. In the large majority of subjects, erythema or edema, crusts or erosions, and transitory stinging or burning sensations after the micro laser peel were minimal or mild when the skin was treated with the serum followed by the cream. The micro laser peel in conjunction with the test products helped to significantly improve hyperpigmentation, wrinkles, and texture as compared to before treatment. This study with the micro laser peel device demonstrated that a novel hyaluronic acid serum combined with the human growth factor cream can be successfully used for skin rejuvenation in conjunction with light-to-medium invasive laser skin treatments.
(J Clin Aesthet Dermatol. 2010;3(12):37–42.)
Today, a large variety of cosmetic procedures including light and laser therapies are used for nonsurgical skin rejuvenation.[1–3] The field of nonsurgical skin rejuvenation has been inspired by patient expectations for minimal risk and rapid recovery.[1] The recovery time for nonsurgical skin regeneration depends on the procedure; generally there is minimal downtime after nonablative treatments and significant downtime after ablative procedures, such as CO2 laser resurfacing. Earlier studies indicate that topical skincare regimens can be beneficial in reducing postprocedure symptoms.[4] With the goal to assess a topical skin care regimen that would reduce procedure-related signs and possibly enhance outcome of the procedure, the present study reports on a skin care regimen consisting of the combined application of a high content hyaluronic acid serum with a cream containing a mixture of human growth factors and cytokines. A slightly invasive laser procedure for skin rejuvenation, known as a micro laser peel, was performed; the device was adjusted to remove up to 20µm of skin. This erbium-doped yttrium aluminium garnet (Er:YAG) laser is an adjustable, minimal-to-full, epidermal, laser peel that removes the outermost layers of the skin as a function of the laser settings. Depending on skin removal and the patient, adverse events are commonly limited to transitory erythema, edema, crusts and erosions lasting for several days after the laser procedure.[5]
The serum was formulated with 1% high molecular weight (about 1000kDa), pharmaceutical grade, bioengineered hyaluronic acid, while the human growth factor and cytokine mixture was obtained through a biotechnology process using cultured human fetal fibroblasts. The fibroblasts originated from a dedicated cell bank, which was established for the development of wound healing products. The test cream with the growth factor and cytokine mixture has previously been studied for the treatment of adverse events associated with photodynamic therapy.[6] Furthermore, the cream was intensively studied as effective skin care regimen for aged facial skin when used alone[7–9] and was reported to be beneficial in scar management after surgery.[10]
Hyaluronic acid (HA; also known as hyaluronate or hyaluronan) is a high molecular weight, negatively charged (polyanionic) polysaccharide and is naturally present in virtually all vertebrate tissues and fluids including the skin’s extracellular matrix. Through its complex interactions with matrix components and cells, HA has versatile roles in skin related to both its physicochemical and biological properties. HA is well known for its excellent water-holding capacity.[11] Further, HA supports tissue architecture of extracellular matrix, governs skin elasticity, is involved in cell migration and differentiation processes during wound healing and inflammation, and might act as an antioxidant due to restriction of movement of reactive oxygen species.[12] There is also some evidence that HA and growth factors (i.e., fibroblast growth factor) act synergistically to accelerate healing.[13] HA was shown to interact with growth factors, thereby protecting them from degradation by proteases.[14] Finally, HA is used as a topical drug delivery system for localized delivery of certain drugs to the skin.[15] Therefore, due to HA’s specific properties in relation to growth factors, topical products with concentrated HA in combination with human growth factors might be particularly well suited to help improve recovery and outcome after cosmetic light and laser therapies.
METHODS
Study design. The three-center study was conducted according to the Declaration of Helsinki as approved by the Independent Institutional Review Board (Plantation, Florida). After obtaining informed consent, [15] Caucasian, female volunteers between 35 and 65 years of age, in good general health, not nursing or pregnant, of Fitzpatrick skin type 1 to 4, and with moderate-to-severe facial photodamage underwent the treatment regimen. Excluded were subjects with any active or history of skin disease affecting the face; subjects who received microdermabrasion, glycolic or less than 20% trichloro acetic acid (TCA) peel, or hydroquinone-containing products on the face within one month prior to the beginning of the study; subjects who received nonablative laser, light, or radio-frequency treatments within three months prior to the beginning of the study; and subjects who received retinoids, dermabrasion, or greater than 20% TCA peel, Botox®, or filler injection, or ablative laser or cosmetic surgery within six months prior to the beginning of the study.
Micro laser peel. The subject received two micro laser peels (MicroLaserPeel™ Profile Contour 2940nm Er:YAG laser system; Sciton, Palo Alto, California) separated by one month on entire face adjusted to up to 15µm during the first treatment and up to 20µm during the second treatment. Topical 5% lidocaine (LMX 5 Cream; Ferndale Laboratories, Ferndale, Michigan) was provided 30 minutes prior to treatment.
Micro laser peel skin care regimen. The subjects applied a 1% sodium hyaluronate serum (Hyalis; Neocutis, San Francisco, California) followed by an oil-in-water-based skin cream containing a proprietary mixture of human growth factors and cytokines called processed skin cell proteins (Bio-Cream—Bio-restorative Skin Cream with PSP®, Neocutis) one month prior to the laser peel in order to condition the skin before the procedure and after each laser peel for a total of two months twice daily (morning and evening). Before the application of the test products, the subjects were asked to cleanse the skin using a gentle cleanser (Cetaphil® Gentle Skin Cleanser, Galderma Laboratories, Fort Worth, Texas). During the daytime, when sun protection was required, the subjects were additionally asked to use a sun protection factor (SPF) 45 sunscreen (Coppertone® Oil Free Sunsceen Lotion SPF 45; Schering-Plough HealthCare Products, Memphis, Tennessee). Gentle cleanser and sunscreen were also provided to the subjects at the beginning of the study.
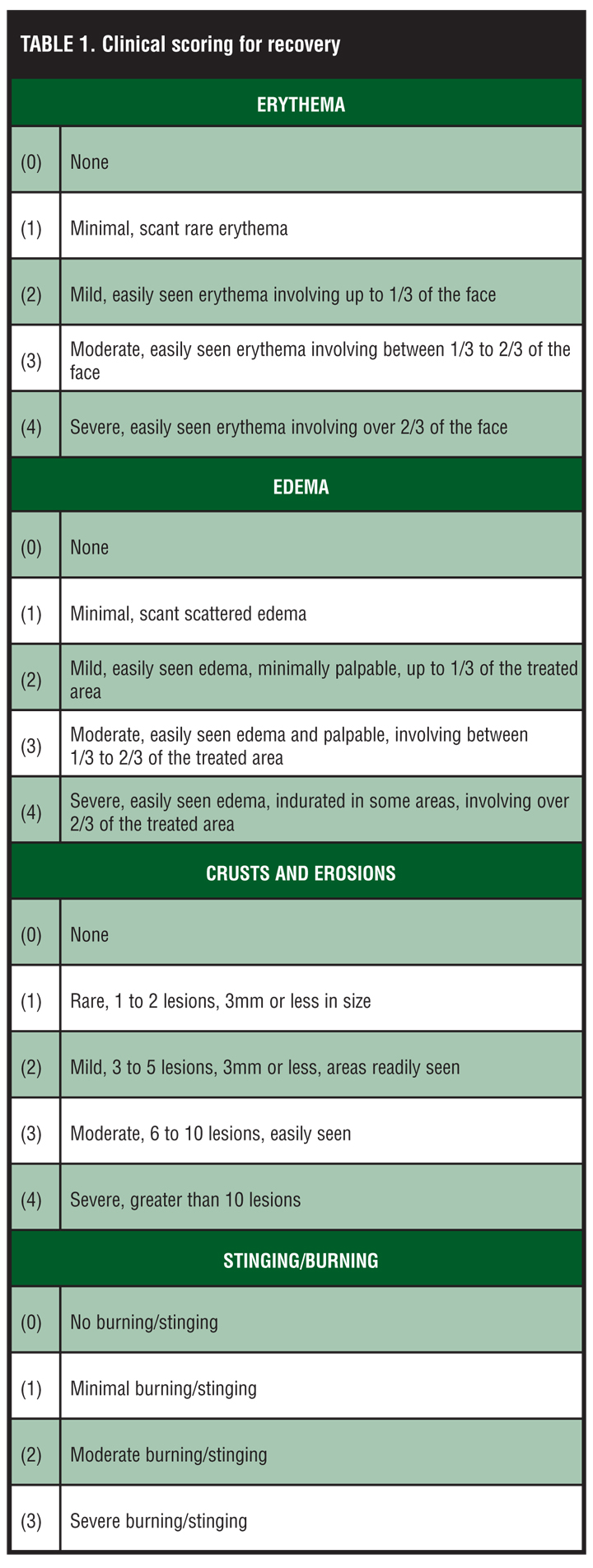
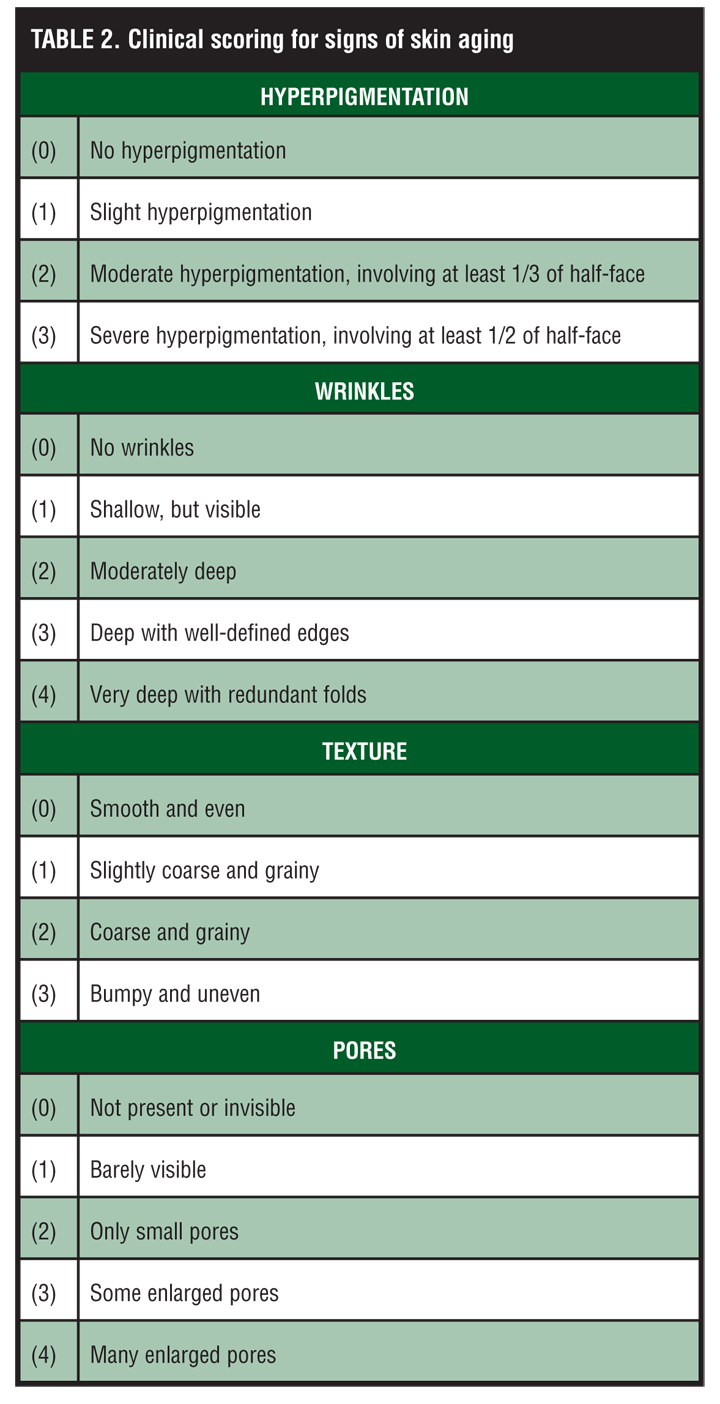
Evaluations. Clinical assessment of recovery (erythema, edema, crusts, and erosions) and improve-ment of signs of skin aging (hyperpigmentation, wrinkle, texture, pore) were assessed using 0 to 3 or 0 to 4-point visual scoring systems (Table 1 and Table 2). In addition, clinical photography was taken under standardized conditions before, three days after the micro laser peels, and at the end of the study period using the OMNIA imaging system (Canfield Scientific; Fairfield, New Jersey). Subjects were further asked whether they tolerated the test products well, whether the products helped to keep skin moist, soothe or calm skin, or reduce general discomfort (pain, burning, stinging, etc.) after the micro laser peel. Possible answers were “Yes,” “Not sure, but seems likely,” or, “No.”
{kind=link}
{kind=link}
RESULTS
All 15 subjects averaged 51±9 years of age (between 36 to 64 years) completed the study. One subject, however, refused to undergo the second micro laser peel since she felt that downtime after the procedure was significant and not acceptable. This subject remained in the study and continued using the test products, but did not receive a second micro laser peel. One subject missed the evaluation three days after the second laser peel (Day 33).
Adverse events and tolerability. The subjects did not experience any adverse events in relation to the test products. One subject had severe periorbital edema occurring one day after the first laser procedure (15 joules). This adverse event was related to the micro laser peel procedure and not to the study products. While the use of the test products was continued, the edema reaction resolved after about five days using ice cooling without any medicinal intervention. This subject tolerated the second laser peel, which was set at a lower laser intensity (10 joules), without the occurrence of any adverse events. One subject developed asthma and one subject a tooth and root canal abscess during the study period; both adverse events were not related to the study products or the laser procedure.
Eighty-seven percent of the subjects after the first peel, and 91 percent after the second peel reported to tolerate the test products well when used starting immediately after the laser procedure for three days. The few subjects who did not report tolerating the test products well mentioned slight stinging or burning sensations after application of the test products. The questionnaire did not allow distinguishing whether the HA serum, the growth factor and cytokine skin cream, the cleanser, or the sunscreen were the cause of these transitory sensory sensations. All subjects (100%) reported to tolerate the test products well one month after each procedure.
Clinical assessment of recovery. On average, erythema was mild involving up to one-third of the face (corresponding to score 2), whereas edema was minimal, scant rare (score 1) three days after the micro laser peel. After the peel, mild crusts and erosions were readily seen (3–5 lesions of 3mm or less; score 2). With the exception of some minimal, scant rare erythema (score 1) seen in 27 percent of subjects after the first peel and 40 percent after the second peel, edema and crusts and erosions completely disappeared within one month after the procedure in all subjects. As judged from the slightly decreased intensity of erythema, edema, and crusts and erosions, the second peel appeared to be better tolerated despite the fact that the subject generally received a more intense peel removing up to 20µm. The detailed results are shown in Figure 1.
{kind=link}
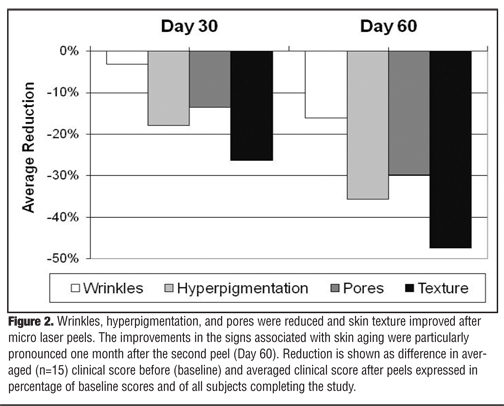
Clinical assessment of signs of skin aging. Wrinkles, hyperpigmentation, and pores were reduced, and skin texture improved after the micro laser peels (Figure 2). The improvements in the signs associated with skin aging were particularly pronounced one month after the second peel (Day 60). In average, signs of wrinkles were reduced by 16 percent, pores by 30 percent, and hyperpigmentation by 36 percent, whereas texture improved by 45 percent as compared to baseline after the two-month study period. These improvements are illustrated in the photographs of one subject taken before and at the end of the study period (Figure 3).
{kind=link}
{kind=link}
Subject questionnaires. Eight or more out of 10 subjects (?80%) reported that test products helped or seemed likely to help keep skin moist, sooth or calm skin, and reduce general discomfort after the first and second laser peel. Furthermore, when asked at the end of the study, 90 percent of subjects responded favorable or very favorable toward using the test products again when undergoing another micro laser peel in the future.
COMMENT
Appropriate skin care in conjunction with cosmetic procedures, such as light and laser therapies, represents an important aspect in nonsurgical skin rejuvenation by helping to minimize downtime and enhance outcome of the procedures. This study with the micro laser peel device suggests that the use of a combination of a high content (1%), high molecular weight and pharmaceutical grade hyaluronic acid skin serum with an oil-in-water cream containing a proprietary mixture of human growth factors and cytokines is generally well tolerated and can be successfully used for postprocedural skin care after cosmetic and dermatological procedures, such as light-to-medium invasive laser skin treatments. The properties of hyaluronic acid that protect growth factors from degradation by proteases,[14] may make the use of hyaluronic acid and growth factor topical products an especially promising combination for treating open skin wounds where protection of growth factors from protease activity can be beneficial.[16] This hypothesis remains to be confirmed in additional, placebo-controlled studies since no active control group was used in this initial series of patients. This will further determine the potential benefits of the treatment regimen versus other treatment modalities and skin care routines.
References
1. Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: nonablative, fractional, and ablative laser resurfacing. J Am Acad Dermatol. 2008;58:719–737.
2. Gold MH. Photodynamic therapy with lasers and intense pulsed light. Facial Plast Surg Clin North Am. 2007;15:145–160.
3. Goldberg DJ, Amin S, Russell BA, et al. Combined 633-nm and 830-nm led treatment of photoaging skin. J Drugs Dermatol. 2006;5:748–753.
4. Garcia BD, Goldman MP, Gold MH. Comparison of pre- and/or postphotodynamic therapy and intense pulsed light treatment protocols for the reduction of postprocedure-associated symptoms and enhancement of therapeutic efficacy. J Drugs Dermatol. 2007;6:924–928.
5. Hantash BM, De Coninck E, Liu H, et al. Split-face comparison of the erbium micropeel with intense pulsed light. Dermatol Surg. 2008;34:763–772.
6. Gold MH, Biron J. A novel skin cream containing a mixture of human growth factors and cytokines for the treatment of adverse events associated with photodynamic therapy. J Drugs Dermatol. 2006; 5:796–798.
7. Gold MH, Goldman MP, Biron J. Efficacy of novel skin cream containing mixture of human growth factors and cytokines for skin rejuvenation. J Drugs Dermatol. 2007;6:197–201.
8. Gold MH, Goldman MP, Biron J. Human growth factor and cytokine skin cream for facial skin rejuvenation as assessed by 3D in-vivo optical skin imaging. J Drugs Dermatol. 2007;6:1018–1023.
9. Hussain M, Phelps R, Goldberg DJ. Clinical, histologic, and ultrastructural changes after use of human growth factor and cytokine skin cream for the treatment of skin rejuvenation. J Cosmet Laser Ther. 2008;10:104–109.
10. Personal communication by Neocutis, Inc., September 1st 2009.
11. Laurent TC, Fraser JR. Hyaluronan. FASEB J 1992;6: 2397–2404.
12. Weindl G, Schaller M, Schäfer-Korting M, et al. Hyaluronic acid in the treatment and prevention of skin diseases: molecular biological, pharmaceutical and clinical aspects. Skin Pharmacol Physiol. 2004; 17:207–213.
13. Radomsky ML, Thompson AY, Spiro RC, et al. Potential role of fibroblast growth factor in enhancement of fracture healing. Clin Orthop Relat Res. 1998; 355 Suppl:S283–S293.
14. Locci P, Marinucci L, Lilli C, et al. Transforming growth factor beta 1-hyaluronic acid interaction. Cell Tissue Res. 1995; 281:317-324.
15. Brown MB, Jones SA. Hyaluronic acid: a unique topical vehicle for the localized delivery of drugs to the skin. J Eur Acad Dermatol Venereol. 2005; 19:308–318.
16. Braund R, Hook S, Medlicott NJ. The role of topical growth factors in chronic wounds. Curr Drug Deliv. 2007; 4:195–204.