Carmen Rodríguez-Cerdeira, MD; Elena Sánchez-Blanco
Dr. Rodríguez-Cerdeira is from the Dermatology Department, CHUVI and University of Vigo, Vigo, Spain; Sánchez-Blanco is a Postgraduate researcher, University of Vigo, Vigo, Spain
Disclosure: The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership, opinions, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Abstract
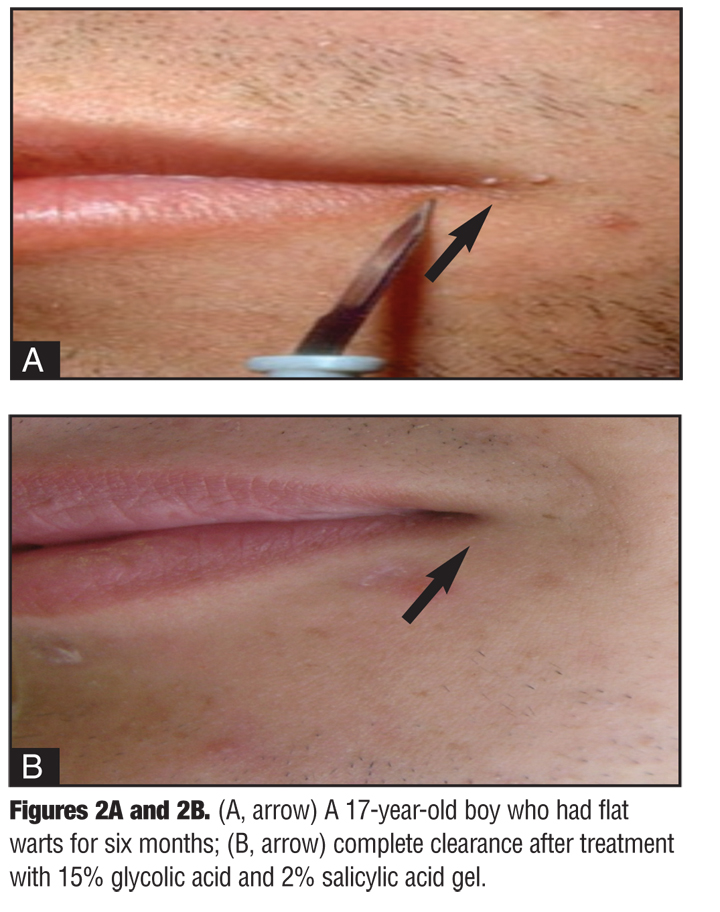
Background: Facial flat warts are a contagious viral disease that can cause disturbing cosmetic problems. Topical glycolic acid has been reported to be effective in dermatological treatment depending on the exfoliant capacity, but has not often been reported to be effective in the treatment of facial flat warts. Objective: The aim of this paper was to evaluate the efficacy and safety of glycolic acid 15% topical gel plus salicylic acid 2% in the treatment of recalcitrant facial flat warts. Methods: A total of 20 consecutive patients 7 to 16 years of age with recalcitrant facial flat warts were enrolled in this study. Patients having warts by the eye and lip regions were excluded from the study. A fine layer of face gel was applied to the treatment area once daily. Most of the participants had tried different treatments with no success. Assessments for the response and the occurrence of side effects were performed every two weeks at Weeks 2, 4, 6, and 8. Results: All the patients were clinically cured within eight weeks. Seven patients cleared in four weeks, and 13 patients cleared in eight weeks. No noticeable adverse events were related to the skin. Conclusion: Topical gel of glycolic acid 15% plus salicylic acid 2% is safe and effective when applied to facial flat warts once daily until clearance and may be considered as first-line treatment. (J Clin Aesthet Dermatol. 2011;4(9):62–64.)
Flat viral warts are circumscribed papules with hyperkeratotic surfaces that can occur singly or in groups. In these types of warts, the human papilloma virus (HPV) has been shown to infect the koilocytes. Although no viral subtype is absolute, typically the infection is with HPV types 3, 10, 28, and 41. These warts are small in size (1–5mm), flat, or slightly elevated lesions. Flat viral warts typically present as skin-colored or light brownish, flat-topped papules on the face, beard area, or on the back of the hands, and primarily affect children and young adults.[1] Their evolution is variable, and although two thirds of cases regress spontaneously in the course of two years due to immunological mechanisms, they occasionally are long lasting.[1] Flat viral warts can greatly affect a patient’s quality of life, and their persistence and/or recurrence can cause frustration. Moderate-to-extreme discomfort is reported in 51.7 percent of patients, and social or leisure activities are affected to a moderate-to-extreme degree in 38.8 percent of patients.[2]
Methods
The present prospective, non-blinded, non-randomized study was conducted at a public practice surgery center. The study population comprised 20 patients ranging in age from 7 to 16 (9.65±2.68). Eleven patients were male and nine were female. All patients were identified as having facial flat warts (FFW). Of the study population, patients had multiple warts (average number 10) before the treatment, with an average duration of five months. The treatment consisted of 15% glycolic acid and 2% salicylic acid gel (Neostrata®). The treatment was started once daily over the entire face and maintained for two months. A fine layer of face gel was applied on the whole surface where the warts were present, avoiding the eyelids and lips. In children 7 to 10 years of age, face gel was applied by their parents. Clinical controls were performed at Weeks 2, 4, 6, and 8.
The follow up showed a favorable course with the lesions clearing in all 20 patients. The warts disappeared within four weeks in seven patients and before eight weeks in 13 patients (Figure 1, Figure 2, Figure 3). Four patients (2 male and 2 female) complained of severe irritation with erythema, which diminished when the dose was reduced to one application every two days (Figure 4). No noticeable side effects were recorded. Four patients had received previous treatment with salicylic acid, two patients had received cryotherapy, and one patient had received retinoic acid. The side effects were observed among the patients who did not receive previous therapy.
{kind=link}
{kind=link}
{kind=link}
Discussion
The following therapies have been used in the treatment of FFWs with varying success: salicylic acid, cryotherapy, retinoic acid, photodynamic therapy (topical 5-aminolevulinic acid photodynamic therapy), pulsed dye laser (PDL), and Candida antigen. Patients should be informed of the possible side effects of all treatments, such as severe erythema, exfoliation, and postinflammatory hyperpigmentation. Patients should also be informed about the importance of sun protection.[2–5]
Good results have been reported with topical imiquimod 5%, with complete clearance of all FFWs occurring after three weeks of therapy. However, this treatment is expensive.[6]
Glycolic acid has been used in the treatment of FFWs with good results. It has been suggested that alpha-hydroxy acids can produce an authentic exfoliation and dehiscence of the corneocytes from recently formed layers of the stratum corneum. Alpha-hydroxy acids also reduce the number of desmosomes and tonofilaments. These effects may be effective in the treatment of flat warts. Concerning glycolic acid, its therapeutically employed concentrations range from 8 to 70 percent, depending on the desired exfoliant capacity and the type of patients. The presumed mode of action is by exfoliation and dehiscence of corneocytes of stratum corneum.[7] Glycolic acid 15% has been shown to be effective and well tolerated.[8] Glycolic acid plus salicylic acid, in spite of its high cost, is also well tolerated and did not produce scars upon withdraw of therapy in any patient. In fact, patients obtained excellent results.
Many other treatments for FFWs are expensive and require that parents accompany their children to several office visit, resulting in loss of time and work hours. Glycolic acid plus salicylic acid is self-administered, requires no special care, and can be prescribed and monitored by nursing staff.
The authors conclude that treatment with 15% glycolic acid and 2% salicylic acid may be considered first-line treatment for nonrecalcitrant FFWs in children or young adults who suffer cosmetic embarrassment or pain.
References
1. Massing AM, Epstein WL. Natural history of warts. A two-year study. Arch Dermatol. 1963;87:306–310.
2. Sterling JC, Handfield-Jones S, Hudson PM. Guidelines for the management of cutaneous warts. Br J Dermatol. 2001;144:4–11.
3. Leman JA, Benton EC. Verrucas. Guidelines for management. Am J Clin Dermatol. 2000;1:143–149.
4. Kubeyinje EP. Evaluation of the efficacy and safety of 0.05% tretinoin cream in the treatment of plane warts in Arab children. J Dermatol Treat. 1996;7:21–22.
5. Kartal Durmazlar SP, Atacan D, Eskioglu F. Cantharidin treatment for recalcitrant facial flat warts: a preliminary study. J Dermatolog Treat. 2009;20:114–119.
6. Khan Durani B, Jappe U. Successful treatment of facial plane warts with imiquimod. Br J Dermatol. 2002;147:1018.
7. Van Scott EJ, Yu RJ. Control of keratinization with alpha hydroxy acids and related compounds. Arch Dermatol. 1974;110:586–590.
8. Borbujo J, Olmos O, Zamora E, Díez JJ. Treatment of verrucae plana with 15% glycolic acid. Int J Dermatol. 2000;39:236–240.