Jacquelyn Levin, DO; James Q. Del Rosso, DO, FAOCD; Saira B. Momin, DO
Dr. Levin is from the Mohave Skin & Cancer Clinics, Dermatology Research Center, Las Vegas, Nevada; Dr. Del Rosso is Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada; Dr. Momin is Chief Dermatology Resident (PGY-4), Valley Hospital Medical Center, Las Vegas, Nevada.
Disclosure: Dr. Levin was a previous employee of and is a consultant to Guthy-Renker Corporation. Drs. Del Rosso and Momin report no relevant conflicts of interest.
Abstract
To date, we are unaware of a review that has investigated common cosmeceutical ingredients in order to answer the three specific questions proposed by the father of cosmeceuticals, Dr. Albert Kligman. It is the goal of this review to gather all the published scientific data on five common cosmeceutical ingredients, answer the three major questions about the scientific rationale for their use, and ascertain how much we really know about consumers’ favorite cosmeceutical ingredients.
Most of the research concerning cosmeceutical retinoid ingredients is based upon the effects of retinoic acid on the skin. Clinical trials concerning retinol and retinaldehyde are scant and lacking in statistical evaluation for significance. There is research substantiating the effects of kinetin in plants and also in-vitro antioxidant effects. However, proof of anti-aging activity remains elusive, and the clinical efficacy of kinetin is based on limited data. Niacinamide is the ingredient investigated that most closely upholds the “Kligman standards” of cosmeceutical-ingredient analysis. With the available scientific evidence on topical niacinamide, clinicians are able to adequately answer questions about permeability, mechanism, and clinical effect. Both green tea and soy have been popularized commercially based on their antioxidant effects, yet there is a paucity of clinical studies concerning their efficacy as topical anti-aging agents. It may be that soy and green tea are better at preventing the signs and symptoms of skin aging than actually reversing them. Since cosmeceutical products are claiming to therapeutically affect the structure and function of the skin, it is rational and necessary to hold them to specified scientific standards that substantiate efficacy claims.
Introduction
Increasingly, patients are looking for cost-effective noninvasive methods to improve the appearance of their skin. Many patients are turning away from prescription medications and medical procedures and are instead considering over-the-counter (OTC) treatments, such as cosmeceuticals. Factors that cause patients to switch to OTC products include lack of adequate insurance coverage for prescription products used to treat photoaging, the need to pay for physician visits to obtain prescription products, and failure to discern “fiction from fact” related to unsubstantiated claims made by some OTC anti-aging skin care products. A cosmeceutical product by definition is a cosmetic product in which the active ingredient is meant to have a beneficial physiological effect due to an enhanced pharmacological action when compared with an inert cosmetic.[1]
Every day in clinical practice, dermatologists see patients who ask them if cosmeceutical products are beneficial. Accurate advice is a challenge that requires knowledge of the structure and function of human skin and the available scientific data, which may or may not support the efficacy of a given cosmeceutical product. As dermatologists, it is very hard for us to keep up with the latest evidence on the popular cosmeceutical ingredients due to the vastness of ingredients, the multitude of commercially available products and their efficacy claims, and the validity or accuracy of data gleaned from in-vitro and clinical studies, if available.
What questions need to be asked when scientifically evaluating the potential therapeutic merits of a cosmeceutical?
According to Dr. Albert Kligman, when asked to evaluate a new cosmeceutical product that claims a beneficial physiological effect, it is important to ask three questions:
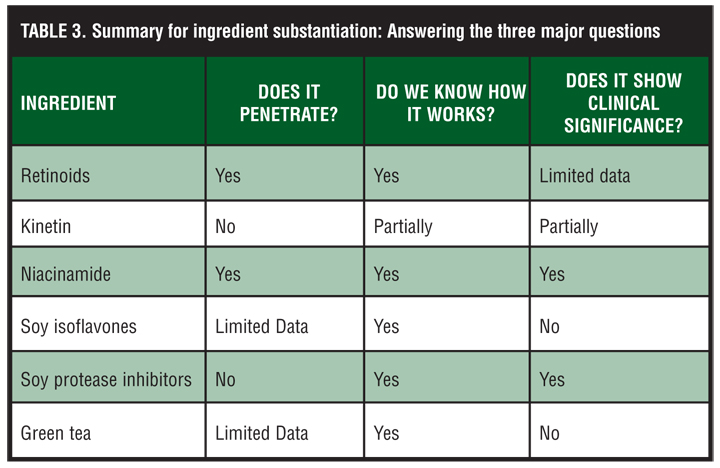
1. Can the active ingredient penetrate the stratum corneum (SC) and be delivered in sufficient concentrations to its intended target in the skin over a time course consistent with its mechanism of action?
2. Does the active ingredient have a known specific biochemical mechanism of action in the target cell or tissue in human skin?
3. Are there published, peer-reviewed, double-blind, placebo-controlled, statistically significant, clinical trials to substantiate the efficacy claims?[1] (Table 1.)
To date, we are unaware of a review that has investigated common cosmeceutical ingredients in order to answer these three specific questions. It is the goal of this review to gather the available published scientific data on five common cosmeceutical ingredients, to answer the three major questions described above, and to ascertain how much we really know about our consumers’ favorite cosmeceutical ingredients.
The first question addresses whether the active ingredient penetrates the SC. The SC is an effective barrier to transepidermal water loss (TEWL) and to the penetration of exogenous substances. Typically, the substances that cannot penetrate the SC easily include: proteins, sugars, peptides and nucleic acids with molecular weights greater than approximately 1000kDa, and highly charged molecules.[1]
{kind=link}
In addition, it is important to determine if the ingredient is delivered in sufficient concentrations to its intended target in the skin to produce the desired effect. The minimum concentration of ingredient required to produce the desired effect is termed the threshold concentration and is important for evaluating cosmetic formulas.
If the agent meets the first criterion, that is penetration of the SC in an amount exceeding the threshold concentration, the second question follows intuitively. The second question asks if there is a known biochemical or pharmacological mechanism of action for this active ingredient to substantiate the marketing claim. Most pharmacologically active ingredients have mechanisms of action on cellular components that regulate physiological functions (i.e., inhibition or activation of enzymes involved in signal transduction or gene expression).[2] Surprisingly, some popular cosmeceutical ingredients have mechanisms that are currently unknown and require further research. If a viable biochemical or pharmacological mechanism of action exists, and the product can reach its target at sufficient concentrations for a long enough duration, the product deserves further clinical experimentation, preferably a randomized, double-blind, vehicle-controlled clinical trial.
Clinical trials should include the use of noninvasive instrumentation, which measures characteristics such as TEWL, corneometry, skin elasticity, colorimetry, surface replica analysis, and other techniques that can be used to assess efficacy claims. Pretreatment and post-treatment photography alone are not adequate because there are major pitfalls in standardized clinical photography. In addition, it is difficult to measure appearance clinically because it is highly subjective and endpoints are difficult to establish. The pitfalls of published clinical trials to date are that many of the reports are anecdotal, have been performed on small groups of patients, and statistical significance has not been well established.
Another way to demonstrate the effects of a product is histology. The histological changes of photoaged skin are well documented. Demonstration of reversal of histological features of photoaging is another approach to substantiate efficacy claims for the reversal of photoaging.[3]
This next section presents a summary of the published scientific data of five popular cosmeceutical ingredients. Specifically, this article reviews the evidence on penetration of the SC, the mechanism of action, and the anti-aging effects on skin based on clinical studies.
What background information is available on cosmeceutical retinoids?
Retinoids consist of natural and synthetic derivatives of vitamin A that can be found in both prescription medications and OTC cosmeceuticals. Retinoic acid (RA) as well as the synthetic napthalene derivatives adapalene, tazarotene, and bexarotene are registered prescription drugs. The topical cosmeceutical retinoids include retinyl esters, retinol, retinaldehyde, and the group of oxoretinoids.[4]
RA has been extensively studied and used as an effective topical treatment for photoaging, acne, and numerous other dermatological disorders. RA can, however, be irritating to the skin, limiting its use in some patients. Retinol (ROL) and retinaldehyde (RAL) are of interest to the scientific community and cosmetic industry as gentler yet still effective alternatives to RA. However, the other cosmeceutical retinoids, retinyl palmitate and retinyl-acetate, are retinoid esters and are not considered effective against photoaging and therefore are not discussed in this review.[4,5]
In the skin, ROL is oxidized into RAL, which in turn is oxidized into RA, the biologically active form of vitamin A. Topical cosmeceuticals containing ROL and RAL are theoreticized to work because once absorbed they are metabolized to RA, which induces pharmacological activity. Given this consideration, not only is the percutaneous absorption profile of ROL and RAL important to its effectiveness, but the metabolism of ROL and RAL to RA is just as important.
What data is available on the percutaneous absorption and metabolic activity of retinoids?
In general, retinoids are lipophilic molecules that can penetrate the epidermis.[6] One study demonstrated the specific penetration characteristics of ROL and RAL in human skin in vivo by measuring levels of the skin enzyme cytochrome P-450-dependent RA 4-hydroxylase (CP450-RAH) (Table 2a).[7] The enzyme CP450-RAH is induced by presence of RA in the skin and therefore its induction can be used as an indicator of ROL and RAL penetration and metabolism to RA. The study found a significant induction in this enzyme following topical application of ROL and RAL to human skin in vivo. After 48 hours of occlusion, both ROL and RAL (0.025% and greater) increased the enzyme activity significantly while lower concentrations did not cause significant induction.[7] Interestingly, the increase in enzyme induction was not linear and higher doses of ROL and RAL only caused small increases in enzyme activity. However, it should be noted that at lower doses (0.01% and 0.025%), RAL was a greater inducer of CD450-RAH than ROL.[7] Given the results of this study, it seems the threshold concentration for adequate penetration and metabolism of RAL and ROL into RA is 0.025%. Hence, it is important that the concentration of RAL and ROL in cosmetic formularies be at least 0.025%. However, it must also be considered that concentrations above 0.025% may not induce greater penetration or metabolism to RA.
{kind=link}
In another experiment, metabolism of ROL, RAL, and RA was studied utilizing in-vitro human skin and dermal fibroblasts.[8] Radiolabeled ROL and RAL were applied either topically to the skin biopsies or to the culture media of the fibroblast suspension and the metabolites were identified by high-performance liquid chromatography (HPLC) after 24 hours of incubation. The skin cultures demonstrated a gradient distribution of the retinoids within the skin: 75 percent of absorbed activity was in the epidermis, 20 percent in the dermis, and 2 to 6 percent in the culture medium for the three retinoids tested. Of the epidermal extracts, 60 percent of applied ROL remained unmetabolized. The main ROL metabolites in the epidermis were retinyl esters (18.5%), RA (2%), RAL (1.6%), 13-cis-retinoic acid (1%), and polar compounds. The dermis yielded similar metabolites, but a higher proportion of polar compounds. RAL was also metabolized in the epidermis, with 43 percent of the absorbed radioactivity being RAL, 9 percent retinyl esters, 14 percent ROL, and 0.8 percent RA.[8]
Collectively, several studies have therefore demonstrated an absorption and metabolic capacity for topical ROL and RAL.[7,8] Retinyl esters appear to be the major metabolite, while the formation of RA from these substances constitutes a small proportion of the metabolites formed. However, whether this conversion is sufficient for pharmacological activity is unknown. In-vivo studies may better quantify both metabolism and dose-response relationships.[6]
What are the potential mechanisms of action of retinoids?
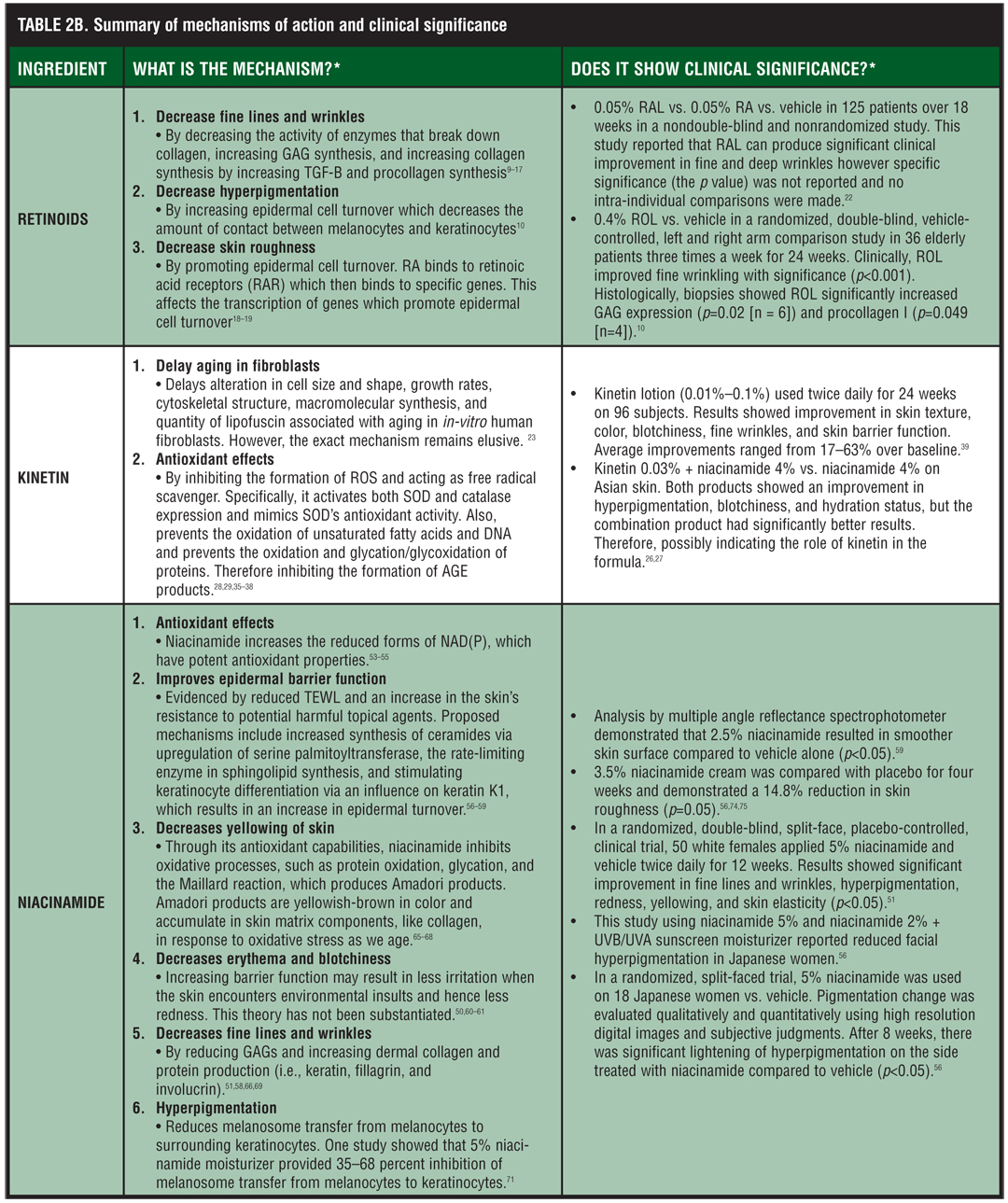
ROL and RAL are metabolized to RA in the skin and therefore, are assumed to exhibit the same mechanism and clinical effects as RA (Table 2b and Table 2b continued). Of these effects, the surface roughness, mottled hyperpigmentation, and fine wrinkles demonstrate the most significant improvement with RA therapy.[9] Although ROL- and RAL-containing cosmeceuticals have not been shown to produce the magnitude of clinical results obtained with the prescription products that are approved and used to treat photoaging (tretinoin, tazarotene), many consumers appear to be pleased with their cosmetic results anecdotally.
{kind=link}
{kind=link}
Hyperpigmentation. RA is thought to reduce mottled hyperpigmentation by enhancing epidermal cell turnover. Enhancing epidermal cell turnover decreases the contact time between keratinocytes and melanocytes and promotes a rapid loss of pigment through epidermopoiesis.[10]
Fine lines and wrinkles. RA therapy reduces fine lines and wrinkles by increasing the capacity of the epidermis to hold water through stimulation of glycosaminoglycan (GAG) synthesis and by stimulating collagen synthesis through increases in transforming growth factor (TGF-beta) and procollagen.[9–12] Furthermore, it is believed that RA may also retard or prevent further dermal matrix degradation by inhibiting the enzymes that break down collagen and preventing oxidative stress.[11,13–17]
Roughness. RA therapy reduces skin roughness by modulating the expression of genes involved in cellular differentiation and proliferation, hence promoting epidermal cell turnover.[9,11] The effects are believed to be mediated through binding to retinoic acid receptors (RAR) and subsequent binding of these complexes to specific genes affecting gene transcription.[18,19]
What clinical studies are available on cosmeceutical retinoids?
There are extensive clinical trials investigating the anti-aging effects of topical RA (Table 2c) (Table 3). RA is considered to be one of most effective and well-substantiated compounds for treating the signs and symptoms of aging and/or photodamaged skin, including fine lines, hyperpigmented spots, and wrinkles.[10,20,21] However, few studies have been reported for the OTC retinoids. Here, the authors present the results of studies investigating the anti-aging effects of RAL and ROL.
{kind=link}
{kind=link}
Some studies have reported that RAL can produce significant clinical improvement in the appearance of fine and deep wrinkles.[10,22] In one study, the efficacy of RAL 0.05% cream for the treatment of photoaging was compared to 0.05% RA and vehicle creams over an 18-week time period.[22] A total of 125 patients (40 in the RA group, 40 in the RAL group, and 45 in the vehicle group) were studied. This study demonstrated that RAL can produce clinical improvement in fine and deep wrinkles.[22] However, statistical significance was not reported and no intra-individual comparisons were made.
Topical ROL has been shown in vivo to have only a modest effect compared with topical RAL and RA while two randomized controlled trials showed a significant improvement in fine wrinkles after 12 and 24 weeks of treatment with the use of ROL versus placebo.[10,23] One of the randomized, controlled trials was completed by Sorg et al[10] who evaluated the effectiveness of topical ROL in improving the clinical signs of naturally aged skin in a randomized, double-blind, vehicle-controlled, left and right arm comparison study.[10] The study population comprised 36 elderly subjects (mean age 87 years) residing in two senior citizen facilities. Topical 0.4% ROL lotion or its vehicle was applied at each visit by study personnel to either the right or the left arm, up to three times a week for 24 weeks. Clinical assessment was made by using a semiquantitative scale and biochemical measurements from skin biopsy specimens. After 24 weeks, there were significant differences between ROL-treated and vehicle-treated sides for fine wrinkling scores (p<0.001). In addition, histology showed ROL treatment significantly increased GAG expression (p=.02 [n = 6]) and procollagen I (p=0.049 [n = 4]) compared with vehicle. This data provided support that topical ROL improves fine wrinkles via its metabolism to RA and subsequent increases in GAGs and collagen production.
What conclusions can be drawn from data on cosmeceutical retinoids?
After sunscreens, many believe topical retinoids are the most important drug class to combat and reverse the signs of aging. With more than two decades of experimentation, there is a vast amount of evidence that regular retinoid use over several months results in clinical improvement in skin texture, wrinkles, and pigmentation.[24] However, most of this knowledge and experience is about prescription products containing RA and not about OTC retinoids, ROL and RAL. Of the limited data available concerning OTC retinoids, RAL seems to be the most efficacious.[10,22] Therefore, those patients who are looking to decrease and or prevent the signs of aging without use of a prescription product should use RAL containing cosmeceuticals as they have the best scientific evidence supporting their efficacy in reducing the signs and symptoms of aging.
So what do we tell our patients concerning retinoid cosmeceuticals? The authors have presented sufficient evidence on cutaneous penetration and concerning mechanism of action and semi-sufficient evidence on the clinical anti-aging effects of ROL and RAL. They believe it is important to remind the patients that while the most effective anti-aging treatment is achieved with prescription retinoids, there is some evidence to support the use of RAL and ROL to decrease fine lines and wrinkles.
What is kinetin (N-furfuryladenine growth factor)?
Kinetin is an essential plant growth hormone that regulates aspects of growth and differentiation, retards leaf yellowing and senescence, and slows down fruit ripening and degeneration.[25,26]
What data is available on the percutaneous absorption of kinetin?
The authors were unable to find any studies investigating the percutaneous absorption of kinetin. However, kinetin has been shown to be nonirritating to the skin, easily formulated, chemically stable, and compatible with other formulation components.[27]
What are the potential mechanisms of action of kinetin?
Kinetin is shown to exert its anti-aging effects in different systems including plants, fruit flies, and cultured human skin fibroblasts.[28–31] Studies on human fibroblasts in vitro have demonstrated that kinetin may have the ability to delay the onset of age-related changes as well as decrease the severity of these changes.[23] These age-related changes include the alteration in cell size and shape, growth rates, cytoskeletal structure, macromolecular synthesis, and quantity of lipofuscin. The delay of age-related cellular characteristics were most pronounced in cultures where kinetin was continuously present. It was noted that some aging characteristics began to reappear upon removal of kinetin, and youthful characteristics in general were better maintained in younger cells compared to older cells. This suggests that continued use of kinetin is necessary to maintain results and that there may be additional benefit to starting kinetin at a younger age.[32] However, the mechanism by which kinetin exerts its effects on human fibroblasts remains elusive.
Antioxidant effects. Investigators have surmised that the mechanism of action that results in age retardation may involve the genes that influence aging and may involve kinetin acting as both an inhibitor of reactive oxygen species (ROS) formation and a scavenger of ROS.[28,33] Many studies have shown kinetin to be a powerful antioxidant. Kinetin has the ability to mimic superoxide dismutase (SOD) activity, activate both SOD and catalase expression, and quench ROS.[28,29,35,36] Also, kinetin has been shown to prevent the oxidation of unsaturated fatty acids and inhibit the in-vitro oxidation of DNA.[36,37] Also, Verbeke et al[38] demonstrated that kinetin can inhibit the oxidation and glycation/glycoxidation of proteins. By inhibiting the oxidation and glycation/glycoxidation of proteins, kinetin inhibits the formation of advanced glycation/glycoxidation end products (AGE). These results strengthen the view that kinetin is a powerful antioxidant with significant biological properties and useful potential for the prevention of oxidative damage.[38]
Other effects. Although clinical studies of topical kinetin have suggested improvement in skin texture, a decrease in hyperpigmentation, and a decrease in TEWL, there appears to be no reported mechanisms for how kinetin improves skin texture, fine wrinkles, hyperpigmentation, and/or the SC permeability barrier.
What clinical studies are available on kinetin?
One open-label study about the clinical safety and efficacy of kinetin 0.1% lotion on human skin was published by McCullough et al.[39] Ninety-six subjects with photodamaged skin showed improvement in the categories of skin texture, color, blotchiness, and fine wrinkles after 24 weeks of twice-daily application of 0.01%, 0.05%, or 0.10% kinetin. Average improvements ranged from 17 to 63 percent over baseline. In addition, the results of this study suggest that kinetin improves barrier function of the SC, as evidenced by a mean decrease in TEWL after 14 weeks of use. Hence, this demonstrated that topical kinetin (0.01%–0.1%) can partially improve some of the clinical signs of mild-to-moderately photodamaged skin, such as skin texture, fine wrinkles, skin color, and blotchiness, and can help restore normal skin barrier function with 12 to 24 weeks of topical application.[39]
Another study investigated the anti-aging effects of topical kinetin 0.03% in combination with niacinamide 4% versus niacinamide 4% alone in Asians. Amasino et al[26] found that the combination of kinetin and niacinamide and niacinamide alone effectively improved many of the facial aging signs in Asians. This combination of ingredients reduced the number of hyperpigmented spots and red blotchiness as well as increased SC hydration status with more persistence than the formula containing niacinamide alone. The authors believe that this indicates a decisive role for kinetin in the formulation and that kinetin plus niacinamide may be used as an adjunctive therapy for anti-aging purposes of the skin.[27]
What conclusions can be drawn from data on kinetin?
In summary, kinetin is a relatively new ingredient in the cosmeceutical world with anti-aging potential given its anti-aging role in plants and its in-vitro antioxidant effects. In order to recommend kinetin, the authors feel that the scientific evidence supporting kinetin is still lacking in permeation studies and mechanistic discoveries as to how this growth factor reduces hyperpigmentation, improves skin barrier function, and improves skin texture. There is modest support of its efficacy based on clinical studies.
What background information is available on niacinamide and nicotinic acid?
While the nutritional value of niacin (vitamin B3) may be well recognized, the skin care benefit of topically applied niacin is a recent discovery based on recently published studies. Niacin (vitamin B3) has two potential forms that can be used in cosmeceuticals: niacinamide (nicotinamide) and nicotinic acid. It is debatable as to whether these two forms of niacin are interchangeable as topical cosmeceuticals. Some studies claim that niacinamide and nicotinic acid are readily converted into each other in vivo40 while other studies speculate that niacinamide and nicotinic acid may have very different pharmaceutical activities despite having identical vitamin activities.[41] In other words, nicotinic acid may have more benefits than topical niacinamide on the skin due to the fact that in addition to having the vitamin effects on skin (increasing levels of niacinamide adenosine dinucleotide [NAD]), it may also have drug-mediated effects on skin via interacting with nicotinic acid receptors present in the skin.[41–44] Yet, the disadvantage of using nicotinic acid as a topical cosmeceutical is its unpleasant side effect of vasodilation that results in skin flushing. This is an effect that is not harmful but intensely disliked by most patients.[45,46] In contrast to nicotinic acid, niacinamide does not cause skin flushing nor does it cause changes in blood pressure, pulse, or body temperature.[47] Due to the decreased number of side effects of topical niacinamide compared to nicotinic acid, the effects of niacinamide as a topical cosmeceutical agent have been studied more to date.
Niacinamide, also known as nicotinamide, is the precursor of important cofactors niacinamide adenosine dinucleotide (NAD) and its phosphate derivative, niacinamide adenosine dinucleotide phosphate (NADP). These cofactors and their reduced forms (NADH and NADPH) serve as reduction-oxidation (redox) coenzymes in more than 40 cellular biochemical reactions. Thus, niacinamide has the potential to exert multiple effects on skin and is a promising anti-aging cosmeceutical ingredient.
What data is available on the percutaneous absorption of niacinamide?
Feldmann et al[48] highlighted the possibilities for the topical application of niacinamide because they were able to prove sufficient percutaneous penetration into human skin.[48,49] In addition, several other studies have used increased levels of NAD in skin cells after the topical application of niacinamide as evidence of percutaneous penetration.[50]
What are the potential mechanisms of action of niacinamide?
Studies have shown that niacinamide has the potential to act as an antioxidant, can improve epidermal barrier function, decrease skin hyperpigmentation, reduce fine lines and wrinkles, decrease redness/blotchiness, decrease skin yellowness (sallowness), and improve skin elasticity.[51,52] The mechanisms by which niacinamide provides this array of skin benefits is not completely understood, but the role of niacinamide as a precursor to the NADP family of coenzymes may play a significant role in all of these improvements.[50]
Antioxidant capacity. Niacinamide increases the antioxidant capacity of skin after topical application by increasing the reduced forms (NADPH), which have potent antioxidant properties.[53–55] This is probably the most well-studied anti-aging effect of niacinamide.
Epidermal barrier function. Niacinamide may improve the skin barrier function in two ways: first, by its ability to upregulate the synthesis of ceramides as well as other SC intercellular lipids, and second, by stimulating keratinocyte differentiation.[56,57] Ceramides and other intercellular SC lipids are known to play a central role in the structural and functional integrity of the epidermal barrier function. The responsible mechanism for the increase of ceramide synthesis in niacinamide-treated, cultured keratinocytes was found to be based on the upregulation of serine palmitoyltransferase, the rate-limiting enzyme in sphingolipid synthesis. The increase in ceramide synthesis has been confirmed in an in-vivo trial after topical application of 2% niacinamide emulsion for four weeks applied twice daily.56 The elevation of ceramides after treatment with niacinamide is associated with an improved barrier function as evidenced by a reduced TEWL and an increase in the cutaneous resistance to potential harmful topical agents.[56] The second mechanism likely responsible for improved barrier function is a stimulation of keratinocyte differentiation seen both in cell cultures in vitro and in-vivo studies conducted by Tanno et al.[56,57] In cell cultures, more rapid keratinocyte differentiation following treatment with niacinamide was established.[56] In particular, it was possible to determine an influence on keratin, K1. K1 is a basic keratin synthesized mainly in the lowest layers of the stratum spinosum. The functional limitations of aging skin include reduced “turnover of the epidermis” (i.e., a slower epidermal cell cycle) due to a deficiency of NADP in aging cells.[58,59] Tanno et al also demonstrated an in-vivo improvement in epidermal barrier function with improved keratinocyte differentiation after the application of topical niacinamide. Once again, the improved barrier function was evident by a decrease in TEWL and increase in SC moisture content. Similar results were also obtained by Ertel et al.[57] In conclusion, it seems that topical application of niacinamide increases NADP levels, which in turn stimulates keratinocyte differentiation. This results in a thicker SC, which is not only associated with an improved barrier, but is also associated with greater hydration retention capacity in the SC.[59]
Erythema and blotchiness. The mechanism by which redness/blotchiness is improved may be related to the improved skin barrier function for reasons discussed above.[50,60,61] Increased barrier function may mean less irritation and redness when the skin encounters environmental insults, such as detergents and soaps, and hence less reddening of the skin. However, this theory has not been substantiated.
Yellowing of skin. The yellowing of skin that comes with aging may be a result of glycation of proteins in the skin called the Maillard reaction. The Maillard reaction is a spontaneous oxidative reaction between protein and sugar that results in cross-linked proteins (Amadori products) that are yellowish-brown in color and are fluorescent.[62–64] These proteins can accumulate in the skin matrix components, similar to collagen, in response to oxidative stress as we age. Published data show a fivefold increase in collagen oxidation products in human skin from age 20 to 80.[65] Since NADH and NADPH are antioxidants and their levels can be increased with niacinamide, a possible effect of topical niacinamide is inhibition of oxidative processes, such as protein oxidation, glycation, and the Maillard reaction, and hence the inhibition of skin yellowing.[66–68]
Fine lines and wrinkles. Multiple mechanisms may be involved in the ability of niacinamide to reduce the appearance of fine lines and wrinkles. The first to consider is that niacinamide may have the ability to increase dermal collagen and protein production. The development of wrinkles is a result of the decrease in epidermal cell layers and dermal components from a reduction in protein and collagen synthesis. Reduced protein synthesis is reflected in the levels of keratin, fillagrin, and involucrin in the skin. Keratin deficiency has an effect on the epidermal cell structure and its water-binding capacity. Fillagrin is an antecedent of natural moisturizing factor (NMF) and hence affects skin hydration. Involucrin is seen as significant for the cell envelope and structure of the SC. In summary, the effects of reduced collagen and protein synthesis are poor skin structure and reduced skin elasticity as well as a decrease in epidermal barrier function with a reduction in SC hydration. In studies on cell cultures, Oblong et al[58] found that in aging cells it was possible to prove that niacinamide, as a precursor of NAD/NADP, stimulated collagen synthesis and the epidermal proteins keratin, fillagrin, and involucrin.[51,58] In addition, another study was able to show niacinamide’s ability to increase dermal matrix collagen production.[66]
The second mechanism that may be relevant to decreasing the appearance of wrinkles is the ability of niacinamide to reduce excess dermal glycosaminoglycans (GAGs). This is a controversial theory because both the elevation and depletion of dermal GAGs are associated with photodamaged or wrinkled skin.[52,69] What is known is that the presence of GAGs is required for normal structure and function of the dermal matrix and increasing the levels of GAGs can increase the moisture content of skin. Testing has indicated that niacinamide reduces excess production of GAGs in old human dermal fibroblasts, thus supporting the potential involvement of this mechanism in reducing the appearance of fine lines and wrinkles.51,70 Given the above analysis and scientific data, it seems more likely that an increase in dermal proteins (including collagen) may play a bigger role in reducing fine lines and wrinkles than decreasing the level of GAGs.
Hyperpigmentation. Topical niacinamide may be effective in decreasing epidermal hyperpigmentation and reducing pigmented spots as we age.[71] Hakozaki et al[71] showed that the reduction of cutaneous pigmentation, surprisingly, was not due to the direct influence of niacinamide on melanin synthesis by melanocytes. Instead, they showed that niacinamide reduced melanosome transfer from melanocytes to surrounding keratinocytes in a co-culture system, although the specific mechanism remains unknown.[71] This was supported by a study using 5% niacinamide moisturizer, which provided 35 to 68 percent inhibition of melanosome transfer from melanocytes to keratinocytes.[71]
What clinical studies are available on niacinamide?
Tanno et al[56] showed a reduction in pigmentation as a result of niacinamide. Eighteen Japanese women with hyperpigmentation were treated on one side of the face with 5% niacinamide and on the other side with vehicle only. The pigmentation change was evaluated qualitatively and quantitatively using high-resolution digital images and subjective judgments. In both forms of evaluation, it was found that after eight weeks of treatment there was significant lightening of hyperpigmentation on the side treated with niacinamide when compared with the effect of the vehicle (p<0.05).[56]
In a separate study also reported by Tanno et al performed with 120 Japanese women, comparisons were made among a sun protection factor (SPF) 15 cream with and without 2% niacinamide and the relevant vehicle. As a result of niacinamide treatment, there was a lightening of the skin after four and six weeks, which was noted to be markedly better than the formula without niacinamide.[56]
It is theoreticized that niacinamide may improve the texture of skin by speeding up epidermal turnover hence functioning as a mild exfoliant.[72] Using a multiple angle reflectance spectrophotometer in an in-vivo test of the back of the hand, Matts and Solenick[73] established a beneficial effect for the topical application of niacinamide in smoothing the skin surface structure. This study demonstrates that the long-term application of 2.5% niacinamide can correct the skin surface damage that results from aging. These results were statistically significant compared with the influence of the vehicle alone (p<0.05).[59] In agreement with the above, another clinical trial using 3.5% niacinamide cream was compared with placebo for four weeks and demonstrated a 14.8-percent reduction in skin roughness (p=0.05).[56,74,75]
One of the best randomized, double-blind, split-face, placebo-controlled, clinical trials published on the anti-aging effects of topical niacinamide was done by Bissett et al.[51] In this study, 50 white females with clinical signs of photodamage applied 5% niacinamide to half of the face and its vehicle control to the other half twice daily for 12 weeks. Analyses of the data revealed a variety of effects related to improvements in skin appearance for topical niacinamide including reductions in fine lines and wrinkles, hyperpigmented spots, red blotchiness, skin sallowness, and improvement in skin elasticity.[51] Matts and Solenick later confirmed the results of Bissett et al with 5% and 2% niacinamide.[59] The results also demonstrated that the anti-aging effects of niacinamide were dose dependent.
What conclusions can be drawn from data on niacinamide?
The topical use of niacinamide for anti-aging has proven to be effective not only when there are signs of a niacin deficiency. Despite the recent discovery of the cosmetic benefit of niacin for the skin, there have been sufficient studies completed to answer all three “Kligman questions.” It is the opinion of the authors that niacinamide is one of the best studied cosmeceutical ingredients for anti-aging. However, further research is required to uncover the specific mechanisms of niacinamide in the skin and to optimize the concentration of niacinamide in cosmeceutical formulations.
Is there additional information on nicotinic acid?
As mentioned earlier, a major obstacle in the topical delivery of therapeutic amounts of nicotinic acid to any tissue is its ability to cause a peripheral vasodilation that leads to a skin flushing response. While this effect is not harmful, it is intensely disliked by most patients.[45,46] This issue may be avoided by using the long chain ester derivative of nicotinic acid, myristyl nicotinate (MN), which is able to deliver large amounts (in concentrations near 5%) of nicotinic acid without flushing.[76,77]
The advantage of using nicotinic acid over niacinamide is its drug-mediated effect on skin as a result of its ability to interact with nicotinic acid receptors present in the skin.[42–44] Nicotinic acid receptors are G protein coupled receptors that when stimulated lead to an increase in skin leptin, which in turn activates several signaling pathways to enhance epidermal differentiation and stimulate wound healing.[78,82]
In a clinical study by Jacobson et al,[76] MN increased skin cell NAD by 25 percent (p=0.0001) demonstrating effective delivery. Relative to placebo, MN treatment of photodamaged facial skin increased SC thickness by approximately 70 percent (p=0.0001) and increased epidermal thickness by approximately 20 percent (p=0.001). In two separate studies, MN treatment increased rates of epidermal renewal by six (p=0.003) to 11 percent (p=0.001) and increased the minimal erythemal dose by 8.9 (p=0.07) and 10 percent (p=0.05) relative to placebo. MN treatment also resulted in reductions in the rates of TEWL of approximately 20 percent relative to placebo on cheeks and arms of study subjects.
The above data demonstrates that topical nicotinic acid preparations can enhance epidermal differentiation and barrier function, suggesting that it may be effective in the treatment of photodamaged skin and other conditions (such as atopic dermatitis) with skin barrier impairments. However, it is hard to compare these results with the results presented above on niacinamide since not all of the same attributes were monitored (such as redness, yellowing, wrinkling, etc). Further investigation is needed to compare the efficacy of MN to niacinamide. Both niacinamide and nicotinic acid have significant numbers of published studies to answer all three major questions to date. However, there is more data available on the anti-aging effects and mechanisms of topical niacinamide.
What background information is available on soy?
Soybeans are known to contain many components with biological activity in the skin.[83] The major components of soy are phospholipids (45–60%) and essential fatty oils (30–35%) while the minor components include the most active compounds, such as isoflavones and the proteases soybean trypsin inhibitor (STI) and Bowman-Birk inhibitor (BBI).[84–86] In this review, the authors will focus on the effects of topical isoflavones and their ability to reduce ROS, stimulate collagen synthesis, increase moisture in the skin and also the proteases STI and BBI,[83,87–94] and reduce skin hyperpigmentation.
What data is available on the percutaneous absorption of soy?
The most plentiful isoflavones in soy are genistein and daidzein. The permeation of isoflavonoids through the skin barrier is poorly investigated. However, the data that is available indicates that the compounds of this group can permeate through the SC and can reach viable layers of the epidermis and dermis.[95,96] The permeation rate of soy through the SC is dependent upon the isoflavonoid’s structure and vehicle composition.[97] In general, the ionized form of a compound has lower percutaneous absorption compared to non-ionized form. This is due to the lipophilic nature of the SC.[98,99] This theory explains why genistein in a completely neutral condition (pH 6) shows higher skin accumulation compared to the ionized form (pH 10.8). The same result was observed for permeation profiles of daidzein.
What are the potential mechanisms of action of soy?
Soy has been purported to exhibit a few potential modes of action, which may correlate with topical treatment of photoaging.
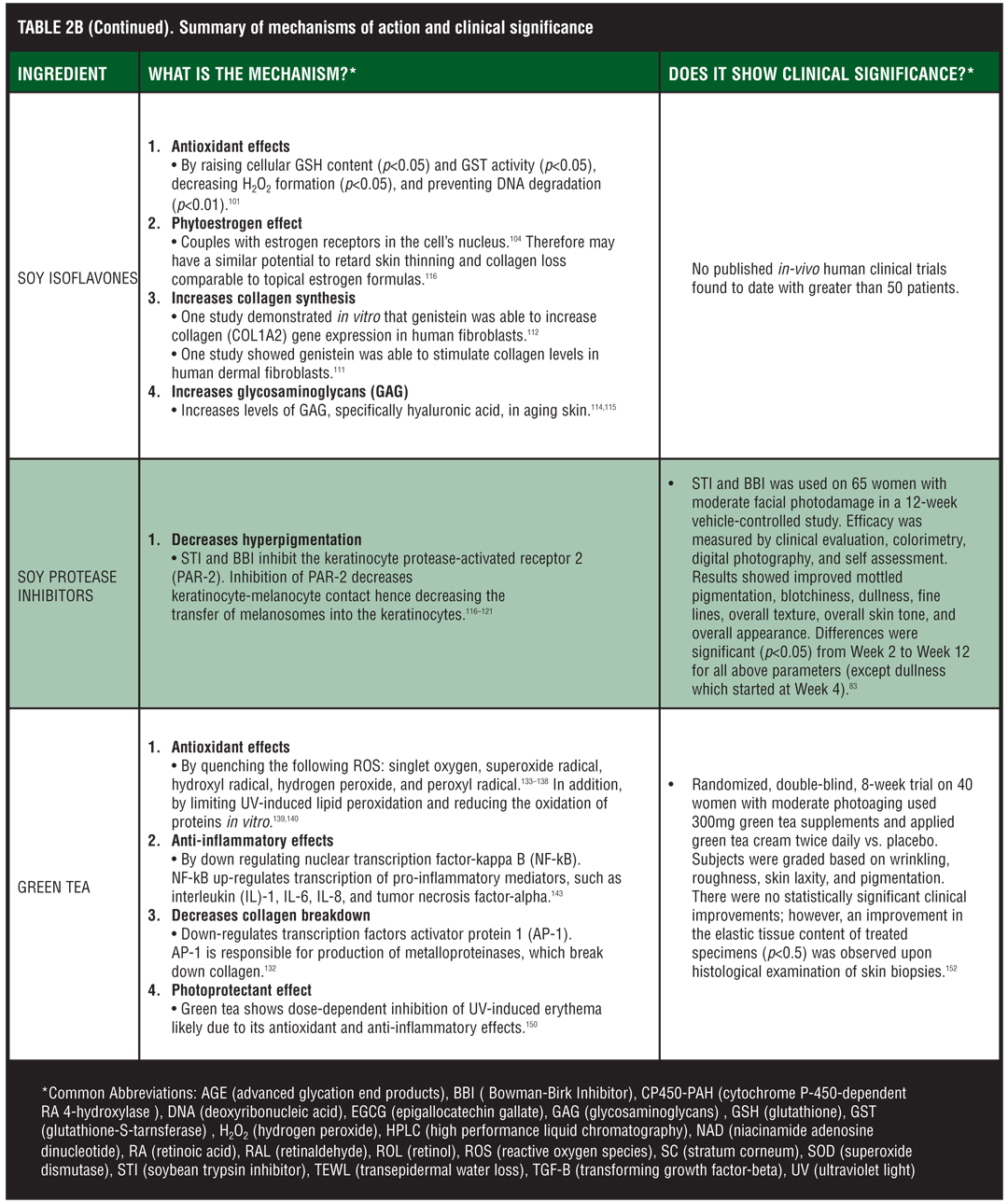
Antioxidant effects. Free radical formation plays a crucial role in aging skin.100 A clinical study by Sharma et al101 found that soy isoflavones (genistein and daidzein) have a fourfold mechanism of action to fight oxidative process in the skin.[101] In this study, soy isoflavones were shown to raise cellular glutathione (GSH) content and glutathione S-transferase (GST) activity (p<0.05), prevent antioxidant enzyme depletion, decrease H2O2 formation (p<0.05), and prevent ornithine decarboxylase (ODC) induction and DNA degradation (p<0.01). Given the wide array of antioxidant effects, the authors speculate that soy isoflavones may not act as antioxidants themselves but instead affect cell signaling processes that increase the skin’s own antioxidant capabilities. However, there is a lack of evidence supporting soy isoflavones as a cell-signaling molecule, and the antioxidant nature of soy isoflavones cannot be sidelined completely because of the polyphenolic structure. Given its structure, genistein can donate hydrogen atoms to deleterious oxygen free radicals and form less reactive phenoxy radicals in the process. Further research is required to determine soy’s true antioxidant mechanism in skin. However, the topical application of soy isoflavones has been shown to increase the antioxidant capability of skin compared to control via increases in the four mechanisms mentioned above. In one study, genistein was able to decrease the H2O2 increment in human keratinocytes caused by ultraviolet B rays by 71 percent and daidzein almost completely inhibited H2O2 production by UVB. Daidzein was expected to be a less effective antioxidant due to its chemical structure; however, this was not the case in this present study.102 Thus, the authors conclude that soy isoflavones may have inhibitory activity against oxidative damage and may be capable of preventing the biochemical alteration associated with aging.[101]
Phytoestrogen effects. The primary metabolites of soy isoflavones, genistein and daidzein, have been identified in various studies in animal and human cell cultures as phytoestrogens. Phytoestrogens are plant compounds with a weak estrogenic effect. In soy, genistein and daidzein are present as glycosides, which do not have estrogenic activity, and only upon conversion to their free isoflavone form do they demonstrate phytoestrogen activity.[103] Phytoestrogens, just like estrogen, work by coupling with estrogen receptors (ERs) in the cell’s nucleus. Two types of receptors, alpha and beta, have been identified and both are present in the skin.[104] One study demonstrated a higher affinity of genistein for ER-beta;[105] however, another study reported a higher affinity of genistein for ER-alpha agonist activity.[106] In comparison with genistein, estradiol has 700-fold more ER-alpha and 45-fold more ER-beta activity.[107] Even though phytoestrogens are weak estrogens, soy may contain as much as 1/1000 of its content as phytoestrogens. Therefore, circulating levels of phytoestrogens may be high and the subsequent biological effect may be great.
Several studies have shown that postmenopausal women have a measurably thinner dermis and less collagen compared to premenopausal women.[108,109] Topical estrogen is able to retard skin thinning and collagen loss in postmenopausal women because estrogen receptor levels are highest in the granular layer of skin. Therefore, the phytoestrogens, genistein and daidzein, have a similar potential to retard skin thinning and collagen loss due to estrogenic stimulation.[116] Further research is needed to compare the estrogenic activity of whole soy versus genistein and daidzein in their free isoflavone form.
Collagen synthesis effects. In other studies, soy isoflavones were investigated for their potential to stimulate collagen synthesis.[111,112] One study demonstrated in vitro that genistein was able to increase collagen (COL1A2) gene expression in in-vitro human fibroblasts.[112] Another study tested four different formulas in terms of their capacity to stimulate de novo collagen synthesis.[111] Depending on the respective method of extraction, the four formulas contained different amounts of isoflavones. The isoflavone daidzein did not elicit any effect, but genistein was able to stimulate collagen levels in human dermal fibroblasts (HDF). Interestingly, the effect on collagen status did not correlate with the isoflavone content of the respective formulas. In other words, the formula with the highest amount of isoflavones did not display the highest efficacy in terms of collagen stimulation. In this study, the specific soy extract that was the most effective contained 10 to 12 percent genistein. The authors speculate that compounds other than isoflavones may play an important role for the collagen stimulatory effect. This fits well with their observation that purified isoflavones stimulated collagen synthesis to a lesser extent than whole topical soy. Therefore, it appears that the pronounced collagen stimulation of soy is only in part because of the isoflavones genistein and daidzein and other ingredients in soy, such as saponins, may play a larger role.[111]
Potential effects on breast cancer. Due to soy’s potential as a phytoestrogen, there is some concern regarding an increased risk of breast cancer and uterine cancer with the use of soy products. However, data concerning this risk is contradictory. On one hand, the majority of breast cancers are estrogen dependent and the use of phytoestrogens could potentiate cancer cell growth, while on the other hand, epidemiological data suggest a protective effect of soy against the development of cancer (including breast cancer).[113] The authors of this review speculate that soy’s protective effect may be due to its antioxidant abilities while potential carcinogenic ability may be related to binding to estrogen receptors. Although the amount of phytoestrogens that are systemically absorbed from a topical preparation is likely very low, it would be prudent to avoid these products in a person with active breast cancer.[116]
Glucosaminoglycan effects. Finally, it has been shown that soy isoflavones can increase levels of GAG and specifically hyaluronic acid (HA) in aging skin although the exact mechanism of action, as far as we are aware, has not been discovered. HA is an anionic, nonsulfated GAG distributed widely throughout the skin. Hyaluronic acid is important for tissue repair and maintaining skin hydration.111 It is widely accepted that the HA content in skin, as well as all the GAG content, declines with age.[114,115] Given the importance of HA for connective tissue overall, and the proven decline of HA in aged skin, there appears to be a necessity for compounds that stimulate HA production in aging skin. More research needs to be completed to demonstrate the efficacy of soy in stimulating HA synthesis and how clinically this increase in HA affects the appearance of skin.
Hyperpigmentation. Soybean trypsin inhibitor (STI) and Bowman-Birk protease inhibitors (BBI) in soy milk exhibit depigmenting activity and prevent UV-induced pigmentation in vitro and in vivo. It has been shown that STI and BBI inhibit the keratinocyte protease-activated receptor 2 (PAR-2), which is involved in the regulation of pigmentation.[116–121] PAR-2 is expressed on keratinocytes and has been shown to increase keratinocyte phagocytosis.[117,118] Several in-vitro and preclinical investigations have demonstrated that the modulation of PAR-2 activation facilitates keratinocyte-melanocyte contact and therefore enhances the transfer of melanosomes into the keratinocytes and produces reversible depigmentation.[116,119]
What clinical studies are available on soy?
Recently, a topical soy formulation was developed containing nondenatured STI and BBI.122 This is important because STI in particular is inactivated by heat and the processing of soybeans and soy milk can destroy their therapeutic effects, including depigmenting activity.[123] Preliminary in-vivo human studies support the skin-lightening effect of nondenatured soy extracts.[122,124–126] A study by Wallo et al[83] investigated the efficacy of a novel soy moisturizer containing nondenatured STI and BBI for the improvement of skin tone, pigmentation, and other photoaging attributes.[83] Sixty-five women, with moderate facial photodamage, were enrolled in the 12-week, parallel, vehicle-controlled study. Efficacy was measured by clinical evaluation, colorimetry, digital photography, and self assessment. Improvement of skin tone was clinically defined as a reduction in mottled hyperpigmentation, lentigines, and blotchiness, with an increase in skin brightness (i.e., reflection of light from skin’s surface). Improvement of skin texture was defined as a reduction in the surface roughness and/or an improvement in fine lines and wrinkling. The results showed that the novel soy moisturizer was significantly more efficacious than the vehicle in improving mottled pigmentation, blotchiness, dullness, fine lines, overall texture, overall skin tone, and overall appearance. Differences were marked from Week 2 to Week 12 for all above parameters (except dullness, which started at Week 4).[83]
Given STI and BBI’s efficacy for treating hyperpigmentation, one might consider using whole soy for the treatment of melasma. Currently, there are conflicting views as to whether soy should be used to treat patients with melasma. On the one hand, one study found that treatment with topical soy twice daily for 12 weeks was shown to be effective for the treatment of melasma.[127] On the other hand, high levels of estrogen have been shown to cause melasma and since soy has estrogen receptor bind capacity, it may be advisable to avoid soy in patients with melasma. Obviously further research is required; however, it should be noted that the isolated constituents of soy STI and BBI do not contain phytoestrogenic abilities and may be a good option for the treatment of melasma.
What conclusions can be drawn from data on soy?
All three of the “Kligman questions” are adequately answered for soy’s protease inhibitor depigmentation effects. However, soy isoflavones, despite all the research into its antioxidant effects is lacking in-vivo, human, clinical trials with greater than 50 patients to prove the efficacy of soy isoflavones efficacy as an anti-aging topical cosmeceutical.
Given that there are two active ingredients in soy, isoflavones and protease inhibitors, there appears to be a need for specific labeling of topical soy products. As a physician evaluating a product, it is important to know whether the product contains whole soy, the isoflavones genistein and daidzein, or soy protease inhibitors STI and BBI in the nondenatured form.
What background information is available on green tea?
White, green, and black teas are derived from the leaves and buds of the tea plant (camellia senensis), with different varieties dependent on the type of processing and antioxidation or fermentation.[128,129] Black tea is the most processed (fermented), while white tea recently replaced green tea as the least processed. The main active ingredients in green tea are polyphenols, also known as catechins, which include epicatechin, epicatechin-3-gallate (ECG), and epigallocatechin-3-gallate (EGCG).[128,129] The largest catechin and most active antioxidant in any tea is EGCG. Green tea has the highest concentration of EGCG.[130]
Polyphenols comprise 30 to 35 percent of the dry weight of the green tea leaf.[107] These polyphenols are believed to have anti-aging effects through decreasing inflammation and acting as a scavenger of free radicals. In addition, compounds found in green tea have been shown to influence biochemical pathways important in cell synthesis and responses of tumor promoters.[131] In this review, the authors focus on the antioxidant and anti-inflammatory attributes of green tea, as these are the factors that most contribute to green tea’s potential as an anti-aging cosmeceutical.
What data is available on the percutaneous absorption of green tea?
The formulary of green tea polyphenols as active ingredients in topical products remains a challenge in the cosmeceutical industry. Green tea polyphenols, as with most antioxidants, are highly unstable and easily oxidized in an ambient environment. Equally difficult is ensuring that the active ingredient penetrates the epidermis and that it stays in the skin long enough to exert its desired effect. EGCG is inherently hydrophilic, limiting its penetration in human skin. Thus, green tea extract is among the more difficult botanicals to formulate.[132] Only when these formulation challenges are met can this topical antioxidant be effective.
After reviewing available product information, it appears that there is little standardization regarding the minimal concentration of green teas in cosmeceuticals, and many products lack active ingredient characterization. Some authors feel that 5% green tea extract is an effective concentration.[132] However, the flaw in this logic is that it is the amount of green tea polyphenols and not the amount of green tea in a product that should be considered when evaluating a product. Many authors recommend products that contain polyphenols in the 90-percent range, which turns the product brown. This brown color does not indicate that the product has oxidized, as is the case when vitamin C products darken.[53,116]
What are the potential mechanisms of action of green tea?
Tea polyphenols have been shown to exhibit antioxidant and anti-inflammatory activities, which may potentially exert clinical benefits.
Antioxidant activity. Tea polyphenols are strong antioxidants.[133] The polyphenols in tea have demonstrated the ability to quench the following ROS: singlet oxygen, superoxide radical, hydroxyl radical, hydrogen peroxide, and peroxyl radical.[133–138] In addition, tea polyphenols have been shown to limit UV-induced lipid peroxidation in skin and reduce the oxidation of proteins in a free radical-generating system in vitro.[139,140]
Anti-inflammatory and collagen synthesis effects. Free radicals are known to promote oxidation of nucleic acids, proteins, and lipids and can damage intracellular structures including DNA.[141,142] Free radicals also up-regulate transcription factors, such as activator protein 1 (AP-1) and nuclear transcription factor-kappa B (NF-kB).[132] AP-1 is responsible for production of metalloproteinases that breakdown existing collagen, contributing to skin wrinkling.[132] NF-kB up-regulates transcription of pro-inflammatory mediators, such as interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor-alpha.[143] Acting through the cell surface, these pro-inflammatory mediators further activate AP-1 and NF-kB, resulting in more damage. It is the sum of these events that are responsible for skin aging.[144]
We now know that green tea and EGCG in addition to being effective free-radical scavengers, down-regulate UV-induced expression of AP-1 and NF-kB and suppress metalloproteinase and age-related collagen cross-linking in mice.[139,145–149] In addition, it has been shown in vitro that green tea polyphenols inhibit the activity of collagenase and increases collagen biosynthesis rate of human fibroblasts.[91]
Photoprotectant effects. Thus taken together, a multitude of scientific evidence exists supporting the notion that green tea extract may improve aging skin through its antioxidant and anti-inflammatory capabilities. These scientific theories were put to the test in studies published by Elmets et al.[150] In their study, human skin was pretreated with either green tea extract or one of its constituents and then exposed to two minimal erythema doses of solar stimulated light. Application of green tea extract and/or one of its constituents resulted in dose-dependent inhibition of UV-induced erythema. EGCG and ECG were the most efficient components in suppressing UV-induced erythema when tested individually. It was also shown that green tea extract can reduce the DNA damage that occurs after UV radiation through mechanisms discussed above.[107,132] Thus, it appears that topical application of green tea extract and some of its components may be useful for mitigating the adverse effects of sunlight on human skin, such as photoaging.
In another study, topical green tea was shown to provide photoprotection anywhere from 24 hours up to 72 hours. It reduced the number of sunburned cells by 66 percent when applied 30 minutes prior to UVB exposure and when applied at 1- to 10-percent concentrations. A dose-dependent inhibition of ultra-violet-induced erythema was evident.[150] Green tea extract also prevented psoralen-UVA photodamage with pre-and post-treatment by reducing erythema, hyperplasia, and hyperkeratosis.[151]
What clinical studies are available on green tea?
To date, we are only aware of one randomized, double-blind, controlled, clinical trial involving topical green tea extract. This study was completed by Chiu et al[152] and consisted of 40 women with moderate photoaging. Eighteen subjects took 300mg green tea supplements twice a day and applied green tea cream twice daily; whereas, the other 18 subjects used a placebo cream and a placebo supplement twice daily. All subjects used the same sunscreen and cleanser. Experts were blinded and subjects were graded based on wrinkling, roughness, course rhytids, skin laxity, pigmentation, and other stigmata associated with photoaging at baseline and at eight weeks. At the end of eight weeks, investigators found no statistically significant clinical improvements in women using the green tea products. Because trends toward improvement were seen in the green tea group, investigators postulate that a longer study might be necessary to demonstrate efficacy. However, an improvement in the elastic tissue content of treated specimens (p<0.5) was observed upon histological examination of skin biopsies.[152]
What conclusions can be drawn from data on green tea?
Although it has been shown that green tea is able to influence mechanisms on skin that are beneficial for anti-aging, via its antioxidant and anti-inflammatory properties, there has yet to be a clinical trial to show a significant clinical improvement in the signs of aging with the topical application of green tea. Even so, green tea products are widely used by consumers despite the lack of evidence. For this reason, a healthy dose of skepticism is appropriate for dermatologists regarding the usefulness of many cosmeceuticals touting green tea until a split-face, double blind, randomized trial involving several concentrations of green tea extract or EGCG is conducted.
Conclusion
The term cosmeceutical was created to define a subgroup of topical products with “drug-like” effects on skin and to differentiate this subgroup from purely cosmetic products and topical prescription drugs. Since cosmeceutical products are claiming to affect the structure and function of skin it makes sense then to hold cosmeceutical products to higher standards of scientific substantiation than cosmetic products. In our opinion, these higher standards should include at minimum being able to substantiate the three major questions proposed by Dr. Albert Kligman, as discussed earlier. Thus, there needs to be a clear understanding that the ingredient penetrates into skin, that it has a defined mechanism of action, and that it has specific clinical effects with continued topical use.
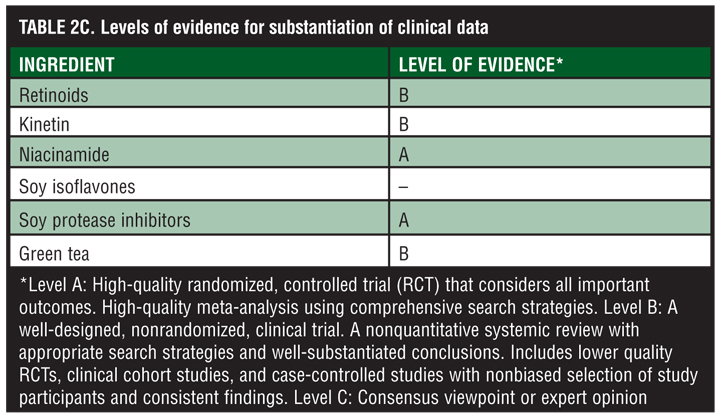
As discussed here in this review, even these five very popular cosmeceutical ingredients fall short of the “Kligman standards” for cosmeceutical ingredients. Most of the research concerning cosmeceutical retinoid ingredients is based upon data related to RA’s effect on the skin, and clinical trials concerning ROL and RAL are scant and lacking in statistical confirmation. Kinetin is supported by research substantiating its effects in plants and antioxidant effects in vitro, yet its anti-aging mechanism of action remains elusive. In addition, the clinical efficacy of kinetin has only been demonstrated with one study. Niacinamide is probably the closest ingredient investigated in this review to satisfy the three major questions in cosmeceutical ingredient analysis. With the available scientific evidence concerning the topical application of niacinamide on skin, we are able to adequately answer questions about permeability, mechanism, and clinical effect. Both green tea and soy are well known for their antioxidant effects, yet there is a conspicuous absence of clinical studies concerning the efficacy of soy and green tea as topical anti-aging cosmeceutical ingredients. It may be that antioxidants, such as soy and green tea, are better at preventing the signs and symptoms of aging than actually reversing the signs of aging. Perhaps clinical trials investigating the prevention of aging would show better efficacy for these two ingredients.
When evaluating a cosmeceutical ingredient, it is important for physicians to access the scientific literature, not only in medicine, but also in basic pharmacology and biochemistry, to verify that the claims made for active cosmeceutical ingredients are backed by a well-defined body of evidence. It was the goal of this review to present and analyze the research available on five popular cosmeceutical ingredients as to their ability to permeate the skin, their mechanisms, and their clinical effects. It is the authors’ hope that physicians will be able to use the information to answer patients’ questions concerning cosmeceutical products with a clearer understanding of what we really know about these ingredients.
References
1. Bigby M. Snake oil for the 21st century. Arch Dermatol. 1998;134:1512–1514.
2. Ross EM. Pharmacodynamics: mechanisms of drug action and the relationship between drug concentration and effect. In Hardman JG, Limbird LE (eds): Goodman and Gilman’s The Pharmacological Basis of Therapeutics, Edition 9. New York, McGraw-Hill;1996:29–41.
3. Kligman D. Cosmeceuticals. Dermatologic Clinics. 2000;18(4):1–7.
4. Green C, Orchard G, Cerio R, et al. A clinicopathological study of the effects of topical retinyl propionate cream in skin photoageing. Clin Exp Dermatol. 1998; 23:162–167
5. Lupo M. Antioxidants and vitamins in cosmetics. Clin Dermatol. 2001; 19: 467–473.
6. Chew AL, Bashir SJ, Maibach HI. Topical retinoids. In: Elsner P, Maibach HI eds. Cosmeceuticals: Drugs vs Cosmetics. New York: Marcel Decker;2000:107–122.
7. Duell EA, Derguini F, Kang S, Elder JT, Voorhees JJ. Extraction of human rpidermis treated with retinol yields retro-retinoids in addition to free retinol and retinyl-esters. J Invest Dermatol. 1996; 107(2):178–182.
8. Baily J, Cretaz M, Scifflers MH, Marty JP. In vitro metabolism by human skin and fibroblasts of retinol, retinal and retinoic acid. Exp Dermatol. 1998;7:27–34.
9. Kang S, Fisher GJ, Voorhees JJ. Photoaging and topical tretinoin: therapy, pathogenesis, and prevention. Arch Dermatol. 1997;133(10);1280–1284.
10. Sorg O, Antille C, Kaya G, Saurat JH. Retinoids in cosmeceuticals. Dermatol Ther. 2006:19:289–296.
11. Berman PE. Aging skin: causes, treatments, and prevention. Nurs Clin N Am. 2007;42:485–500.
12. Ligade VS, Sreedhar D, Manthan J, Udupa N. Cosmeceuticals: Are they truly worth the cost? Indian J Dermatol Venereol Leprol. 2009;75(1):8–9.
13. Singh DK, Lippman SM. Cancer chemoprovention. Part 1: Retinoids and carotenoids and other classic antioxidants. Oncology (Williston Park). 1998:12: 1643–1653.
14. Tsuchiya M, Scita G, Freisleben HJ, et al. Antioxidant radical scavenging activity of carotenoids and retinoids compared to alpha tocopherols. Meth Enzymol. 1992:213:460–472.
15. Tesoriere L, D’Arpa D, Re R, Livrea MA. Antioxidant reactions of all trans retinol in phospholipid bilayers: effect of oxygen partial pressure, radical fluxes, and retinol concentrations. Arch Biochem Biophys. 1997:343:13–18.
16. Sorg O, Tran C, Saurat JH. Cutaneous vitamins A and E in the context of UV or chemically induced oxidative stress. Skin Pharmacol. 2001;14:363–372.
17. Sorg O, Kuenzli S, Kaya G, et al. Proposed mechanisms of action for retinoids derivatives in the treatment of skin. J Cosmet Dermatol. 2005;4:237–244.
18. Serri R, Iorizzo M. Cosmeceuticals: focus on topical in photoaging. Clin Dermatol. 2008;26:633–635.
19. Sefton J, Kligman AM, Kopper SC, Lue JC, Gibson JR. Photodamage pilot study: a double-blind, vehicle-controlled study to assess the efficacy and safety of tazarotene 0.1% gel. J Am Acad Dermatol. 2000;43(4):656–663.
20. Oblong JE, Bissett DL. Retinoids. In: Draelos ZD, ed. Cosmeceuticals. Philadelphia: Elsevier Saunders;2005:36–42.
21. Mukherjee D, Date A, Patravale V, et al. Retinoids in the treatment of aging skin: an overview of clinical efficacy and safety. Clin Interv Aging. 2006;1(4):327–348.
22. Creidi P, Vienne MP, Ochonisky S, et al. Profilometric evaluation of photodamage after topical retinaldehyde and retinoic acid treatment. J Am Acad Dermatol. 1998; 39:960–965.
23. Rivers JK. The role of cosmeceuticals in antiaging therapy. Skin Therapy Lett. 2008;13:1–9.
24. Morganti P. Cosmeceuticals. Clin Dermatol. 2008;26:317
25. Miller CO, Skoog F, von Saltza MH, Strong FM. Kinetin, a cell division factor from deoxyribonucleic acid. J Am Chem Soci. 1955;77:1392.
26. Amasino R. 1955: Kinetin arrives: the 50th anniversary of a new plant hormone. Plant Physiol. 2005;138:1177–1184.
27. Chiu PC, Chan CC, Lin HM, Chiu HC. The clinical anti-aging effects of topical kinetin and niacinamide in Asians: a randomized, double blind, placebo-controlled, split face comparative trial. J Cosmet Dermatol. 2007;6:243–249.
28. Barciszwski J, Rattan SIS, Sibooska G, Clark BFC. Kinetin— 45 years on. Plant Science. 1999:148:37–45.
29. Sharma SP, Kaur J, Rattan SIS. Increased longevity of kinetin-fed Zapronus fruitflies is accompanied by their reduced fecundity and enhanced catalas activity. Biochem Mol Biol Int. 1997;41:869–875.
30. Sharma SP, Kaur J, Rattan SIS. Plant growth hormone kinetin delays aging, prolongs life span, and slows down development of fruitfly Zaprionus paravittiger. Biochem Biophys Res Commun. 1995;216:1067–1071.
31. Rattan SI, Clark BFC. Kinetin delays the onset of ageing characteristics in human fibroblasts. Biochem Biophys Res Commun. 1994;201:665–672.
32. Glaser D. Anti-aging products and cosmeceuticals. Facial Plast Surg Clin N Am. 2004:12:363–372.
33. Quan T, He T, Shao Y, et al. Elevated cysteine rich 61 mediates aberrant collagen homeostasis in chronologically aged and photoaged human skin. Am J Pathol. 2006; 169(2):609–615.
34. Goldstein S, Czapski G. SOD-like activity studies of cytokinin-copper(II) complexes. Free Radic Res Commun. 1991:12–13: 173–177.
35. Kurepa J, Heroat D, Vanmontagu M, Inze D. Differntial expression of CuZn- and Fe-Superoxide dismutase genes of tobacco during development, oxidative stress, and hormonal treatments. Plant Cell Physiol. 1997;38:463–470.
36. Olsen A, Siboska GE, Clark BFC, Rattan SIS. N(6)-Furfuryladenine, kinetin protects against Fenton reaction mediated oxidative damage to DNA. Biochem Physiol Res Commun. 1999; 265:499–502.
37. Lesham YY. Plant senescence processes and free radicals. Free Rad Biol Med. 1988:5:39–49.
38. Verbeke P, Siboska G, Clark BFC, Rattan SIS. Kinetin inhibits protein oxidation and glycoxidation in vitro. Biochem Biophys Res Commun. 2000; 276:1265–1270.
39. McCullough JL, Weinstein GD. Clinical study of safety and efficacy of using topical kinetin 0.1% (Kinerase) to treat photodamaged skin. Cosmetic Dermatol. 2002;15:29–32.
40. Burgess C. Topical vitamins. J Drugs Dermatol. 2008;7(7):2–6.
41. Niacinamide (Monograph) Altern Med Rev. 2002;7(6):525.
42. Lorenzen A, Stannek C, Lang H, et al. Characterization of a G protein-coupled receptor for nicotinic acid. Mol Pharmacol. 2001;59:349–357.
43. Wise A, Foord SM, Fraser NJ, et al. Molecular identification of high and low affinity receptors for nicotinic acid. J Biol Chem. 2003:278:9869–9874.
44. Jacobson EL, Benavente CA, Wondrak GT, Jacobson MK. NAD and PARPs in skin cancer treatment and prevention. Med Sci Monit. 2005;11:24–32.
45. Morrow JD, Awad JA, Oates JA, Roberts Jr LJ. Identification of skin as a major site of prostaglandin D2 release following oral administration of niacin in humans. J Invest Dermatol. 1992;98: 812–815.
46. Carlson LA. Nicotinic acid: the broad spectrum lipid drug. A 50th Anniversary review. J Intern Med. 2005;258:94–114.
47. Namazi MR. Nicotinamide as a potential addition to the anti-atopic dermatitis armamentarium. Int Immunopharmacol. 2004;4:709–712.
48. Feldmann RJ, Maibach HI. Absorption of some organic compounds through the skin in man. J Invest Dermatol. 1970;54: 399–404.
49. Franz TJ. Percutaneous absorption: on the relevance of in vitro data. J Invest Dermatol. 1975;64:190–195.
50. Bissett DL, Oblong JE, Saud A, et al. Topical niacinamide provides skin aging appearance benefits while enhancing barrier function. J Clin Dermatol. 2003; 32S:9–18.
51. Bissett DL, Miyamoto K, Sun P, et al. Topical nicotinamide reduces yellowing, wrinkling, red blotchiness, and hyperpigmented spots in aging facial skin. Int J Cosmet Sci. 2004;26:231–238.
52. Bissett DL, Oblong JE, Berge CA. Niacinamide: a B vitamin that improves aging facial skin appearance. J Dermatol Surg. 2004;31(7 Pt 2):860–865; discussion 865.
53. Baumann L. Less known botanical cosmeceuticals. Dermatol Ther. 2007:20:330–342.
54. Wozniacka A, Sysa-Jedrzejowska A, Adamus J, Gebicki J. Topical application of NADH for the treatment of rosacea and contact dermatitis. Clin Exp Dermatol. 2003;28:61–63.
55. Shindo Y, Witt E, Han D, Epstein W, Packer L. Enzymatic and non-enzymatic antioxidants in epidermis and dermis of human skin. J Invest Dermatol. 1994;102:122–124.
56. Tanno O, Ota Y, Kitamura N, Katsube T, Inoue S. Nicotinamide increases biosynthesis of ceramides as well as other stratum corneum lipids to improve the epidermal permeability. Br J Dermatol. 2000;143:524–531.
57. Ertel KD, Berge CA, Mercurio MG, Fowler TJ, Amburgey MS. New facial moisturizer technology increases exfoliation without compromising barrier function. Presented at: The 58th Annual Meeting of the American Academy of Dermatology; 2000; San Francisco.
58. Oblong JE, Bissett DL, Ritter JL, Kurtz KK, Schnicker MS. Effect of niacinamide on collagen synthesis and markers of keratinocyte differentiation. Presented at: The 60th Annual Meeting of the American Academy of Dermatology. 2002; New Orleans.
59. Gehring W. Nicotinic acid/niacinamide and the skin. J Cosmet Dermatol. 2004;3: 88–93.
60. Bissett DL. Topical niacinamide and barrier enhancement. Cutis. 2002;70S:8–12.
61. Gonzalez S, Moran M, Kochevar IE. Chronic photodamage in skin of mast cell-deficient mice. Photochem Photobiol. 1999;70:248–253.
62. Vlassara H. Recent progress on the biologic and clinical significance of advanced glycolsylation end products. J Lab Clin Med. 1994;124:19–30.
63. Wolff SP, Jiang ZY, Hunt JV. Protein glycation and oxidative stress in diabetes mellitus and aging. Free Rad Biol Med. 1991;10:339–352.
64. Wu JT. Advanced glycosylation end products: a new disease marker for diabetes and aging. J Clin Lab Nal. 1993;7:252–255.
65. Dyer DG, Dunn JA, Thorpe SR, et al. Accumulation of maillard reaction products in skin collagen in diabetes and aging. J Clin Invest. 1993;91:2463–2469.
66. Matts PJ, Oblong JE, Bissett DL. A review of the range of effects of niacinamide in human skin. Intl Fed Soc Cosmet Chem Mag. 2002;5:285–289.
67. Griffiths CE, Voorhees JJT. Topical retinoic acid for photoaging: clinical response and underlying mechanisms. Skin Pharmacol. 1993;6S:70–77.
68. Weiss JS, Ellis CN, Headington JT, Voorheess JJ. Topical tretinoin in the treatment of aging skin. J Am Acad Dermatol. 1988;19:169–175.
69. Schwartz E, Kligman LH. Topical tretinoin increases the tropoelastin and fibronectin content of photoaged hairless mouse skin. J Invest Dermatol. 1995;104:518–522.
70. Kang S, Duell EA, Fisher GJ, et al. Application of retinol to human skin in vivo induces epidermal hyperplasia and cellular retinoid binding proteins characteristic of retinoic acid but without measurable retinoic acid levels or irritation. J Invest Dermatol. 1995;105:549–556.
71. Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer II. Br J Dermatol. 2002;305:260–268.
72. Draelos ZD. Cosmeceuticals: the first step in resurfacing. Cosmet Dermatol. 2005;18:373–375.
73. Matts PJ, Solenick ND. Predicting visual perception of human skin surface texture multiple-angle reflectance. Presented at: The 59th Annual meeting of the American Academy of Dermatology: 2001; Washington.
74. Hakozaki T, Minwalla L, Zhuang J, et al. The effect of nicotinamide on reducing cutaneous pigmentation and suppression of melanosome transfer I. Br J Dermatol. 2002;147:20–31.
75. Shoechnick N. Topical niacinamide improves skin texture. Poster 0465 presented at: The 20th World Congress of Dermatology; July 1–5, 2002; Paris, France.
76. Jacobson EL, Kim H, Kim M, et al. A topical lipophilic niacin derivative increases NAD, epidermal differentiation and barrier function in photodamaged skin. Exp Dermatol. 2007:16:490–499.
77. Wondrak GT, Jacobson MK, Jacobson EL. Endogenous UVA-photosensitizers: mediators of skin photodamage and novel targets for skin photoprotection. Photochem Photobiol Sci. 2006;5:215–237.
78. Hanley K, Jiang Y, Crumrine D, et al. Activators of the nuclear hormone receptors PPAR-alpha and FXR accelerate the development of the fetal epidermal permeability barrier. J Clin Invest. 1997;100:705–712.
79. Sano S, Itami S, Takeda K, et al. Keratinocyte-specific ablation of Stat3 exhibits impaired skin remodeling, but does not affect skin morphogenesis. EMBO J. 1999;18:4657–4668.
80. Frank S, Stallmeyer B, Kampfer H, Kolb N, Pfeilschifter J. Leptin enhances wound re-epithelization and constitutes a direct function of leptin in skin repair. J Clin Invest. 2000;106:501–509.
81. Bendinelli P, Maroni P, Pecori GF, Piccoletti R. Leptin activates Stat3, Stat1, and AP-1 in mouse adipose tissue. Mol Cell Endocrinol. 2000;168:11–20.
82. Unger RH, Zhou YT, Orci L. Regulation of fatty acid homeostasis in cells: novel role of leptin. Proc Natl Acad Sci USA. 1999;96:2327–2332.
83. Wallo W, Nebus J, Leyden JJ. Efficacy of soy moisturizer in photoaging: a double blind, vehicle controlled, 12-week study. J Drugs Dermatol. 2007;6(9):917–927.
84. PDR for Herbal Medicines Second Edition. Montvale, NJ;Thompson Medical Economics:2000.
85. Jellin JM, Gregory P, Butz F, et al. Pharmacist’s Letter/Prescriber’s Letter Natural Medicines Comprehensive Database. 3rd ed. Stockton, CA; Therapeutic Research Faculty: 2000.
86. Weil H, Spencer JM, Gelfand J, et al. They soy isoflavone genistein: a new agent in dermatology. Cosmet Dermatol. 2001;14(2):13–19.
87. Pinnell SR. Cutaneous photodamage, oxidative stress, and topical antioxidant protection. J Am Acad Dermatol. 2003;48:1–19.
88. Wei H, Cai Q, Rahn RO. Inhibition of UV light- and Fenton reaction induced oxidative DNA damage by the soybean isoflavone genistein. Carcinogenesis. 1996;17:73–77.
89. Kin SY, Kin SJ, LeeJY, et al. Protective effects of dietary soy isoflavones against UV-induced skin aging in hairless mouse model. J Am Coll Nutr. 2004;23:157–162.
90. Kennedy AR. The Bowman-Birk inhibitor from soybeans as an anti-carcinogenic agent. Am J Clin Nutr. 1998;68: 1406S–1412S.
91. Gao X, Zhang L, Wei H, Chen H. Efficacy and safety of innovative cosmeceuticals. Clin Dermatol. 2008;26:367–374.
92. Huang MT, Xie JG, Lin CB, et al. Inhibitory effect of topical applications of nondenatured soymilk on the formation and growth of UVB-induced skin tumors. Oncol Res. 2004;14:387–397.
93. Dittman KH, Gueven N, Mayer C, Rodemann HP. Characterization of the amino acids essential for the photo and radioprotective effects of a Bowman-Birk protease inhibitor-derived non-peptide. Protein Eng. 2001;14:157–160.
94. Birk Y. The Bowman-Birk inhibitor. Trypsin- and chymotrypsin-inhibitor from soybeans. Int J Pept Protein Res. 1985;25:113–131.
95. Metfort I, Heilmann J. In vivo skin penetration studies of chamomile flavones. Pharmazie. 1994;49:509–511.
96. Saija A, Tomanio A. Influence of different penetration enhancers on in vitro skin permeation and in vivo photoprotective effect of flavonoids. Int J Pharm. 1998;175:85–89.
97. Arct J, Oborska A. Common cosmetic hydrophilic ingredients as penetration modifiers of flavonoids. Int J Cosmet Sci. 2002;24:357–366.
98. Cole L, Heard CM. Skin permeation enhancement potential of aloe vera and a proposed mechanism based of action based upon size exclusion and pull effect. Int J Pharm. 2007;333:10–16.
99. Lee WR, Shen SC, Fang CL, Liu CJ, Fang JY. Skin pretreatment with an ER: YAG laser promotes the transdermal delivery of three narcotic analgesics. Laser Med Sci. 2007;22:271–278.
100. Sun Y. Free radicals, antioxidants enzymes, and carcinogenesis. Free Radic Biol Med. 1990;8:583–599.
101. Sharma S, Sultana S. Modulatory effect of soy isoflavones on biochemical alterations mediated by TPA in mouse skin model. Food Chem Toxicol. 2004;42:1669–1675.
102. Wei H, Saladi R, Lu Y, et al. Isoflavone genistein: photoprotection and clinical implications in dermatology. J Nutr. 2003;133:3811–3819.
103. Bingham Sa, Atkinson C, Liggins J, Bluck L, Coward A. Phyto-estrogens-where are we now? Br J Nutr. 1998;79:393–406.
104. Brandenberger AW, Tee MK, Lee JY, Chao V, Jaffe RB. Tissue distribution of estrogens receptors alpha (er-alpha) and beta (er-beta) mRNA in the midgestational human fetus. J Clin Endocrinol Metab. 1997;82:3509–3512.
105. Kuiper GG, Carlsson B, Grandien K, et al. Comparison of the ligand binding specificity and transcript tissue distribution of estrogen receptors alpha and beta. Endocrinology. 1997;138:863–870.
106. Barhen T, Carlsson B, Nilsson Y, et al. Differential response of estrogen receptor alpha and estrogen receptor beta to partial estrogen agonists/antagonists. Mol Pharmcol. 1998;54:105–112.
107. Pinnell S. Cutaneous photodamage, oxidative stress, and topical antioxidant protection. J Am Acad Dermatol. 2003;48(1):1–19.
108. Brincat M, Versi E, O’Dowd T, et al. Skin collagen changes in post-menopausal women receiving osteradiol gel. Maturitas. 1987;9:1–5.
109. Varila E, Rantala I, Oikarinen A, et al. The effect of topical oestrdiol on skin collagen of postmenopausal women. Br J Obstet Gynacol. 1995:102:985–989.
110. Baumann L. Botanical Ingredients in cosmeceuticals. J Drugs Dermatol. 2007;6(11):1084–1088.
111. Südel KM, Venzke K, Mielke H, et al. Novel aspects of intrinisc and extrinsic aging of human skin: beneficial effects of soy extract. Photochem Photobiol. 2005;81: 581–587.
112. Greenwel P, Hu W, Kohanski RA, Ramirez F. Tyrosine dephosphorylation of nuclear proteins mimics transforming growth factor beta-1 stimulation of alpha-2 (I) collagen gene expression. Mol Cell Biol. 1995;15:6813–6819.
113. Rice S, Whitehead SA. Phytoestrogens and breast cancer- promoters or protectors? Endocr Relat Cancer. 2006;13:995–1015.
114. Ghersetich I, Lotti T, Campanile G, Grappone C, Dini G. Hyaluronic acid in cutaneous intrinsic aging. Int J Dermatol. 1994;33(2):119–122.
115. Schachtschabel D, Freudenstein G. [Decreased stimulation of hyaluronic acid synthesis by PDGF, IGF-I or serum in the aging process of skin fibroblasts in vitro]. Z Gerontol. 1994;27(3):177–181.
116. Seiberg M, Paine C, Sharlow E, et al. Inhibition of melanosome transfer results in skin lightening. J Invest Dermatol. 2000;115:162–167.
117. Seibeg M, Paine C, Sharlow E, et al. The protease-activated receptor 2 regulates pigmentation via keratinocyte-melanocyte interactions. Exp Cell Res. 2000;254:25–32.
118. Sharlow ER, Paine CS, Babiarz L, et al. The protease-actiavted receptor-2 upregulates keratinocyte phagocytosis. J Cell Sci. 2000;113:3093–3101.
119. Boissy RE. Melanosome transfer to and translocation in the keratinocyte. Exp Dermatol. 2003;12(S2):5–12.
120. Babiarz-Magee L, Chen N, Seiberg M, Lin CB. The expression and activation of protease activated receptor 2 correlate with skin color. Pigment Cell Res. 2004;17:241–251.
121. Scott G, Deng A, Rodriguez-Burford C, et al. Protease-activated receptor 2, a receptor involved in a melanosome transfer, is upregulated in human skin by UV irradiation. J Invest Dermatol. 2001;117:1412–1420.
122. Liu JC, Seiberg M, Miller J, et al. Soy: potential applications in skin care. Poster presented at: The 59th American Academy of Dermatology Meeting: March 2–7, 2001: Washington, DC.
123. Wallace GM, Bannatyne WR, Khaleque A. Studies on the processing and properties of soymilk. II. Effect of processing conditions on trypsin inhibitor activity and the digestibility in vitro of proteins in various soymilk preparations. J Sci Food Agric. 1971;22:526–531.
124. Hermanns JF, Petit L, Martalo O, et al. Unraveling the patterns of subclinical pheomelanin-enriched facial hyper-pigmentation: effect of depigmenting agents. Dermatology. 2000;201:118–122.
125. Wu J, NJS, Kollias N, Liu JC, Leiden J. Total soy to diminish wrinkles and hyperpigmentation in photoaged population. J Am Acad Dermatol. 2004;50:26–36.
126. Finkey MB, Herndon J, Steohens T, Appa Y. Soy moisturizer SPF15 improves dyschromia. J Am Acad Dermatol. 2005;52:170.
127. Perard G, et al. Poster presented at: The 59th Annual Meeting of the American Academy of Dermatology; March 2–7,2001:Washington, DC.
128. Camouse MM, Hanneman KK, Conrad EP, Baron ED. Protective effects of tea polyphenols and caffeine. Expert Rev Anticancer Ther. 2005;5:1061–1068.
129. Katiyar S, Elmets CA, Katiyar SK. Green tea and skin cancer: photoimmunology, angiogenesis, and DNA repair. J Nutr Biochem. 2007;18:287–296.
130. Spencer JM. Chemoprevention of skin cancer and photoaging. Cosmet Dermatol. 2001;14(6):25–28.
131. Katiyar SK, Ahmad N, Mukhtar H. Green tea and skin. Arch Dermatol. 2000;136: 989–994.
132. Farris P. Idebenone, green tea, and coffeeberry extract: new and innovative antioxidants. Dermatol Ther. 2007;20: 322–329.
133. Jovanovic SV, Simic MG. Antioxidants in nutrition. Ann N Y Acad Sci. 2000;899: 326–334.
134. Unno T, Yayabe F, Hayakawa T, Tsurge H. Electron spin resonance spectroscopic evaluation of scavenging acitivity of tea catechins on superoxide radicals generated by phenazine methosulfate and NADH system. Food Chem. 2002;76:259–265.
135. Ueda JI, Saito N, Shimazu Y, Ozawa T. A comparison of scavenging abilities of antioxidants against hydroxyl radicals. Arch Biochem Biophys. 1996;333:377–384.
136. Shi XL, YE JP, Leonard SS, et al. Antioxidant properties of epicatechin-3-galate and its inhibition of Cr (VI)-induced DNA damage and CR (IV) or TPA-Stimulated NF-kappa B activation. Mol Cell Biochem. 2000;206:125–132.
137. Grinberg LN, Newmark H, Kitrossky N, et al. Protective effects of tea polyphenols against oxidative damage to red cells. Boichem Pharmacol. 1997;54:973–978.
138. Liu ZQ, Ma LP, Zhou B, Yang L, Liu ZL. Antioxidative effects of green tea polyphenols on free radical initiated and photosensitized peroxidation of human low density lipoprotein. Chem Phys Lipids. 2000;106:53–63.
139. Kim J, Hwang JS, Cho YK, et al. Protective effects of epigallocatechin-3-gallate on UVA and UVB induced skin damage. Skin Pharmacol Appl Skin Physiol. 2001;14:11–19.
140. Nakagawa T, Yokozawa T, Terasawa K, Shu S, Juneja LR. Protective activity of green tea against free radical and glucose medicated protein damage. J Argic Food Chem. 2002;50:2418–2422.
141. Sohal RS, Weindrunch R. Oxidative stress, caloric restriction and aging. Science. 1996:273:59–63.
142. Camougrand N, Rigoulet M. Aging and oxidative stress: studies of some genes involved both in aging and in response to oxidative stress. Respir Physiol. 2001;128:393–401.
143. Senftleben U, Karin M. The ILK/NF-Kappa B pathway. Crit Care Med. 2002;30: S18–S26.
144. Fisher GJ, Kang S, Varani, et al. Mechanisms of photoaging and chrono-logical skin aging. Arch Dermatol. 2002;138:1462–1470.
145. Wei H, Zhang X, Zhao J, et al. Scavenging of hydrogen peroxide and inhibition of ultraviolet induced oxidative DNA damage by aqueous extracts from green and black teas. Free Radic Biol Med. 1999;26:1427.
146. Katiyar SK, Afaq F, Perez A, et al. Green tea polyphenol (-)-epigallocatechin-3-gallate treatment of human skin inhibits ultraviolet radiation-induced oxidative stress. Carcinogenesis. 2001;22:287–294.
147. Vayalil PK, Mittal A, Hara Y, et al. Green tea polyphenols prevent UV light induced oxidative damage and matrix metalloproteinases expression in mouse skin. J Invest Dermatol. 2004;122: 1480–1487.
148. Vayalil PK, Elemets CA, Katiyar SK. Treatment of green tea polyphenols in hydrophilic cream prevents UVB induced oxidation of lipids and proteins, depletion of antioxidant enzymes and phos-phorylation of MAPK proteins in SKH-1 hairless mouse skin. Carcinogenesis. 2003;24:927–936.
149. Rutter K, Sell DR, Fraser N, et al. Green tea extract suppresses the age related increase in collagen crosslinking and fluorescent products in C&BL/6 mice. Int J Vitam Nutr Res. 2003;73:453–460.
150. Elmets C, Singh D, Tubesing K, et al. Cutaneous photoprotection from ultraviolet injury by green tea polyphenols. J Am Acad Dermatol. 2001;44:425–432.
151. Zhao F, Zhang YJ, Jinx H, et al. Green tea products against psoralen plus UVA induced photochemical damage to skin. J Invest Dermatol. 1999;70:637–644.
152. Chiu AE, Chan JL, Kern DG, et al. Double-blinded, placebo-controlled trial of green tea extracts in the clinical and histologic appearance of photoaging skin. Dermatol Surg. 2005;31:855–860.