Grace K. Kim, DO, Dermatology Research Fellow, Mohave Skin & Cancer Clinics, Las Vegas, Nevada; James Q. Del Rosso, DO, Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada, and Director of Dermatology Research, Mohave Skin & Cancer Clinics, Las Vegas, Nevada
Abstract
Psoriasis is a commonly encountered dermatosis with a variety of internal and external paradoxical factors contributing to the clinical course of the disease. There are several drugs described in the literature that have been associated with the initiation, exacerbation, and aggravation of psoriasis. Understanding the pathophysiology can provide clues to treatment and management of drug-induced and drug-aggravated psoriasis, which may be indistinguishable from idiopathic psoriasis. The clinical manifestations of drug-associated psoriasis can range from plaque-type psoriasis to severe erythroderma, thus warranting astute and sustained clinical observation.
(J Clin Aesthetic Dermatol. 2010;3(1):32–38.)
Psoriasis is a chronic, immune-mediated, inflammatory condition seen frequently in the clinical practice with a reported prevalence of 0.6 to 4.8 percent in the general population.[1,2] Some factors known to trigger psoriasis include smoking, alcohol consumption, body mass index (BMI), trauma, infection, endocrine disorders, drugs, and acute withdrawal of systemic or potent topical corticosteroids.[1] Analysis of comedication in a study of 1,203 psoriasis patients revealed 23.2 percent of patients were taking more than three systemic medications, and of these patients, 11.1 percent were taking more than 10 medications.[3] Further analysis demonstrated that comorbid cardiac and metabolic disorders are common in these individuals with a high prevalence of hypertension (28.2%), diabetes (10.5%), and dyslipidemia (12.5%).[3] With this in mind, many psoriasis patients can be on multi-drug regimens; therefore, careful analysis of medications that can exacerbate the disease is prudent. Drugs reported to be associated with exacerbation/induction of psoriasis are based mostly on case reports, with no definitive “cause-and-effect” links between these drugs and onset of psoriasis.
Drugs have several ways in which they can affect the diathesis of psoriasis including 1) precipitation of psoriasis de novo in predisposed and nonpredisposed individuals; 2) exacerbation of pre-existing psoriatic lesions; 3) induction of lesions in clinically normal skin in patients with psoriasis; and 4) development of treatment-resistant psoriasis.[4] The clinical presentation of drug-provoked psoriasis spans the spectrum of generalized plaque psoriasis, palmoplantar pustulosis, and erythroderma.[4] The nails and scalp can also be involved, thus making the distinction of drug-associated psoriasis a clinically difficult diagnosis.[4] In addition, the mechanism of action can also involve both immunological and nonimmunological pathways.[5] Therapeutic agents can also be categorized as having a causal relationship to psoriasis, with considerable but insufficient data supporting induction of psoriasis, or occasionally an association with psoriasis.[4] Drugs that appear to have a strong causal relationship to psoriasis are beta-blockers, lithium, synthetic antimalarials, nonsteroidal anti-inflammatory drugs (NSAIDs), and tetracyclines, which will be discussed in this review.[4]
Psoriasiform Drug Eruption and Drug-Provoked Psoriasis
“Psoriasiform drug eruption” is a broad term referring to a heterogeneous group of disorders that clinically and/or histologically simulate psoriasis at some point during the course of the disease.[6] A psoriasiform eruption is used also to describe a histological reaction pattern, which exhibits presence of cellular infiltration, papillomatosis, and epidermal hyperplasia with elongation of rete ridges.[6] Hypergranulosis and parakeratosis may also be observed in selected cases.[7–10] This type of eruption can also be seen with seborrheic dermatitis, pityriasis rubra pilaris, secondary syphilis, pityriasis rosea, mycosis fungoides, drugs, and some malignancies.[6] These psoriasiform reactions are elicited by inflammatory events that cause dysregulation of cytokines, growth factors, and abnormal keratinocyte proliferation.[6] Depending on the disorder, the lesions may vary in size, shape, extent and type of scaling, and anatomic distribution.[6]
Drug-provoked psoriasis can be divided into two categories (Table 1). The first category, drug-induced psoriasis, is where discontinuation of the causative drug stops the further progression of the disease. The second category, drug-aggravated psoriasis, is where the disease progresses even after the discontinuation of the offending drug.[4] True drug-induced psoriasis tends to occur in a de-novo fashion in patients with no family or previous history of psoriasis.[5] The clinical presentation of these lesions may often mimic the pustular variant of psoriasis, often with no nail involvement or associated arthritis.[5] Furthermore, there is an absence of Munro microabscesses, few macrophages, and sparse vascular changes noted histologically.[5] Drug-aggravated psoriasis exhibits a propensity to occur in patients with a history of psoriasis or with a genetic predisposition for the disease. Patients can have exacerbation of pre-existing psoriatic lesions or develop new lesions in previously uninvolved skin. Histological examination reveals features that are more characteristic of psoriasis vulgaris.[11]
{kind=link}
Beta Blockers and Drug-Provoked Psoriasis
Beta blockers are a very popular class of drugs used to treat both cardiovascular and noncardiovascular diseases, including hypertension, ischemic heart disease, arrhythmias, heart failure, hyperthyroidism, glaucoma, and anxiety disorders.[11] They exert their action by blockade of either ß1 receptors (cardioselective) or ß2 receptors (noncardioselective), hence their classification. ß2-adrenergic receptors are found predominantly on epidermal keratinocytes and on the surface of macrophages.11 Several theories have been proposed regarding the pathogenesis of beta blocker-induced psoriasis. These include a delayed-type hypersensitivity reaction, immunological mechanisms including impaired lymphocyte transformation, or alterations in the cyclic adenosine monophosphate (cAMP) pathway.[12–14] Cyclic adenosine monophosphate is an intracellular messenger that is responsible for the stimulation of proteins for cellular differentiation and inhibition of proliferation.[11] The most reliable proposition is that blockade of epidermal ß2 receptors leads to a decrease in intraepidermal cAMP causing keratinocyte hyperproliferation.[4] Biopsy specimens from eruptions caused by ß1 blockers (metoprolol and atenolol) are characterized by excessive degranulation of neutrophils in the dermis.[15] Nonselective beta blockers (propranolol, nadolol, and sotalol) were marked by excessive release of proteolytic enzymes from macrophages.[15] Both groups of beta blockers exhibit excessive release of enzymes by lymphocytes, neutrophils, and macrophages, and it is believed that this event is responsible for the presence of hyperproliferation and psoriasiform change. It has also been reported that beta blockers increase phosphorylation in T cells in psoriasis, which may be relevant to intracellular levels of calcium.16 The blockade of these receptors has been implicated in the pathogenesis of drug-provoked psoriasis in both groups of beta blockers.[11]
Clinical manifestations of beta-blocker-provoked psoriasis. In the past, beta blockers have been known to cause drug-induced/exacerbation of psoriasis, psoriasiform dermatitis, eczematous eruptions, and lichenoid changes.[8] Psoriasiform eruptions are the most common cutaneous consequence of beta-blocker therapy, seen more frequently in patients with no past or family history of psoriasis.[4,17] Clinical improvement after withdrawal of the implicated drug is the distinguishing feature in many cases suggesting drug-induced psoriasis.[4] In a case-controlled and case-crossover study of 110 patients who were hospitalized for extensive psoriasis vulgaris, beta blockers were considered a major factor in triggering or aggravating psoriasis.[18–20] Practolol is the prototype cardioselective beta blocker, which is no longer available due to the high incidence of cutaneous side effects reported, including psoriasiform eruptions and exacerbations of pre-existing psoriasis.[12] Transformation of plaque-type psoriasis into pustular psoriasis with pindolol has also been observed.[21] In addition, atenolol has been reported to precipitate psoriasiform pustulosis.[22] Topical application of timolol in the treatment of open-angle glaucoma has been reported to induce psoriasis and to transform psoriasis vulgaris into psoriatic erythroderma through the passage into the systemic circulation via the conjunctiva.[23,24]
Both psoriasiform eruption and drug-induced/aggravated psoriasis from beta-blocker therapy usually appear at 1 to 18 months after initiation of therapy.[15] In psoriasiform eruptions, lesions clear after several weeks of discontinuing the medication.[15] In addition, re-exposure with oral challenge results in recurrence within a few days.[15] Many believe that psoriasiform eruptions from beta blockers are not true representations of psoriasis, partly due to histological features and partly due to clinical presentations exhibiting lesions that are less red, thick, or scaly than classic lesions of psoriasis, and usually with absence of knee and elbow involvement.[15] In contrast, beta-blocker-provoked psoriasis improves upon discontinuation of medication, but usually does not completely resolve.[11] In regard to beta-blocker-induced, de-novo pustular psoriasis, the duration is much shorter.[4] Reasons for these variations remain a mystery and may be due to genetic, environmental, or racial backgrounds.
Management of beta-blocker-provoked psoriasis. Cross reactivity between both groups of beta blockers have led many researchers to believe that the mechanism of action is directly via the skin.[5] This has been demonstrated with the observation that switching from one beta blocker to another results in re-introduction of psoriasiform skin lesions.[5] However, researchers have found that the cumulative drug exposure to beta blockers is not a substantial risk factor for development of psoriasiform lesions.[25] In psoriasiform eruptions, discontinuation alone can cause rapid regression of the disease.[4] If psoriasis is present only in localized areas, emollients alone can be helpful.[4] Exacerbation of psoriasis by beta blockers can be persistent and resistant to therapy unless they are discontinued.4 Management of drug-provoked psoriasis necessitates the use of conventional therapeutic agents that include topical and systemic agents used in the treatment of psoriasis vulgaris.[4] Treatment of erythroderma resulting from beta-blocker therapy should be targeted at decreasing transepidermal fluid loss.[26] Hospitalization is required to monitor hypovolemia and hemodynamic instability that requires aggressive fluid resuscitation.[26] These cases should be treated aggressively with systemic and topical agents in concordance with discontinuation of the offending drug.[26]
Lithium- and Drug-Provoked Psoriasis
Lithium is a metal ion that has been used extensively in the treatment of manic-depressive disorder since the 1970s.11 Although utilization of lithium is not as widespread as in the past, it is commonly prescribed. The first association of lithium with psoriasis was reported in 1972, and since then there have been several reports of lithium-induced psoriasis described in individuals with no personal or family history.[11] Toxic effects of lithium on organs other than the skin are dose related, with adverse events involving the thyroid, kidneys, central nervous system, and gastrointestinal tract.[11] Psoriasiform eruptions are the most common cutaneous side effects, reported to occur in 3.4 to 45 percent of patients treated with lithium.[27]
Pathogenesis of lithium-provoked psoriasis. There are several theories purported to explain the pathogenesis of lithium-provoked psoriasis. Induction and aggravation of psoriasis through cAMP are now being refuted by some investigators.16 In the past, researchers theorized that the decrease in cAMP from lithium treatment caused low intracellular levels of calcium, leading to a lack of differentiation, increased proliferation of keratinocytes, and enhanced chemotaxis and phagocytic activity of polymorphonuclear leukocytes.[28,29] Past studies have shown that the short-term use of lithium leads to diminution of intracellular cAMP, but long-term lithium treatment causes just the opposite response through a compensatory mechanism.[30,31] The current belief is that lithium causes depletion of inositol monophosphatase resulting in alterations in calcium homeostasis and seritonergic function.[5,32–34] Inositol is an intracellular second messenger system linked to neurotransmitters affecting cell function, growth, and differentiation.[5] The association between the blockade of the phosphatidyl inositol pathway and lithium-provoked psoriasis is through the release and depletion of intracellular calcium.[5] Low intracellular calcium levels cause increased proliferation of keratinocytes and affect terminal differentiation.[11] Lithium inhibits the enzyme inositol monophosphatase, necessary for the recycling of inositol.[11] The inhibition of the intracellular release of calcium appears to be the mechanism in which lithium provokes the development of a psoriasiform eruption.[35] The support for the ‘inositol depletion hypothesis’ comes from the clinical observation that inositol supplementation can reverse the exacerbation of lithium-provoked psoriasis.[16] In addition, studies have shown that lithium increases the production of interleukin-2 (IL-2), tumor necrosis factor-a (TNF-a), and interferon-gamma in psoriatic keratinocytes.[11] The dysregulation in the production of these cytokines has been linked to the induction of psoriatic lesions.[11] Lithium also increases intracellular tyrosine phosphorylation in psoriatic T cells but not in control T cells, with a possible implication to psoriasis lesion development.[16]
Clinical manifestation of lithium-provoked psoriasis. Reports of lithium-provoked psoriasis in the literature include new onset of pustular psoriasis, palmoplantar pustulosis, erythroderma, psoriasiform dermatitis, psoriatic arthropathy, and psoriasis involving the nail and scalp.[36] The most common presentation of lithium-provoked psoriasis is the classic plaque-type lesions.[5] Clinically and histologically, there is little difference between psoriasis vulgaris and lithium-provoked psoriasis.[37] In addition, elevated plasma concentrations of lithium have been found in patients with psoriasis who have never been treated with lithium compounds, suggesting a possible environmental factor.[38] There may be inherent factors that influence the induction or aggravation of psoriasis with lithium.11 When plaque-type psoriasis develops with lithium therapy, it may take longer to resolve compared to pustular psoriasis.[37] It has been suggested that exacerbation of pre-existing psoriasis is more common than induction of new psoriatic lesions.[39–40] While in some patients, there is a definite temporal relationship between aggravation of psoriasis with the initiation of lithium and improvement with discontinuation of the drug, this is not always the case.[27,41] The refractory period for the development of psoriatic lesions after the initiation of lithium treatment is variable and ranges from a few weeks to several months.[36] There have also been reports suggesting that production of psoriatic lesions can be temporally related to the improvement in mood symptoms due to cellular saturation with lithium ions.[36]
Management of lithium-provoked psoriasis. Sup-plementation with inositol in dietary consumption has sparked an interest in the treatment of psoriasis associated with lithium therapy. Peripheral inositols received in the form of dietary consumption do not cross the blood-brain barrier and therefore do not alter lithium effects on mood stabilization.[42] Studies have shown that patients with psoriasis on lithium therapy experience significant improvement after 6g of daily inositol supplementation by mouth with “dramatic improvement” within 48 to 72 hours.[43] A double-blind, randomized, placebo-controlled, crossover trial showed that inositol supplementation significantly improved the Psoriasis Area and Severity Index (PASI) scores in psoriasis patients on lithium compared to placebo.[5] In another double-blind, placebo-controlled trial, 4 to 6g/day of omega-3 fatty acid was found to be very useful in clearing acute lithium-induced psoriasis.[44] In addition, there has also been success with TNF-a inhibitors, such as etanercept, in the treatment of severe, recalcitrant, lithium-provoked psoriasis.[44–45] However, there are new reports suggesting the onset or exacerbation of psoriasis with TNF-a inhibitors possibly through elevation of cytokines or due to increased susceptibility to infections.[46] In evaluating lithium-provoked psoriasis, the role of stress and other psychological factors, as well as current medications, must be evaluated. Lithium-provoked psoriasis can be controlled with conventional treatments, such as topical corticosteroids, keratolytics, vitamin D analogues, oral retinoids, psoralen plus ultraviolet A (PUVA) therapy, and methotrexate.[36] Psoriatic lesions generally disappear within a few months after discontinuation of lithium treatment.[36] In some cases, patients can develop treatment-resistant psoriasis, which may warrant discontinuation of lithium with change to another mood-stabilizing agent (under close supervision of a psychiatrist) depending on the severity of cutaneous involvement.[40,47,48] Reduction in dosage of lithium is an additional option for treatment-resistant cases.[36] Yet, lithium-provoked psoriasis has been reported to occur at varying therapeutic levels and is not believed to be dose related.[49] It is advised that not all patients with psoriasis will have a flare-up with the initiation of lithium therapy, and psoriasis is not considered a contraindication to lithium use.[50]
Antimalarials and Drug-Provoked Psoriasis
The synthetic oral antimalarial (AM) agents are 4-aminoquinolone compounds that have been used in the prophylaxis and treatment of malaria and several dermatological disorders for many years.[11] The most commonly used oral AMs are chloroquine and hydroxychloroquine.[11] The exacerbation and induction of psoriasis during treatment with AMs has been widely acknowledged.[4] One mode of action of AMs is through the inhibition of transglutaminase in the skin, which is thought to influence cellular proliferation.[11] The inhibition of this enzyme can induce de-novo pustular psoriasis, which is notably uncommon compared to aggravation of pre-existing psoriasis.[51] Some patients may have minimal presence of pre-existing psoriatic lesions without being aware that these minor skin changes constitute psoriasis.[11] It has been shown that patients with psoriatic skin lesions after use of AMs had exacerbation of their psoriasis in 31 percent of cases.[52] The same study also reported the induction of psoriasis and pustular psoriasis during chloroquine therapy.[53,54] In another group, 42 percent (20/48) of American soldiers with psoriasis given chloroquine for the prophylaxis of malaria had exacerbation of psoriasis, which was treatment resistant.[55] Exacerbation of psoriasis has been reported with chloroquine treatment for psoriatic arthritis.[56–57] Psoriatic skin lesions most often occur with a latency of 2 to 12 weeks (average of 3 weeks) after starting AMs, with some patients exhibiting durations longer than 40.5 weeks, especially in cases of pustular eruptions occurring in those with pre-existing psoriasis.[4] Clinicians may be faced with a difficult decision in patients with simultaneous collagen vascular disease, such as progressive discoid or subacute cutaneous lupus erythematosus and psoriasis.4 Resolution of psoriatic lesions usually occurs within one month of discontinuing the AM agent.[11] The use of chloroquine and hydroxychloroquine in patients with psoriasis is considered by some to be a contraindication.[11]
Antibiotics and Drug-Provoked Psoriasis
A relationship between systemic antibiotics and drug-provoked psoriasis remains controversial. The tetracyclines are one group of antibiotics that have been described in association with psoriasis with no definitive latency period.[58] Tetracyclines may theoretically provoke psoriasis through reduction of intracellular cAMP and by the interaction with arachidonic acid and its metabolites.[59] It has been theorized that tetracyclines accumulate in higher concentrations in psoriatic lesions compared to uninvolved skin.[60] Some tetracyclines may cause photosensitization, which may result in predisposed patients with psoriasis to experience exacerbation through the Koebner phenomenon secondary to phototoxicity.[61–63] In one study, investigators reported that 4.11 percent (19/462) of patients experienced exacerbation of psoriasis as a consequence of tetracycline use.[4] It has also been suggested that tetracyclines should be avoided in patients with clinical evidence of psoriasis, as well as in healthy individuals with a genetic predisposition for psoriasis, such as in those with a positive family history or with HLA-B13, B17, and B27 genotypes.[4] The validity, practicality, and clinical relevance of these suggestions remain uncertain.
Reports suggest that exacerbation of psoriasis by penicillin derivatives is rare and may actually represent acute generalized exanthematous pustulosis and not true drug-provoked psoriasis.[65–66] Macrolides and penicillin derivatives were associated with psoriasis in one multivariate case-control model in patients less than 50 years of age.[64] Whether the actual drug intake or the infection itself is the inciting agent is still uncertain.[4] Therefore, clinicians should keep in mind that antibiotics may have been given as a treatment for presumed streptococcal infection, a known trigger of psoriasis development or exacerbation.[64]
Nonsteroidal Anti-Inflammatory Drugs and Drug-Provoked Psoriasis
NSAIDs are a class of medications used for treatment of pain and arthritides. NSAIDs are frequently used by patients who have psoriasis as well as psoriatic arthritis. NSAIDs are available by prescription and over the counter. NSAIDs inhibit the metabolism of arachidonic acid by the cyclo-oxygenase (COX) pathway leading to accumulation of leukotrienes, which has been postulated to aggravate psoriasis.[11] According to one study, both topical and systemic NSAIDs were the most common cause of both exacerbation and induction of psoriasis.[11] Of the NSAIDs, naproxen was the most common culprit.[67] Six patients had exacerbation of psoriasis after taking oral NSAIDs in a large study of 462 patients.[68] In another study, topical 1% indomethacin cream exacerbated psoriasis in 14 of 20 patients with known disease.[69] In case-controlled and case-crossover studies, there have been adverse side effects of NSAIDs reported in patients with psoriasis, particularly with proprionic acid derivatives.[69] The effects of NSAIDs have a short latency period (1.6 weeks on average) without significant variations between the different subsets of drug-provoked psoriasis.[4] Considering that patients with psoriasis can have associated arthropathies, it is important for clinicians to recognize NSAIDs as potential exacerbators of psoriasis. Nevertheless, in some patients, exacerbation of psoriasis and arthritis may coincidently occur simultaneously with the use of NSAIDs.
Angiotensin-Converting Enzyme Inhibitors and Drug-Provoked Psoriasis
Angiotensin-converting enzyme inhibitors (ACEI) are widely used to control hypertension. In an analysis of case-controlled and case-crossover studies, ACEIs were associated with psoriasis in patients greater than 50 years of age.[64] Although there are no current studies confirming a causal relationship between the two, ACEIs are considered to be possible triggering/exacerbating agents of psoriasis.[64] Recent studies suggest that patients with a history of familial psoriasis and a specific ACE genotype exhibiting low ACE activity are more susceptible to developing psoriasis after initiation of therapy.[70]
Other Drugs and Drug-Provoked Psoriasis
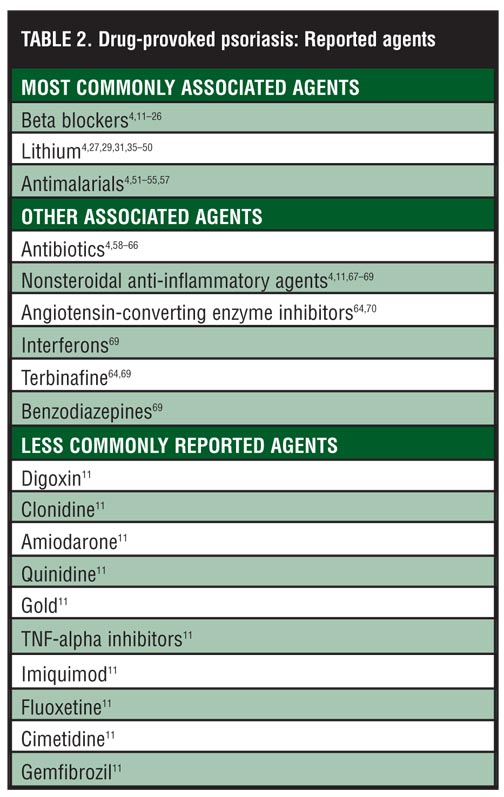
Drugs with considerable data in the induction/ exacerbation of psoriasis include interferons, terbinafine, and benzodiazepines.[64,69] There have also been reports of generalized pustular psoriasis in association with phenylbutazone.[4] Other miscellaneous drugs with a reported association with psoriasis include digoxin, clonidine, amiodarone, quinidine, gold, TNF-alpha inhibitors, imiquimod, fluoxetine, cimetidine, and gemfibrozil.[11] With an ever-expanding list of medications, investigators have suggested using the Adverse Drug Reactions Probability Scale in assessing the relationship between drugs and adverse reactions if a clinician is faced with a difficult decision in high-risk psoriasis patients on multidrug regimens.[71]
Conclusion
Several drugs have been associated with drug-provoked psoriasis (Table 2). Understanding the pathogenesis of drug-provoked psoriasis not only helps to achieve a greater appreciation of the disease process, but is also useful in providing guidance for treatment methodologies. In certain cases of drug-provoked psoriasis, lesions may become resistant to treatment and hence early recognition and management can help avoid issues of nonadherence. In general, most drugs tend to exacerbate psoriasis rather than induce it.[11] In cases where psoriasis is induced, one should question if this is truly a first-time occurrence or if previous subclinical signs may have gone undetected. Why provocation of psoriasis occurs in some individuals and not others who are exposed to a specific drug remains unclear. The absence of additional triggering factors should always be ruled out first. Patients should be encouraged to avoid alcohol, excessive sun exposure, smoking, and stress—factors that can all affect the clinical course of the disease. Management of drug-provoked psoriasis includes detailed personal, social, and family history. Provocation testing is also an option if a definitive relationship cannot be established. Drugs that are considered to have a strong potential risk factor for psoriasis development should be avoided after weighing the risk and benefits of the agent.[64] Fortunately, there are only a few drugs that demonstrate a well-documented, direct, causal relationship with the development of psoriasis or psoriasiform eruptions, and alternative therapeutic options are frequently available.
{kind=link}
References
1. Naldi L. Epidemiology of psoriasis. Curr Drug Targets Inflamm Allergy. 2004;3:121–128.
2. Raychaudhuri SP, Farber EM. The prevalence of psoriasis in the world. J Eur Acad Dermatol Venereol. 2001;15:16–17.
3. Zahl V, Gerdes S, Mrowietz U. Co-medication in patients with severe psoriasis: first results of a retrospective analysis in 1203 hospitalized patients in Germany. Presented at: the 4th International Congress-The Royal College of Physicians; December 1–3, 2005; London, England.
4. Tsankov N, Irena A, Kasandjieva J. Drug-induced psoriasis: recognition and management. Am J Clin Dermatol. 2000;1:159–165.
5. O’Brian M, Koo J. The mechanism of lithium and beta-blocker agents in inducing and exacerbating psoriasis. J Drugs Dermatol. 2006;5:426–433.
6. Sehgal V, Dogra S, Srivastava G, et al. Psoriasiform dermatoses. Indian J Dermatol Venereol Leprol. 2008;74: 94–99.
7. Weedon D, Strutton G. Psoriasiform tissue reactions. In: Weedon D, ed. Skin Pathology. 2nd ed. New York, NY: Churchill Livingstone; 2002:76–79.
8. Ackerman AB. A method of pattern analysis. In: Histologic Diagnosis of Inflammatory Skin Disease. Philadelphia, Pa: Lea and Febiger; 1978:124–126.
9. Mihm MC. Psoriasiform dermatitis. In: Hood AF, Kwan TH, Mihm MC, et al, eds. Primer of Dermatopathology. Boston, Mass.: Little Brown; 1993:102–106.
10. Smotter BR. Psoriasiform dermatitis. In: Pathology of the Skin. Farmer ER, Hood AF, eds. 1st ed. New York, NY: McGraw Hill; 2000:170–174.
11. Lionel F, Baker B. Triggering psoriasis: the role of infections and medications. Clin Dermatol. 2007;25:606–615.
12. Assem ESK, Banks RA. Practolol induced drug eruptions. Proc R Soc Med. 1973;66:179–181.
13. Halevy S, Livni E. Psoriasis and psoriasiform eruptions associated with propranolol—the role of an immunological mechanism. Arch Dermatol Res. 1991;238:472–473.
14. Raftery EB, Denman AM. Systemic lupus erythematosus syndrome induced by practolol. BMJ. 1973;2:452–455.
15. Heng MC, Heng MK. Beta-adrenoceptor antagonist-induced psoriasiform eruption. Clinical and pathogenetic aspects. Int J Dermatol. 1988; 27(9):619–627.
16. Ockenfels HM, Nussbaum G, Schultewolter T, et al. Tyrosine phosphorylation in psoriasis T cells is modified by drugs that induce or improve psoriasis. Dermatology. 1995;191: 217–225.
17. Jenson H, Mikkelsen I, Wadskov F, et al. Cutaneous reactions to propranolol (Inderal). Acta Med Scad. 1976;199:363–367.
18. Steinkraus V, Steinfath M, Mensing H. Beta-adrenergic blocking drugs and psoriasis. J Am Acad Dermatol. 1992;27:266–267.
19. Halevy S, Livni E. Beta-adrenergic blocking drugs and psoriasis: the role of an immunologic mechanism. J Am Acad Dermatol. 1993;29:504–505.
20. Halevy S, Livni E. Psoriasis and psoriasiform eruptions associated with propranolol—the role of an immunologic mechanism. Arch Dermatol Res. 1991;283:472–473.
21. Tsankov N, Pramatarov K, Kamarachev J. Psoriasis placat, die unter der Einwirkung der beta blocker in eine psoriasis. Dtsch Dermatologe. 1992;40:1702–1706.
22. Hu CH, Miller CM, Pepperkorn R, et al. Generalized pustular psoriasis provoked by propranolol. Arch Dermatol. 1985;121:1326–1327.
23. Coignet M, Sayag J. Collyre beta bloquant et psoriasis. Dermatology. 1990;9:552.
24. Puig L, Goni FJ, Roque AM, et al. Psoriasis induced by ophthalmic timolol preparations. Am J Ophthalmol. 1989;108:445–446.
25. Brauchli YB, Jick SS, Meier C. Association between beta-blockers, other antihypertensive drugs and psoriasis: population-based case-control study. Br J Dermatol. 2008;158:1299–1307.
26. Waqar S, Sarkar P. Exacerbation of psoriasis with beta blocker therapy. CMAJ. 2009;181:1–2.
27. Carter TN. The relationship of lithium carbonate to psoriasis. Psychosomatics. 1972;13(5):325–327.
28. Voorhees JJ, Marcelo CL, Duell EA. Cyclic AMP, cyclic GMP and clucocorticoids as potential metabolic regulators of epidermal proliferation and differentiation. J Invest Dermatol. 1975;65(1):179–190.
29. Bloomfield FJ, Young MM. Enhanced release of inflammatory mediators from lithium-stimulated neutrophils in psoriasis. Br J Dermatol. 1983;109(1)9–13.
30. Di Giovanna JJ, Aoyagai T, Taylor RT. Inhibition of epidermal adenyl cyclase by lithium carbonate. J Invest Dermatol. 1981;76:759–763.
31. Beyaert R, Schulze-Osthoff K, Van Roy F. Synergistic induction of interleukin-6 by tumor necrosis factor and lithium chloride in mice: possible role in the triggering and exacerbation of psoriasis by lithium treatment. Eur J Immunol. 1992;22:218–224.
32. Hwang SM, Ahn SK, Menon GK, et al. Basis of occlusive therapy in psoriasis: correcting defects in permeability barrier and calcium gradient. Int J Dermatol. 2001;40(3):223–231.
33. Odagaki Y, Koyama Y, Yamashita I. Lithium and serotonergic neural transmission: a review of pharmacological and biochemical aspects in animal studies. Lithium. 1992;100: 3–12.
34. Hamlock C, Rosenthal JS, Winston A. Fluoxetine-induced psoriasis. Ann Pharmacother. 1992;26:211–212.
35. Gill R, Mohammed R, Badyal R, et al. High resolution structure of myo-inositol monophosphatase, the putative taret of lithium therapy. Acta Crystallogr D Biol Crystallogr. 2005;61:545–555.
36. Jafferany M. Lithium and psoriasis: what primary care and family physicians should know. Prim Care Companion J Clin Psychiatry. 2008;10:435–439.
37. Abel EA, DiCicco LM, Orenberg EK, et al. Drugs in exacerbation of psoriasis. J Am Acad Dermatol. 1986;15: 1007–1022.
38. Hanada K, Tasaki M, Hashimoto I, et al. Development of psoriasis-like syndrome following lithium therapy. Biol Trace Elem Res. 1978;14:169–177.
39. Sarantidis D, Waters B. A review and controlled study of cutaneous conditions associated with lithium carbonate. Br J Psychiatry. 1983;143:42–50.
40. Skoven I, Thormann J. Lithium compound treatment and psoriasis. Arch Dermatol. 1979;115:1185–1187.
41. Bakker JB, Pepplinkhuizen L. More about the relationship of lithium to psoriasis. Psychosomatics. 1976;17:143–146.
42. Allan SJR, Kavanagh GM, Herd RM, Savin JA. The effect of inositol supplements on the psoriasis of patients taking lithium: a randomized, placebo-controlled trial. Br J Dermatol. 2004;150:966–969.
43. Grisaru N, Blemaker RH. Ltihium dosage and inositol levels. Br J Psychiatry. 1994;164(1):133–134.
44. Akkerhuis G, Nolen W. Lithium associated psoriasis and omega-3 fatty acids. Am J Psychiatry. 2003;160:7.
45. Watchter T, Murach WM, Brocker EB, et al. Recalcitrant lithium-induced psoriasis in a suicidal patient alleviated by tumor necrosis factor-alpha inhibition. Br J Dermatol. 2007;157(3):627–629.
46. Wendling D, Blablanc J, Briancon D, et al. Onset or exacerbation of cutaneous psoriasis during TNF alpha antagonist therapy. Joint Bone Spine. 2008;75:315–318.
47. Selmanowitz VJ. Lithium, leukocytes and lesions. Clin Dermatol. 1986;4(1):170–175.
48. Alvarez WA, Freinhar JP. Direct evidence for lithium-induced psoriasis syndrome. Int J Psychosom. 1984;31:21–22.
49. Evans DL, Martin W. Lithium carbonate and psoriasis. Am J Psychiatry. 1979;136:1326–1327.
50. Skoven I, Thormann J. Lithium compound treatment and psoriasis. Arch Dermatol. 1979;115:1185–1187.
51. Wolf R, Schiavo AL. Is transglutaminase the mediator between antimalarial drugs and psoriasis. Int J Dermatol. 1997;36:10–13.
52. Slagel GA, James WD. Plaquentil induced erythroderma. J Am Acad Dermatol. 1985;12:857–862.
53. Baker H. The influence of chloroquine and related drugs on psoriasis and kertoderma blenorrhagium. Br J Dermatol. 1966;78:161–166.
54. Friedman SS. Pustular psoriasis associated with hydroxyl chloroquine. J Am Acad Dermatol. 1987;16:1256–1257.
55. Kufik EG. Effect of anti-malarial drugs on psoriasis. Cutis. 1980;26:153–155.
56. Bessis D, Moles JP, Basset-Seguin N, et al. Differential expression of a human endogenous retrovirus E transmembrane envelope glycoprotein in normal, psoriatic and atopic dermatitis human skin. Br J Dermatol. 2004;151: 737–745.
57. Trnavsky K, Zbojanova M, Vloek F. Antimalarials in psoriatic arthritis. J Rheumatol. 1983;10:833.
58. Botev-Slatkov N, Tsankov N, Tonev S, et al. Drug therapy deteriorates the course of psoriasis. Presented at: 17th World Congress of Dermatology, Part II; West Berlin: Springer; 1987:216.
59. Counis R, Koumanov K, Ranlin J, et al. Intepretation du role antilipolytique de la tetracycline. Inhibition de l’adenylate cyclase in vitro. Eur J Biochem. 1973;37:244–247.
60. Forster S, Ilderton E, Summerly R, et al. The level of phospholipase A2 activity is raised in uninvolved epidermis of psoriasis. Br J Dermatol. 1983;108:103–105.
61. Boothe JH. The tetracyclines. In: Hlavka JJ, ed. Handbook of Experimental Pharmacology. Vol 78. The Tetracyclines. Berlin: Springer-Verlag; 1985:451.
62. Wright AL, Colver GB. Tetracyclines-how safe are they? Clin Exper Dermatol. 1988;13:57–61.
63. Powles AV, Baker BS, Rutman AJ, et al. Epidermal rupture is the initiating factor for the Koebner response in psoriasis. Acta Derm Venereol. 1990;70:35–38.
64. Katz M, Seidenbaum M, Weinrauch L. Penicillin-induced generalized pustular psoriasis. J Am Acad Dermatol. 1987;17:918–920.
65. Sidoroff A, Halevy S, Bowes-Bavinck JN, et al. Acute generalized exanthematous pustulosis (AGEP)—a clinical reaction patter. J Cutan Pathol. 2001;28:113–119.
66. Cohen A, Bonneh D, Reuveni H, et al. Drug exposure and psoriasis vulgaris: case-control and case-crossover studies. Acta Derm Venereol. 2005;85:299–303.
67. Grau R. Drug-induced psoriasis—A retrospective chart review performed at the University of Oklahoma Department of Dermatology. J Am Acad Dermatol. 2008;59:P2647.
68. Ellis CN, Fallon JD, Heezen JL, et al. Topical indomethacin exacerbates lesions of psoriasis. J Invest Dermatol. 1983;80:362.
69. Cohen AD, Bonneh DY, Reuveni M, et al. Drug exposure and psoriasis vulgaris: case-control and case-crossover studies. Acta Derm Venereol. 2005;85:299–303.
70. Chang YC, Wu WM, Chen CH, et al. Association between the insertion/deletion polymorphism of the angiotensin I-converting enzyme gene and risk for psoriasis in a Chinese population in Taiwan. Br J Dermatol. 2007;156:642–645.
71. Naranjo CA, Busto U, Seller EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–245.