Peter G. Pavlidakey, MD, Department of Pathology, Case Western Reserve University School of Medicine, Cleveland, Ohio; Erin E. Brodell, University of Richmond; Associate Professor of Internal Medicine, Northeastern Ohio Universities School of Medicine, Rootstown, Ohio; Stephen E. Helms, MD, Assistant Professor of Dermatology, Case Western Reserve University School of Medicine, Cleveland, Ohio
Abstract
Patients who present with a history of “allergy” to local anesthetics are common in clinical practice. Injectable 1% diphenhydramine is a safe, inexpensive, and effective local anesthetic for simple dermatological procedures in patients who report “caine” allergies. Utilizing this agent permits the dermatologist to operate at the time of the initial visit and schedule a referral to the allergist for definitive sensitivity testing at the patient’s convenience. (J Clin Aesthetic Dermatol. 2009;2(10):37–40.)
Diphenhydramine hydrochloride (DPH) has numerous pharmacological uses in medicine. It is a first-generation, sedating, oral antihistamine. When topically applied, DPH has excellent anesthetic and antipruritic effects. DPH has also been shown to be an effective injectable drug for local anesthesia. This may be due to its three-dimensional structure, which is similar to other anesthetic drugs.[1,2] The authors present a patient whose history of a severe “allergic” reaction to a “caine” local anesthetic prompted the use of 1% DPH to allow same-day surgery and avoid any possibility of a potentially life-threatening reaction.
Case Report
A 51-year-old man presented for evaluation of a freely movable 2cm diameter “cyst” on his back. He reported experiencing an allergy to Novocain© (procaine) during a procedure at the dentist’s office 30 years previously. Symptoms included pounding in the chest and light-headedness, which occurred immediately following the injection of the local anesthetic. An emergency room visit eventuated in a 24-hour admission to the hospital. The medical record from this incident was not available. The patient assiduously avoided local anesthetic injections following this event.
A referral to an allergist for definitive testing of a “caine” allergy was considered and discussed with the patient. However, to permit “same-day” surgery, 1cc of DPH 10mg/mL was used as a local anesthetic. The patient experienced no pain and had no untoward side effects during the cyst removal using a punch incision/cyst extraction technique.
Discussion
The cause of this patient’s reaction 30 years earlier is unclear. Vasovagal reactions result from increased sympathetic activity in response to fear, pain, or the sight of blood. This causes a burst of parasympathetic activity leading to light-headedness, fainting, and sometimes clonic limb jerking associated with a slow heart rate.[3] Vasovagal reactions do not produce “pounding” in the chest. Most likely, this patient had a pharmacological reaction to epinephrine or an anaphylactic reaction to the injectable anesthetic itself.
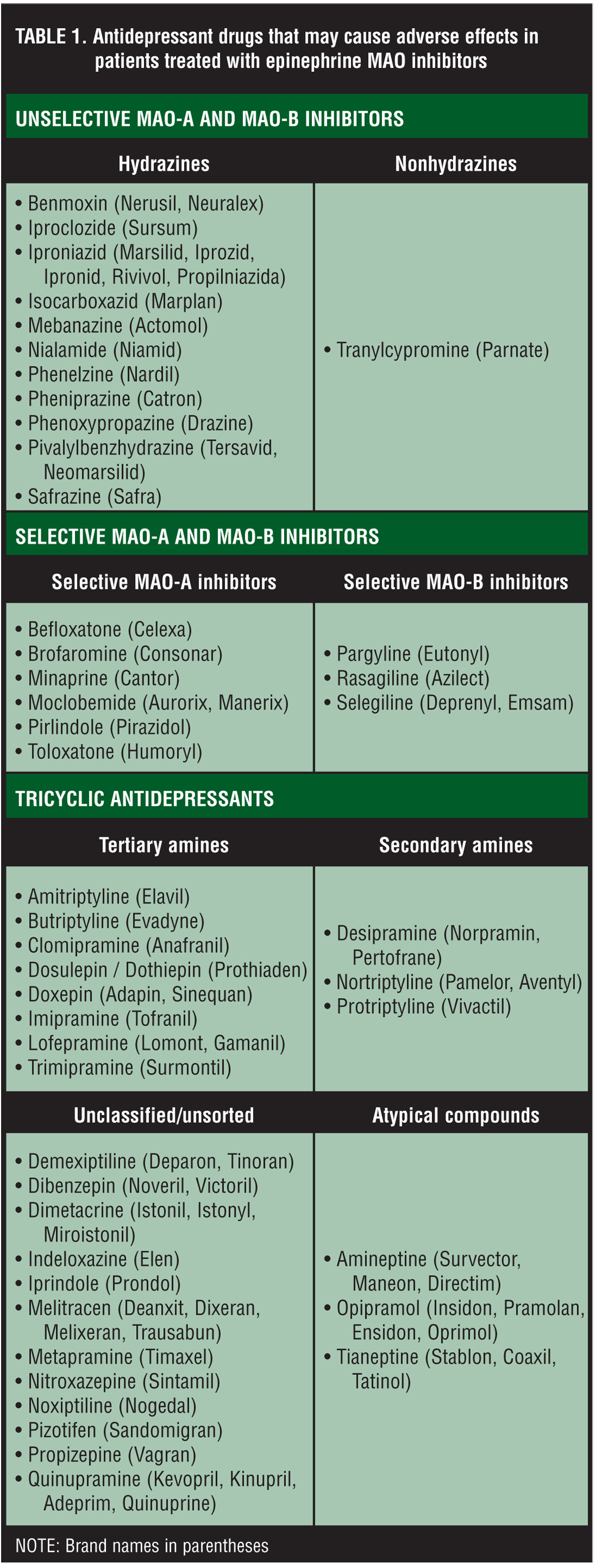
Epinephrine is combined with injectable anesthetics to decrease bleeding during surgery and prolong anesthetic effects.[4] Although small amounts of epinephrine in local anesthetics usually cause no reaction, rare idiosyncratic reactions have been reported, which could include pounding in the chest and light-headedness experienced by our patient.[4] Interestingly, epinephrine, when given in the presence of a beta blocker, can cause unopposed alpha-agonist activity leading to a dramatic increase in blood pressure.[4] It has also been recommended that epinephrine not be given with monoamine oxidase inhibitors (MAOI) or tricyclic antidepressants (Table 1). This can cause augmented pharmacological effects, including palpitations, tachycardia, sweating, nausea, vomiting, respiratory difficulty, pallor, dizziness, weakness, tremor, headache, and anxiety.[4] There is debate, however, about whether the amount of epinephrine used in small dermatological procedures could produce clinically significant effects in these patients.[5]
{kind=link}
Reactions to “caine” local anesthetics, when limited to the injection site, are caused by type 4 hypersensitivity reactions.4 Signs may include localized or widespread pruritic and erythematous macules, patches, papules, vesicles, and plaques.[4–7] The more severe immunoglobulin E (IgE)-mediated anaphylactic reactions represent less than one percent of allergies to local anesthetics.[5,8] Patients may be exposed to an allergen many times without any reaction, but once sensitization has occurred, a similar response is expected each time the antigen is presented. Anaphylaxis is associated with a decrease in blood pressure caused by increased permeability of the capillary bed. Clinically, this produces a rapid heart beat, urticaria, stridor, wheezing, angioedema, light-headedness, fainting, nausea, and sometimes death.[5,8,9]
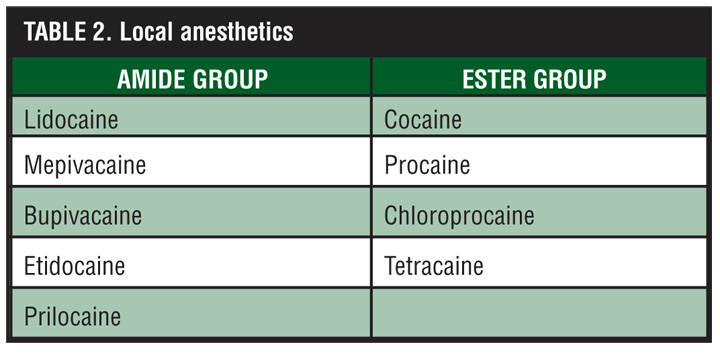
Careful consideration of the medical history and review of available medical records are critical steps in the evaluation of patients. If a reaction is determined to be the result of epinephrine, a “caine” anesthetic without epinephrine could be administered. However, if there is any chance of an anaphylactic reaction to “caine” anesthetic in the past, there is potential for a significant, even life-threatening, event with re-introduction of the local anesthetic. Most type 1 IgE-mediated reactions are caused by ester anesthetics while amide anesthetics only very rarely cause these reactions (Table 2).[3] While allergy cross-reactivity occurs between various ester anesthetics and within the amide class, there is no cross-reactivity between ester and amide anesthetics. In summary, if the identity of the offending anesthetic (usually an ester) can be determined with certainty in a patient with true IgE-mediated allergic reactions, an amide in a preservative-free solution could be utilized. However, in the vast majority of cases in the outpatient setting, it is impossible to determine exactly which anesthetic was utilized prior to the allergic reaction. In this case, referral to an allergist for testing is suggested.[10]
{kind=link}
Scratch testing followed by subcutaneous challenge with increasing concentrations of the suspected allergen is the definitive method to determine if the patient is likely to suffer anaphylaxis with future exposure to “caine” anesthetics. Histamine and saline controls are also used at the time of testing. If the scratch test is positive to a sample of the local anesthetic, no further testing is needed and these patients should not be given that particular class of injectable “caine” anesthetic. If scratch tests are negative, subcutaneous challenge may be performed with increasing concentrations of local anesthetic, testing from most diluted to full-strength medication. False-negative tests would not be expected since this mimics the injection of a local anesthetic. However, false-positive tests have been reported frequently in intradermal skin testing.[1,11–17]
A comprehensive, algorithmic approach to evaluating hypersensitivity to local anesthetics was recently proposed.18 Interestingly, allergists will sometimes choose not to perform this testing when the evidence of anaphylaxis is strong, since anaphylaxis can result from the use of testing materials. Furthermore, some patients may choose not to undergo allergy testing because of additional costs. However, the cost of this testing in the allergist’s office is reasonable when the benefits from testing are realized. Medicare allowable charges (MAC) in the authors’ region include the following: 1) new patient consultation ($122.06, CPT 99243); 2) scratch testing with positive and negative controls ($5.77/scratch x 3 = $17.31, CPT 95004); and 3) subcutaneous challenge ($12.62/dilution or full strength x 5 = $63.10, CPT 95015). Therefore, the total cost of this evaluation would be $202.47.
Recognizing that there is always a risk of an anaphylactic reaction during the allergy testing procedure, there are several important reasons why the dermatologist may choose to refer patients for “caine” allergy testing.[10] First, patients who are confirmed to have anaphylactic reactions to local anesthetics should be identified and wear a bracelet to notify healthcare providers of this fact in an emergency. This may prevent a patient with a significant history of “caine” anaphylaxis from receiving this drug in the setting of cardiac arrhythmia or as a local anesthetic. Similarly, patients who have incorrectly been labeled as allergic to “caine” anesthetics should be identified so that they can receive the “caine” drugs they need without delay. Secondly, patients may someday need dental or other, more extensive surgical procedures that require a regional anesthetic block. As noted above, DPH is contraindicated in this setting. Finally, the cost of this testing is reasonable, and most insurance benefit plans cover these costs.
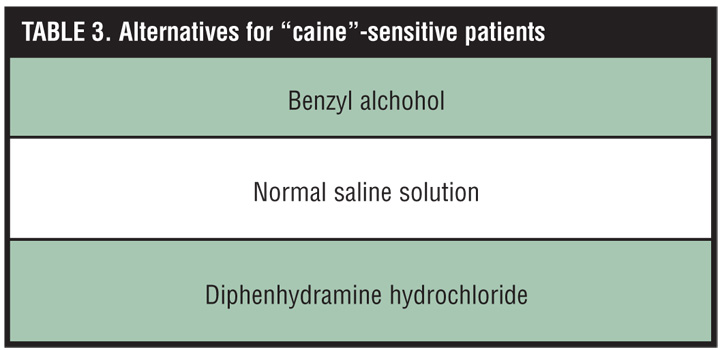
Whether or not a referral to an allergist is made, same-day surgery is possible if an alternative local anesthetic is chosen that does not cross react with “caine” agents (Table 3). Benzyl alcohol has been used as a local anesthetic with some success and these injections have been shown to be less painful than buffered lidocaine.[2] However, its utility is limited because of its rapid absorption.[19–21] This problem can be reduced when epinephrine is combined with benzyl alcohol.[19,20] This approach has two main drawbacks. First, the duration of anesthesia of benzyl alcohol/epinephrine is still shorter than that of lidocaine. Secondly, this approach is not viable in patients whom epinephrine is contra-indicated or in patients whom epinephrine may have played a role in previous reactions. Surprisingly, normal saline has also been shown to provide adequate local anesthesia in small areas of the skin. It was found to be less painful upon injection than lidocaine and provided adequate anesthesia when inserting intravenous catheters.[22] In the absence of a clear mechanism of action that correlates with this effect, we are skeptical that this approach would produce uniform results.
{kind=link}
DPH 1% solution is our favored alternative. It has been utilized since 1939 in the realm of dental anesthesia, surgery, and in the emergency room in patients who are allergic to local anesthetics.[1,2,6,23–27] DPH is an ideal choice since it provides adequate anesthesia and has no allergic cross reactivity to “caine” anesthetics.[1,2] A local injection of 1% DPH provides adequate anesthesia for 80 percent of people within five minutes.[25] The duration of anesthesia is between 15 minutes and three hours, which is adequate for most common dermatological procedures.[2,23–25] DPH is also inexpensive. The average wholesale cost (AWP) of 5% DPH is about 24 cents/cc. By comparison, injectable lidocaine costs 15 cents/cc. To prepare a 1% solution of DPH (10mg/cc), 10cc of normal saline is removed from a 50cc vial and discarded. Ten cc’s of 5% DPH are then injected into the remaining saline.
When 1% DPH is used as a local anesthetic, side effects may occur. Sedation is dose related, and caution is advised with driving when more than 25mg (2.5cc of 1% DPH) is injected.[1,6] In younger children, the total dosage should be adjusted according to body weight. These are volumes that provide successful anesthesia for most small dermatological procedures. The soporific effects of DPH are potentiated in patients taking sedatives.[24] DPH has been reported to cause more injection-related pain than lidocaine when administered for local anesthesia.[1,21,25,26,28] Interestingly, buffering does not appear to reduce pain of local injections with DPH.[29] Vesicle formation, erythema, rebound hyperesthesia, and tissue irritation rarely occur.[1,25,26,30] Skin sloughing has been reported using 5% diphenhydramine, but this has not been reported with 1% diphenhydramine.[1,2,25] DPH is contraindicated in patients with a history of allergic contact dermatitis to topical DPH or previous allergic reactions to oral or intramuscular DPH. In addition, we do not recommend use of DPH for digital blocks that have been associated with prolonged patchy anesthesia and paraesthesia.[2,28,31] Relative contraindications of DPH include pregnancy, nursing, asthma, narrow angle glaucoma, peptic ulcer, benign prostatic hypertrophy, and obstructive bowel disease.[24]
Conclusion
DPH 1% solution is a safe, effective, inexpensive alternative to “caine” local anesthetics. This allows same-day surgery in patients with a confirmed history of “caine” anesthetic reactions and in patients with a questionable history who have not had definitive allergy testing. Dermatologists should counsel patients about the advantages of referral to an allergist for definitive testing.
References
1. Green SM, Rothrock SG, Gorchynski J. Validation of diphenhydramine as a dermal local anesthetic. Ann Emerg Med. 1994;23(6):1284–1289.
2. Bartfield JM, Jandreau SW, Raccio-Robak N. Randomized trial of diphenhydramine versus benzyl alcohol with epinephrine as an alternative to lidocaine local anesthesia. Ann Emerg Med. 1998;32(6):650–654.
3. Hruza G. Anesthesia. In: Bolognia JL, ed. Dermatology. New York: Mosby; 2003:2235–2236.
4. Adriani J, Zepernick R. Allergic reactions to local anesthetics. South Med J. 1981;74(6):694–699,703.
5. Fenwick MJ, Muwanga CL. Anaphylaxis and monoamine oxidase inhibitors—the use of adrenaline. J Accid Emerg Med. 2000;17(2):143–144.
6. Huether MJ, Brodland DG. Local anesthetics. In: Wolverton SE, ed. Comprehensive Dermatology. New York: WB Saunders; 2001:736–766.
7. Dance D, Basti S, Koch DD. Use of preservative-free lidocaine for cataract surgery in a patient allergic to “caines.” J Cataract Refract Surg. 2005;31(4):848–850.
8. Winton GB. Anesthesia for dermatologic surgery. J Dermatol Surg Oncol. 1988;14(1):41–54.
9. Schatz M, Fung DL. Anaphylactic and anaphylactoid reactions due to anesthetic agents. Clin Rev Allergy. 1986;4(2):215–227.
10. Austin KF. Disorders of the immune system, connective tissue, and joints. In: Kasper DL, Baunwald E, Hauser S, Longo D, Jameson JL, Fauci AS, eds. Harrisons Principles of Internal Medicine, 16th ed. New York: McGraw- Hill; 2004:1949–1953.
11. Glinert RJ, Zachary CB. Local anesthetic allergy. Its recognition and avoidance. J Dermatol Surg Oncol. 1991;17(6):491–496.
12. Koay J, Orengo I. Application of local anesthetics in dermatologic surgery. Dermatol Surg. 2002;28(2):143–148.
13. Incaudo G, Schatz M, Patterson R, Rosenberg M, Yamamoto F, Hamburger RN. Administration of local anesthetics to patients with a history of prior adverse reaction. J Allergy Clin Immunol. 1978;61(5):339–345.
14. deShazo RD, Nelson HS. An approach to the patient with a history of local anesthetic hypersensitivity: experience with 90 patients. J Allergy Clin Immunol. 1979;63(6):387–394.
15. Chandler MJ, Grammer LC, Patterson R. Provocative challenge with local anesthetics in patients with a prior history of reaction. J Allergy Clin Immunol. 1987;79(6): 883–886.
16. Swanson JG. Assessment of allergy to local anesthetic. Ann Emerg Med. 1983;12(5):316–318.
17. Giovannitti JA. Evaluation of local anesthetic hypersensitivity reactions. Clin Prev Dent. 1982;3:20–22.
18. Boren E, Teuber SS, Naguwa SM, Gershwin ME. A critical review of local anesthetic sensitivity. Clin Rev Allergy Immunol. 2007;32(1):119–128.
19. Thyssen JP, Menne T, Elberling J, Plaschke P, Johansen JD. Hypersensitivity to local anaesthetics—update and proposal of evaluation algorithm. Contact Dermatitis. 2008;59(2):69–78.
20. Bartfield JM, May-Wheeling HE, Raccio-Robak N, Lai SY. Benzyl alcohol with epinephrine as an alternative to lidocaine with epinephrine. J Emerg Med. 2001;21(4):375–379.
21. Wilson L, Martin S. Benzyl alcohol as an alternative local anesthetic. Ann Emerg Med. 1999;33(5):495–499.
22. Wightman MA, Vaughan RW. Comparison of compounds used for intradermal anesthesia. Anesthesiology. 1976;45(6):687–689.
23. Windle PE, Kwan ML, Warwick H, Sibayan A, Espiritu C, Vergara J. Comparison of bacteriostatic normal saline and lidocaine used as intradermal anesthesia for the placement of intravenous lines. J Perianesth Nurs. 2006;21(4):251–258.
24. Uckan S, Guler N, Sumer M, Ungor M. Local anesthetic efficacy for oral surgery: comparison of diphenhydramine and prilocaine. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;86(1):26–30.
25. Gallo WJ, Ellis E 3rd. Efficacy of diphenhydramine hydrochloride for local anesthesia before oral surgery. J Am Dent Assoc. 1987;115(2):263–266.
26. Dire DJ, Hogan DE. Double-blinded comparison of diphenhydramine versus lidocaine as a local anesthetic. Ann Emerg Med. 1993;22(9):1419–1422.
27. Ernst AA, Marvez-Valls E, Mall G, et al. 1% lidocaine versus 0.5% diphenhydramine for local anesthesia in minor laceration repair. Ann Emerg Med. 1994;23(6):1328–1332.
28. Ernst AA, Anand P, Nick T, Wassmuth S. Lidocaine versus diphenhydramine for anesthesia in the repair of minor lacerations. J Trauma. 1993;34(3):354–357.
29. Howard K, Conrad T, Heiser J, Manzi JA. Diphenhydramine hydrochloride as a local anesthetic. A case report. J Am Podiatry Assoc. 1984;74(5):240–242.
30. Singer AJ, Hollander JE. Infiltration pain and local anesthetic effects of buffered vs plain 1% diphenhydramine. Acad Emerg Med. 1995;2(10):884–888.
31. Nuttall GA, Barnett MR, Smith RL 2nd. Establishing intravenous access: a study of local anesthetic efficacy. Anesth Analg. 1993;77(5):950–953.