aNeal Carlin, BS; bLindaSusan Marcus, MD; aRobert Carlin, MA
aLindaSusan Marcus, MD, Wyckoff, New Jersey; bPrivate Practice, Wyckoff, New Jersey;
Director–Chair, Department of Dermatology, Valley Hospital, Ridgewood, New Jersey
Abstract
A 15-year-old Caucasian boy with a diagnosis of confluent and reticulated papillomatosis who had received numerous treatments with minimal responses cleared with a 20-week course of 13-cis-retinoic acid and has remained in remission. It is important to consider the use of oral retinoids in the treatment of this stubborn, unsightly, and psychologically upsetting disease. (J Clin Aesthetic Dermatol. 2010;3(7):56–57.)
This case describes a 15-year-old Caucasian boy who presented with a pruritic, brownish eruption of a few years’ duration that was treated with diphenhydramine hydrochloride cream and moisturizers. His past history is unremarkable except for being premature due to abruptio placenta. He is overweight and plays football. His prior skin diagnoses include eczema, for which he was given topical steroids, and tinea versicolor, which responded minimally to oral and topical ketoconazole.
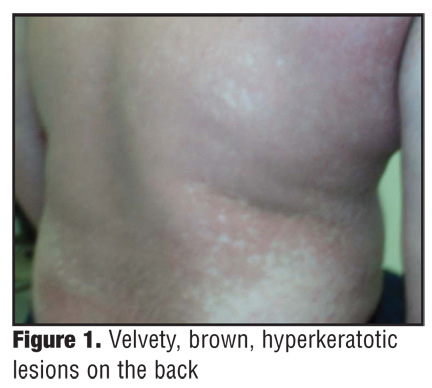
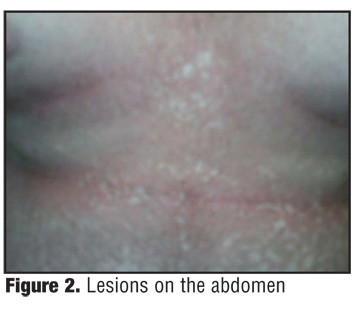
On physical examination, the patient had brownish-tan sessile, velvety, hyperkeratotic, coalescing papules on the chest, back, nape of neck, and extensor surfaces of upper arms (Figure 1
and Figure 2). Scraping produced a powdery scale.
{kind=link}
{kind=link}
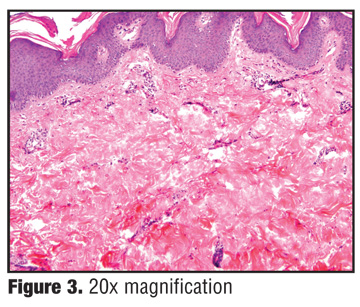
A biopsy showed horn formation and was difficult to assess (Figure 3). Asteatotic eczema, pityriasis rubra pilaris, acanthosis, and fungus were considered and dismissed. In view of the deeper sections and the history, a diagnosis of confluent and reticulated papillomatosis of Gougerot et Carteaud (also known as Gougerot-Carteaud syndrome) was made.
{kind=link}
Treatment began with minocycline 100mg daily for three months. The dosage was tapered to 50mg daily over the next three months as the lesions faded and the patient’s skin felt smooth.
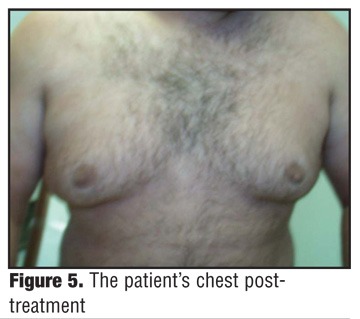
Unfortunately, the lesions began to return, and isotretinoin was started at 1mg/kg or 60mg twice daily with food for 20 weeks. The patient’s triglycerides were monitored and fenofibrate was added in the third month of the regimen. The patient had an excellent response—the unsightly lesions were eliminated and his skin became smooth (Figure 4 and Figure 5).
{kind=link}
{kind=link}
Discussion
Confluent and reticulated papillomatosis is a rare disease affecting teenagers who initially develop 1 to 2mm erythematous papules that become brownish hyperkeratotic 4 to 5mm papules, which coalesce with a peripheral reticulate pattern. The lesions occur over the trunk and extensor surfaces sparing the mucous membranes.[1] Gougerot and Carteaud first described confluent pigmented reticulated papillomatosis in 1927 and 1932.[2,3] Wise described the first case in the United States 10 years later.[4] Two other variants are nummular and punctate papillomatosis. Familial cases have been noted. The prevalence of males to females and African Americans to Caucasians is debatable as many cases are not reported.[5]
There has been a constant argument as to the classification of Gougerot-Carteaud syndrome; however, it is generally agreed that it is a distinct entity from acanthosis nigricans. Some authors feel it may represent an endocrine disturbance including a relation to Cushing’s disease, irregular menstruation, diabetes mellitus, thyroid, pituitary, hirsutism, hypertrichosis, obesity, an abnormal reaction to fungi, Pityrosporum or bacteria, a hereditary disorder, or a variant of amyloidosis. Histology and the lack of positive correlation to blood workups mitigate against these proposals.[6]
Electron microscope and immunohistochemical studies show abnormal keratinocyte differentiation, increased transition cell layer, and increased lamellar granules in the stratum granulosum as well as increased melanosomes in the stratum corneum.[7] Involucrin, keratin 16, and Ki-67 expression are increased.[8] Although the etiology of this disorder remains unknown, the defect in keratinization suggest its pathophysiology.
The disease exacerbates and remits. Minocycline has been used to treat Gougerot-Carteaud syndrome with some success; however, it usually recurs.[9] Pathological studies indicating abnormal keratinization may be the basis for the use of a retinoid as treatment. Vitamin A, tretinoin cream, and etretinate have been used in the past with some success.[10–12] Isotretinoin (2mg/kg/day) for two months with the dosage reduced to 1.14mg/kg/day beginning with the third month was used in a patient and there were no recurrences.[5] Recommended dosages for the use of isotretinoin is 0.5mg/kg/day to 2mg/kg/day. The 1mg/kg/day dosage was prescribed to the patient reported in this case and was administered for the recommended 20 weeks of treatment with excellent results.[13]
Conclusion
Since this disorder causes extreme distress to patients, it is imperative that treatment be effective and swift. Considering the pathophysiology of confluent and reticulated papillomatosis, it seems reasonable to use oral retinoid therapy, which should be considered the treatment of choice for Gougerot-Carteaud syndrome. Oral retinoid therapy may bring a prolonged response and control of an unsightly, annoying, psychologically upsetting disease in young people.
References
1. Ponten F, Lundeberg J, Asplund A. Neoplasms of the skin. In: Bologna JL, Jorizzo JL, Rapini RP, et al, eds. Dermatology. 2nd ed. Spain: Mosby Elsevier; 2008:1677–1678.
2. Gougerot H, Carteaud A. Papilloma-tose pigmentee incominee. Bull So Fr Dermatol Syp. 1927;34:719–721.
3. Gougerot H, Carteaud A. Neve forme der pappillomatose. Arch Dermatol Syph. 1932;165: 232–267.
4. Young AW. Cutaneous papillomatosis. AMA Arch Derm Syphilol. 1953;67(6):594–597.
5. Lee MP, Stiller MJ, McClain SA, Shupack JL, Cohen DE. Confluent and reticulated papillomatosis: response to high-dose oral isotretinoin therapy and reassessment of epidemiologic data. J Am Acad Dermatol. 1994;31: 327–331.
6. Schwartz R. Confluent and reticulated papillomatosis: treatment and medication. Sep 3, 2009. http://emedicne. medscape.com/article/1106748-treatment. Accessed on January 24, 2010.
7. Jimbow M, Tallpash O, Jimbow K. Confluent and reticulated papillomatosis: clinical, light, and electron microscopic studies. Int J Dermatol. 1992;31(7):480–483.
8. Kanitakis J, Zambruno G, Viac J, Thivolet J. Involucrin expression in keratinization disorders of the skin—a preliminary study. Br J Dermatol. 1987;117(4):479–480.
9. Sassolas B, Plantin P, Guillet G. Confluent and reticulated papillomatosis: treatment with minocycline. J Am Acad Derm. 1992;26:501–502.
10. Lim KB. Confluent and reticular papillomatosis. Cutis. 1988;41:215–217.
11. Bruynzeel-Koomen C, de Wit RFE. Confluent and reticulated papillomatosis successfully treated with the aromatic etretinate. Arch Dermatol. 1984;120:1236–1237.
12. Kim JG, Seo WF, Cha MG, et al. Confluent and reticulated papillomatosis treated with aromatic analog of vitamin A acid (Ro10-9359). Korean Dermatol. 1982;20:467–470.
13. Accutane [package insert]. South San Francisco, CA: Genentech, a member of the Roche Group; 2007.