Michael H. Gold, MD; Tennessee Clinical Research Center, Nashville, Tennessee; Anneke Andriessen; RBC Consultants, The Netherlands; Julie Biron; Tennessee Clinical Research Center, Nashville, Tennessee; Hinke Andriessen; RBC Consultants, The Netherlands
Abstract
This study was an evaluation of the performance of self-applied, blue light, light-emitting diode therapy in the treatment of mild-to-moderate inflammatory acne on the face, concerning: 1) time to improvement and/or resolution of the number of blemishes and lesions on the face; 2) quality of skin condition; 3) occurrence and count of the number of new blemishes and lesions; and 4) ease of product use; patient comfort, wellbeing, and satisfaction during the treatment period; and safety of treatment. Subjects (N=21) were included according to the inclusion/exclusion criteria and after they had given informed consent. The blue light treatment was conducted over an eight-week period. For study data management and analysis, SPSS 16.0 statistical software was used. Data management and analysis was performed independently using, where appropriate, ANOVA, student t-test, and Mann-Whitney test for N=20. Tests were carried out at the five-percent significance level. The confidence interval was 95 percent. Twenty-one subjects concluded the study (18/21 were female and 3/21 were male). Upon the first outbreak of acne, subjects had a mean age of 15 years (range 8–28 years), and 19 subjects had mild-to-moderate acne for a mean duration of 13.1 years. During the study period with self-applied blue light treatment, the total number of comedones on the face had significantly reduced for the assessment at Day 7 (p<0.019) and at Day 28 (p<0.001). The total number of open comedones (blackheads) on the face during the treatment period was reduced significantly (p<0.02) for assessment at treatment Day 7 (p<0.005) and for the assessment at Day 28. The total number of closed comedones (whiteheads) on the face during the treatment period, was reduced significantly (p<0.007) for the assessment at Day 28. The total number of papules during treatment had reduced significantly for assessment at Day 7 (p<0.048) and Day 28 (p<0.005). The total number of pustules during treatment had reduced, but this difference was not statistically significant. This was similar for nodules present. Subjects expressed confidence in using the self-applied blue light without the supervision of a doctor. Regarding previous treatments, subjects expressed dissatisfaction and considered self-applied blue light treatment to be better for their condition. Self-applied blue light treatment was reported to be easy and safe to use.
(J Clin Aesthetic Dermatol. 2009;2(3):44–50)
**********************************************************************************************************************************
Subjects who suffer from mild-to-moderate acne are generally treated with over-the-counter topical cleansers, astringents, and benzoyl peroxide preparations. For more severe flare-ups, they may receive treatment from healthcare providers with topical or systemic antibiotics.[1]
Increasingly, Propionibacterium acnes has been reported to develop resistance to antibiotic treatment, making this modality less effective.[2] Moreover, patients often feel the psychological pain of the few effective treatments and of chronic persistence and recurrence of their acne.[3]
Phototherapy with visible light, specifically blue light, has been shown to improve skin condition in cases of acne and blemishes.[4] It is further reported to control the condition before an outbreak occurs. This blue light therapy is clinically shown to control acne without harsh chemicals or prescriptions and improves the skin’s appearance.
Tända™ Clear Acne Light Therapy Treatment (Pharos Life Corporation, Cambridge, Ontario, Canada) is blue light therapy. It is noninvasive and designed for self-care use. This treatment is drug free without any form of unfavorable side effects. It does not cause redness, flakiness, or dry skin.
Mild-to-moderate acne
Acne vulgaris is a common skin condition affecting 70 percent of adolescents[2] and frequently continues into adulthood.[5–7] The mainstay of treatment of acne is the use of topical or systemic antibiotics, benzoyl peroxide preparations, and topical or systemic retinoids.[7]
The rapid increase in the incidence of antibiotic resistance in the causative bacterium P. acnes is of concern and there is a pressing need for effective, nonantibiotic treatments.[8]
Acne often improves after exposure to sunlight or artificially produced solar radiation. P. acnes produce mainly coproporphyrin III, which has an absorption spectrum peak at 415nm.[9] In-vitro irradiation of P. acnes colonies with blue visible light leads to photo-excitation of endogenous bacterial porphyrin, singlet oxygen production, and bacterial destruction.[10]
It has been shown both in vivo and clinically that acne may be treated successfully with blue visible light phototherapy.[10]
Current treatment for mild-to-moderate acne
Topical and oral antibacterials, such as tetracycline and erythromycin, are the mainstay of treatment for acne vulgaris. Antimicrobial therapy usually lasts a minimum of several months and can continue for years. More recently, other oral formulations, including minocycline, doxycycline, and trimethoprim, have been widely used.[7,11]
Oral isotretinoin is considered to be the most effective acne treatment currently available. It is reported to induce long-term remission in some individuals. The indications for use of isotretinoin have recently been broadened from nodulocystic acne to less severe forms of acne, including mild-to-moderate disease that fails to respond to systemic antimicrobials or acne associated with severe psychological problems.[7] However, isotretinoin is highly teratogenic, and women must avoid pregnancy during treatment and for one month after treatment. It frequently produces significant mucocutaneous symptoms and, less frequently, systemic symptoms, such as myalgia, headaches, and depression.[11]
Materials and methods
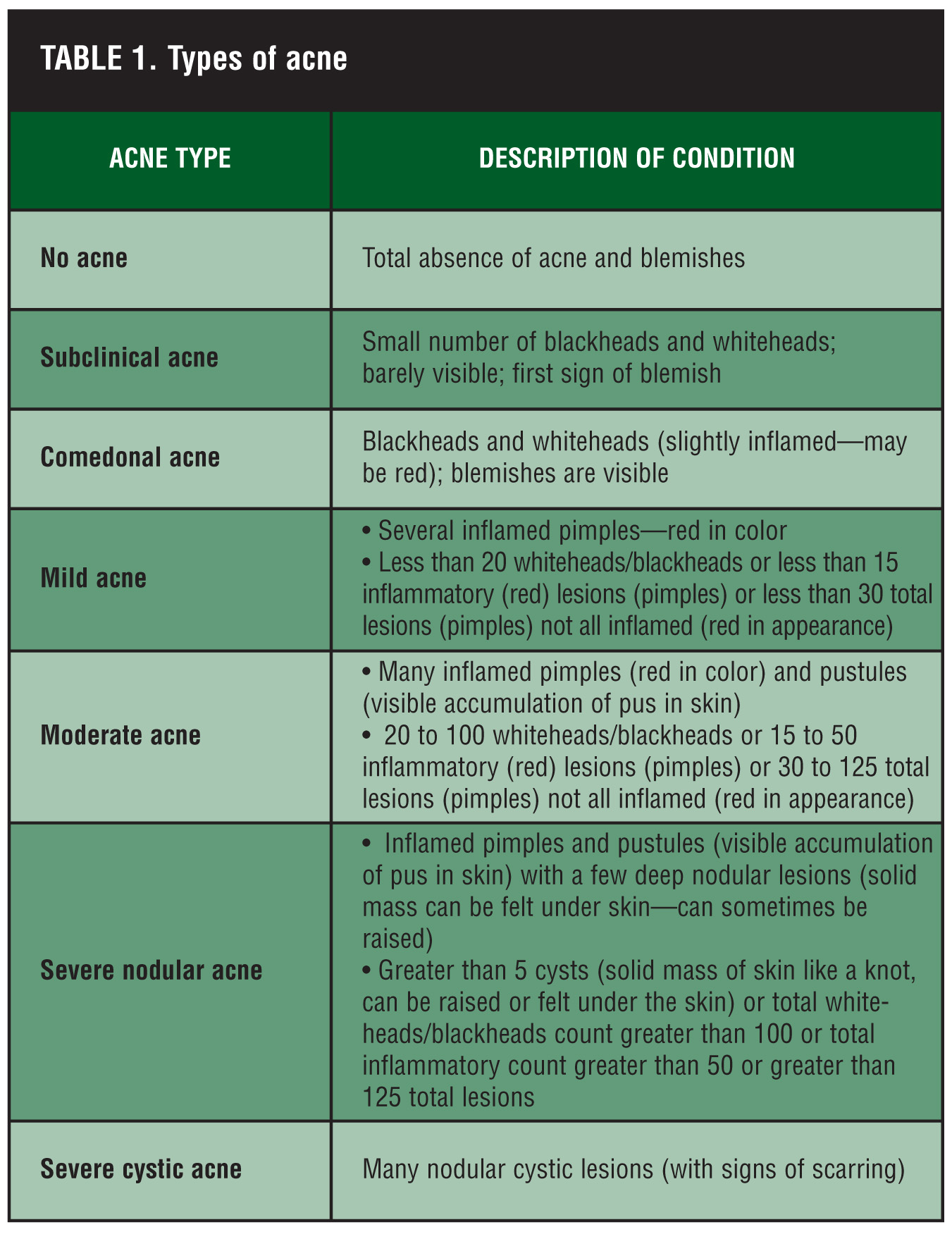
Tända Clear (TC) is a 414nm blue light-emitting diode (LED) treatment that is scientifically and clinically proven to kill the P. acnes bacteria that causes mild-to-moderate acne.[12] This device will help improve existing blemishes as well as prevent future outbreaks. It is indicated in the treatment of mild-to-moderate inflammatory acne. Definitions applied are given in Table 1. The self-assessment chart that provides users with information on their condition is based on an amended Burton[13] acne grading scale.
{kind=link}
Subjects included in the study were instructed by the staff and performed the first treatment under supervision by the clinician, after which self treatment was conducted at home. Affected areas on the face were treated placing the device in contact with the skin. After treatment, the head of the device is easily removed and cleansed.
For the study, TC was applied to the applicable area once daily for six minutes for a period of eight weeks, after which the treatment was completed. The device turns on automatically after the switch is activated, and the unit comes in contact with the skin. Subjects were instructed to wear protective goggles to avoid exposure to the eyes. Treatments were conducted in office during scheduled office visits and at home by the subject throughout the remainder of the study. Specific instructions were given in the instruction sheet provided to the subject. The present study evaluated the performance of self-applied, LED, blue light therapy in the treatment of mild-to-moderate acne on the face, with regard to the following:
• time to improvement and time to resolution of the number of blemishes and lesions on the face;
• quality of skin condition; occurrence and count of the number of new blemishes and lesions;
• ease of product use;
• Patient comfort, wellbeing, and satisfaction during the treatment period; safety of treatment.
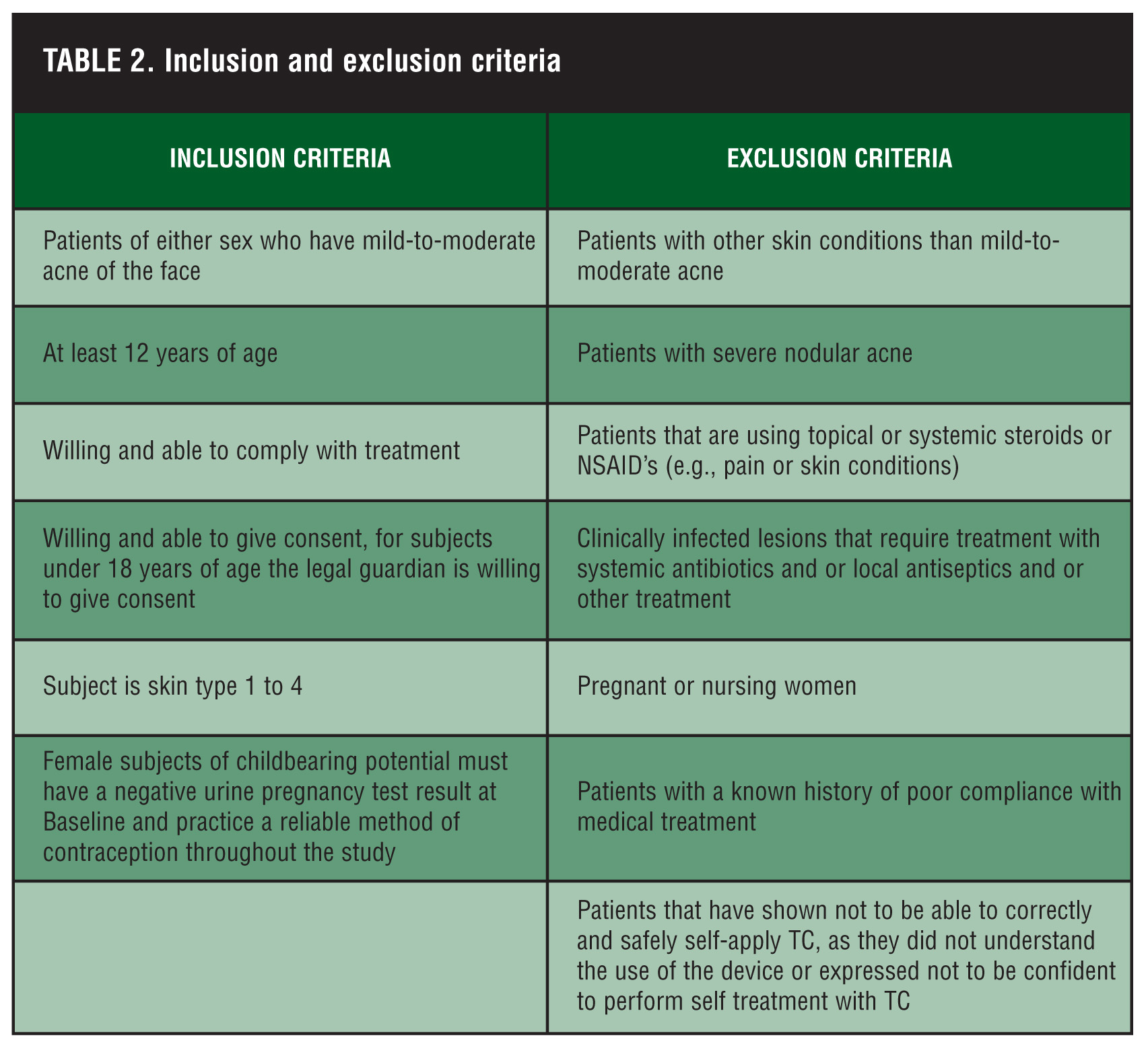
Twenty-one patients with mild-to-moderate acne were included in the study. Patients fulfilled the inclusion criteria prior to recruitment to the evaluation (Table 2).
{kind=link}
Subjects at the Tennessee Clinical Research Center, Nashville, Tennessee (N=21) were included in the study according to the inclusion/ exclusion criteria and after signing the informed consent form under the auspices of an institutional review board. After the subjects agreed to participate in the study, they were supplied with a Tända™ Skincare device. During the eight weeks of therapy, treatment was given to the site of the face where mild and/or moderate acne was present. For observation purposes, the areas on the face were divided as follows: the left and right forehead, the left side of the face, the left chin, the right side of the face, and the right chin. According to the presentation of the subject’s skin condition, the applicable areas of the face were included in the study. A skin-cleansing regime was carried out using Cetaphil® cleanser (Galderma Laboratories, Fort Worth, Texas) before the blue light treatment.
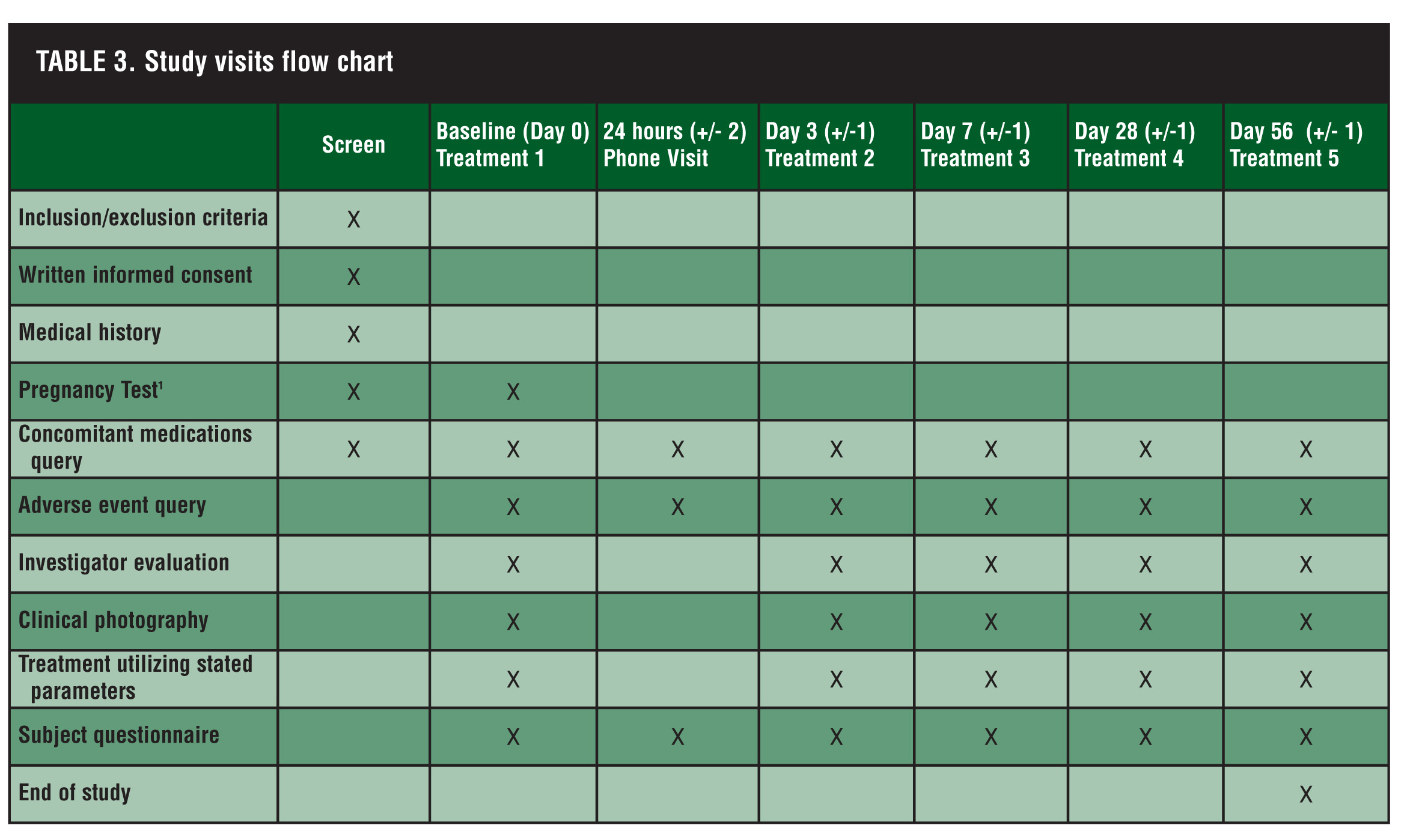
The present clinical evaluation is a prospective, controlled study. Table 3
provides information on the number of visits and activities during these visits. Visual examination and evaluation of skin condition were performed by the clinical investigator and the subject according to the time schedule described in Table 3.
{kind=link}
The effectiveness of TC treatments was measured by the change in the acne-grading scale used from the pretreatment level. Assessments, the filling out of a questionnaire, took place before the start of the Tända Clear treatment at 0 (TX1), at 24 hours (by phone), 72 hours (TX2), and at 1 (TX3), 4 (TX4), and 8 weeks (TX5). If resolution of the blemishes and/or lesions occured before the eight-week study period, the patient returned to the clinic for a final evaluation.
In order to stimulate compliance with the treatment protocol, subjects were informed that details on the use of the blue light were stored in the device’s memory.
Tests were carried out at the five-percent significance level. Data management and analysis was performed independently with SPSS 16.0 statistical software. Where appropriate, ANOVA (repeated measures two- way analyses of variance test), student t-test, and Mann-Whitney test for N=20 were used. Tests were carried out at the 5-percent significance level. The confidence interval was 95 percent.
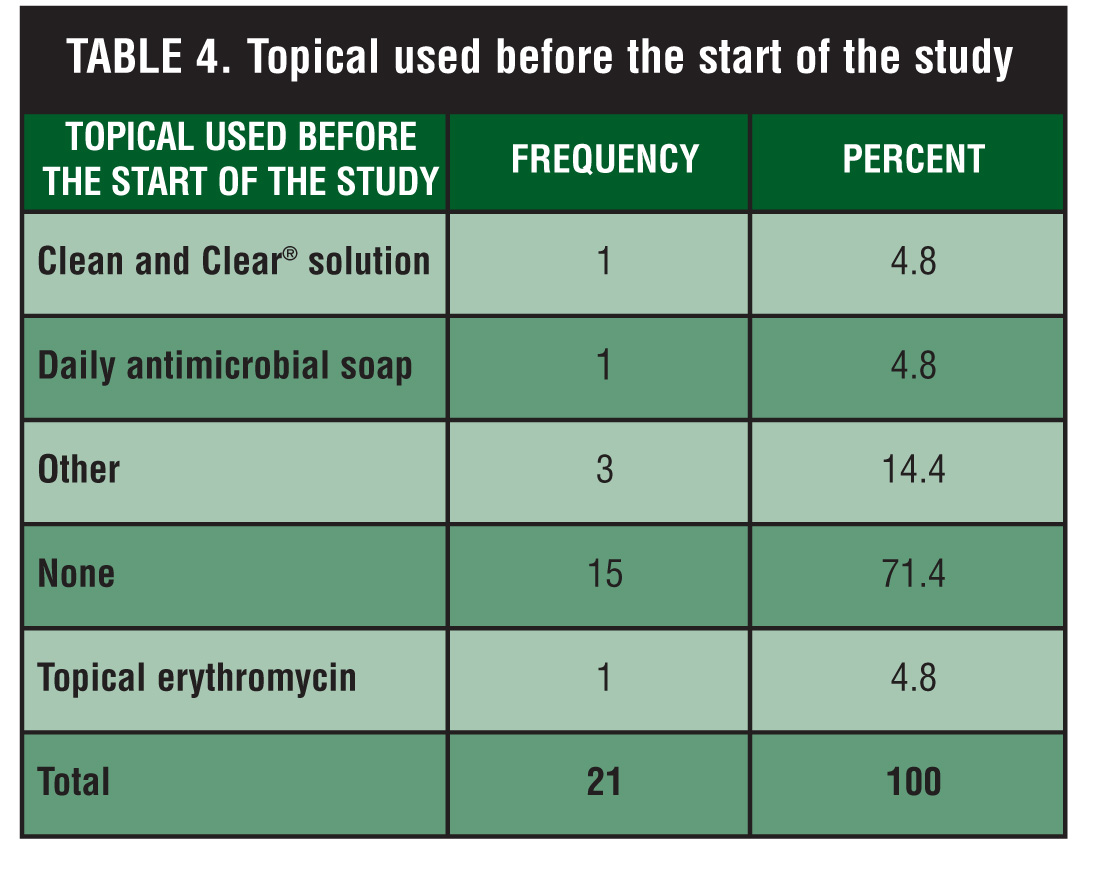
Before the start of the treatment, six subjects used a topical treatment for their acne, and no systemic treatment was used (Table 4). One month prior to and during the study, subjects did not receive treatment to the face with microdermabrasion, glycolic acid, or <20% trichloroacetic acid (TCA) peels. Three months prior to and during the study, subjects did not receive treatments to the face with nonablative laser or other forms of light treatments. Six months prior to and during the study, subjects did not receive treatment to the face with dermabrasion, >20% TCA peel, botulinum toxin, filler injections, cosmetic surgery, isotretinoin, or photodynamic therapy.
{kind=link}
Results
Twenty-one subjects concluded the study (18/21 were female and 3/21 were male with a mean age of 31 years). Subjects expressed confidence in the use of TC for self treatment of acne without the supervision of a doctor and/or clinician. Regarding their previous treatment prior to the start of the study, 33 percent of subjects (n=7) expressed dissatisfaction and 33 percent of subjects (n=7) gave a neutral answer.
When asked whether their expectation of the blue light treatment outcomes would be better for their condition than previous treatment, 76 percent of subjects (n=16) expected to see better results with TC and 23 percent of subjects (n=5) gave a neutral answer.
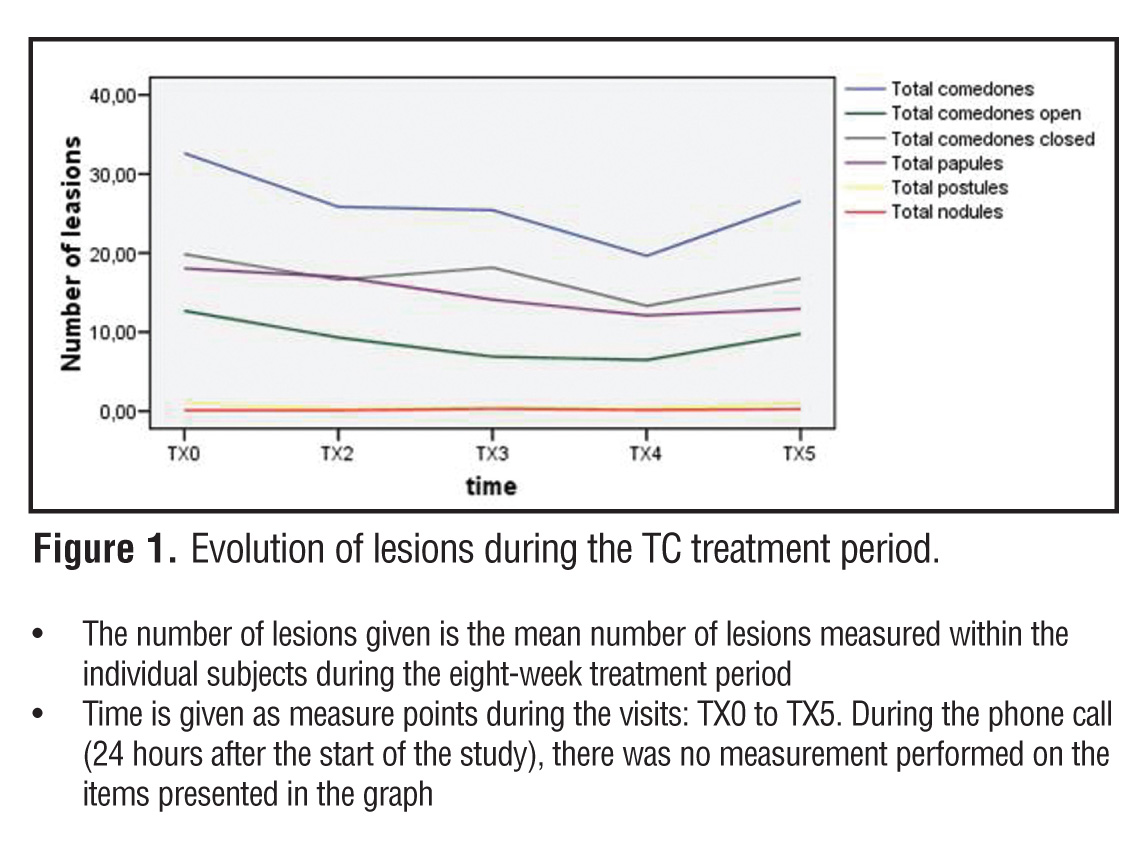
Upon the first outbreak of acne, subjects had a mean age of 15 years (range 8–28 years), and 19 subjects had mild-to-moderate acne for a mean duration of 13.1 years. The study showed that daily self treatment using the device for mild-to-moderate inflammatory acne reduced the number of inflammatory acne lesions significantly.
The total number of papules within subjects during treatment had reduced, and was significant for TX3 with a 21.8-percent reduction (p<0.048), TX4 with a 41.03-percent reduction (p<0.005), and TX5 with a 35.64-percent reduction (p<0.009) .
The total number of pustules measured within subjects during treatment had reduced, but this difference was not statistically significant. Similar results were witnessed for the nodules.
During the study period with blue light treatment, the total number of comedones (blackheads and whiteheads) on the face had significantly reduced. The reduction was statistically significant for the assessment at Day 7 (TX3) with a 22.8-percent reduction (p<0.019) and at Day 28 (TX4) with a 39.1-percent reduction (p<0.001) in total acne lesions. For the assessment at Day 56 (TX5), there was a slight increase noted of these noninflammatory acne lesions.
The total number of open comedones (blackheads) on the face during the treatment period measured within subjects was reduced significantly with a 41.5-percent reduction (p<0.02) for assessment at treatment Day 7 (TX3) and a 50-percent reduction (p< 0.005) for the assessment at Day 28 (TX4).
The total number of closed comedones (whiteheads) on the face during the treatment period measured within subjects was reduced significantly with a 30.4-percent reduction (p< 0.007) for the assessment at Day 28 (TX4) (Figure 1).
{kind=link}
Assessment by the clinician looking at facial skin irritation showed that there was light skin irritation before the start of treatment (mean score was 2 on a 5-point scale—1=strongly disagree; 5=strongly agree) that had slightly improved by the end of the study period. At the start of the study, a light dryness and flakiness was observed, which had significantly improved during the study period.
Signs of inflammation had reduced during the treatment period with TC from 10.6 percent of subjects to 9.5 percent. There were no signs of allergic reactions observed during the study period.
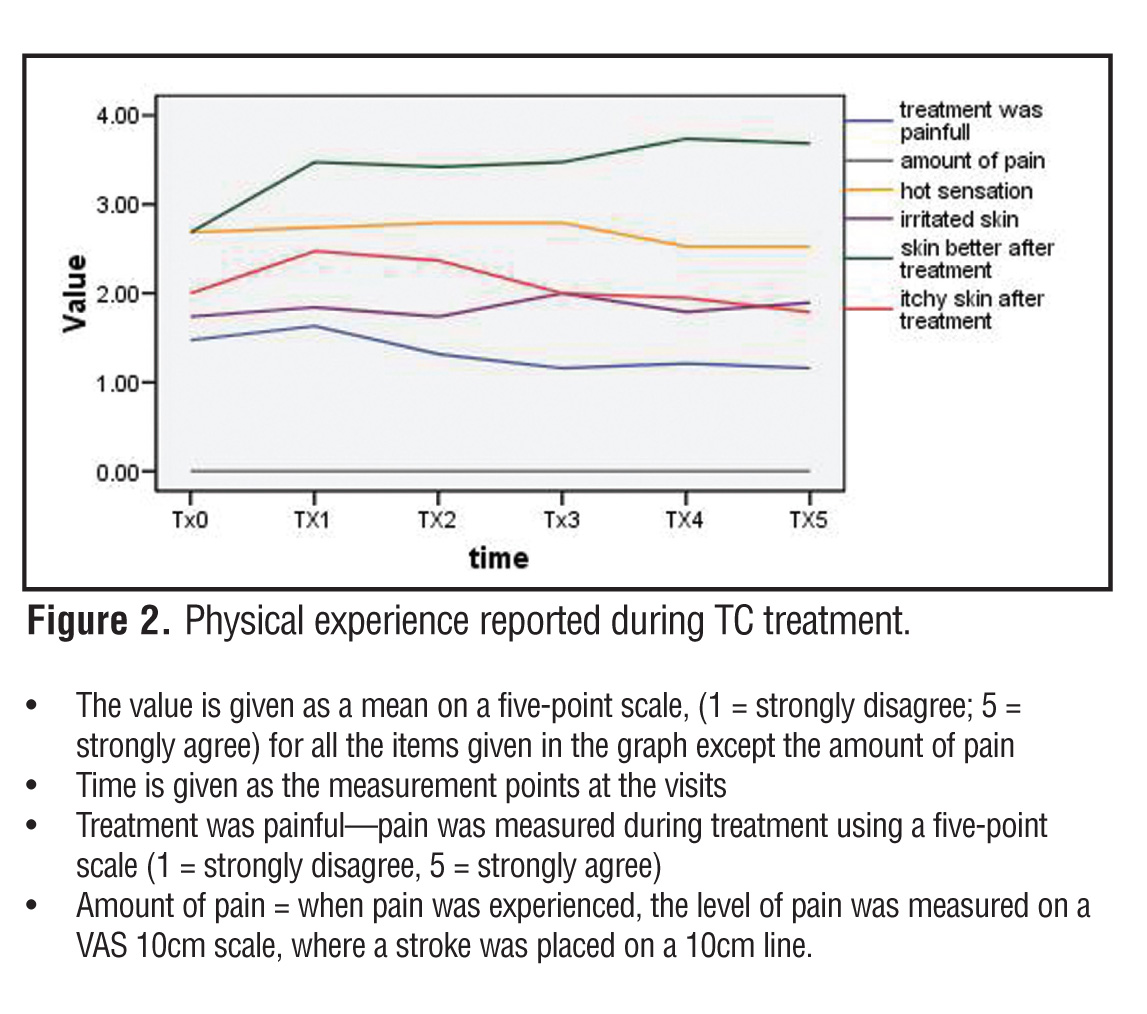
Subjects reported little or no pain or just a slight warm sensation that reduced quickly within minutes after TC therapy treatment. Further, there was little or no irritation reported during the treatment. Most of the subjects expressed the opinion that their skin looked better after the blue light therapy treatment period had been completed (Figure 2).
{kind=link}
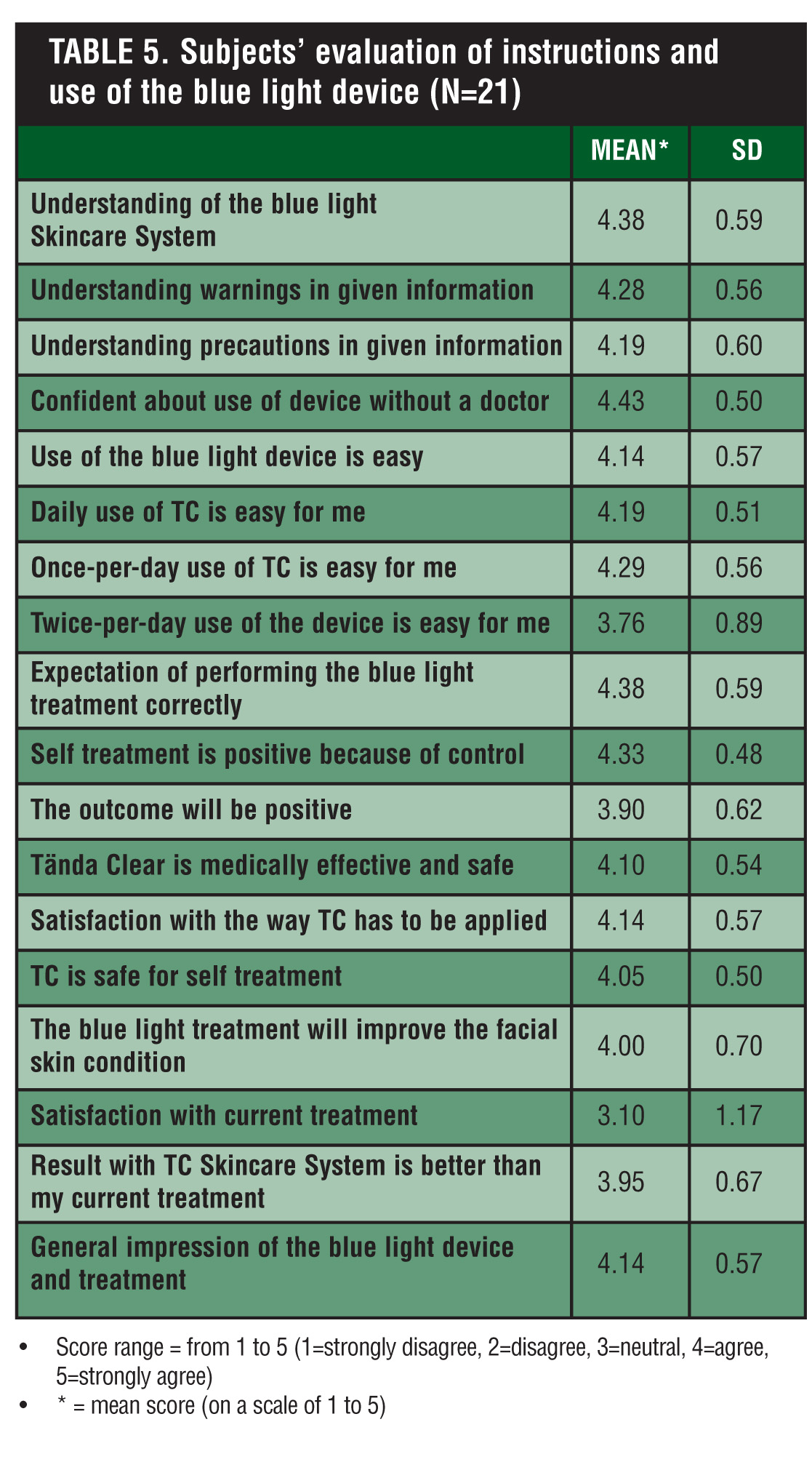
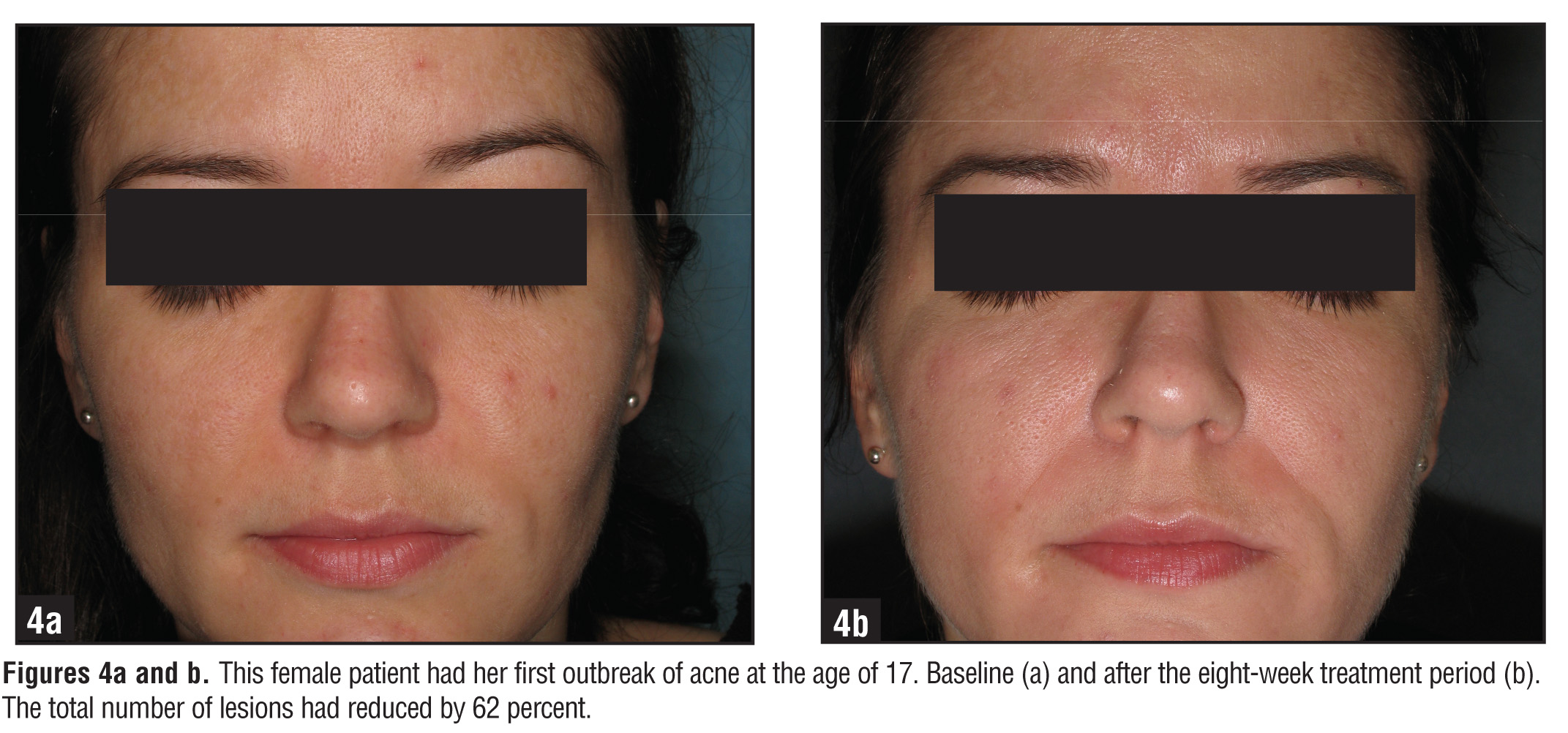
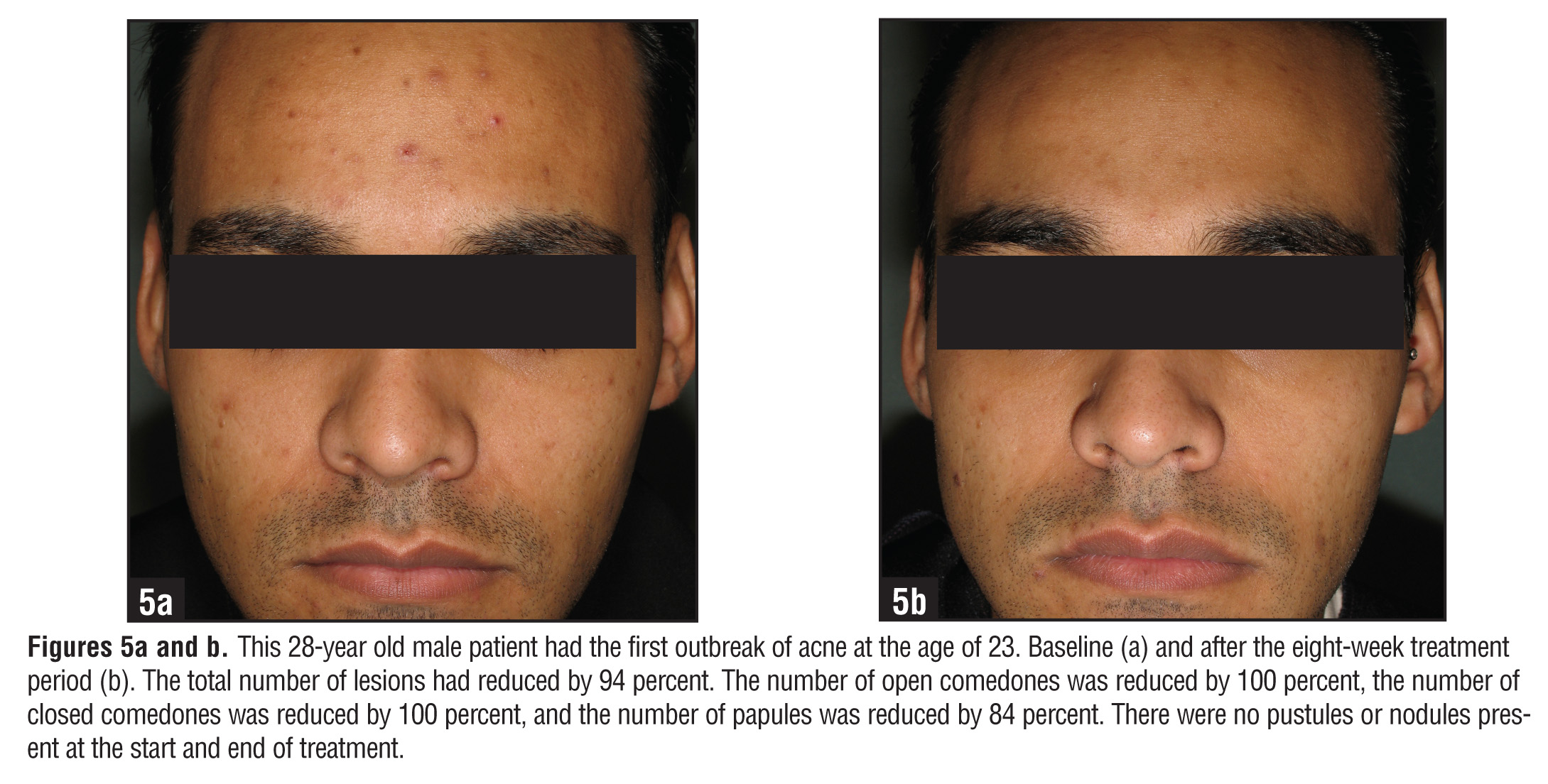
All of the subjects reported that the blue light treatment was easy to perform, they felt confident in administering self treatment once daily (Figure 3), and they thought treatment with the device was safe (Table 5 ). Two typical cases, as shown in Figures 4 and 5, illustrate the results with the Tända Clear system.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
A subject with moderate or severe acne has a well-advanced case of skin inflammation, which is to be addressed with the treatment. Studies have been performed that report on successful treatment of acne using blue light.[14] These studies used various types of LED light sources and had patients visit the clinic for treatment twice weekly.
Self treatment with TC has advantages and may save costs. The present study results obtained are in line with other studies using LED, where treatment was conducted during clinic visits.[10] Twice-weekly application in the clinic with blue light LED has been shown to reduce the number of acne lesions10 and is even more effective when applied daily.
The proposed mode of action of LED application is that a porphyrin (coproporphyrin III) produced within P. acnes generates free radicals when irradiated by 420nm and shorter wavelengths of light.[15] When LED is applied over several days, these free radicals effectively kill the bacteria.[16] Since porphyrins are not otherwise present in skin, and no UV light is employed, LED is shown to be safe. It has been approved by the FDA.[17]
The results of the study showed that the total number of pustules measured within subjects during treatment had decreased; however, this difference was not statistically significant. Similar results were witnessed for the nodules. Some of the subjects had deep-seated pustules that occurred on the bearded area of the face. During the outbreak, they refrained from shaving because of the painful or exudative nature of the lesions. This may explain why there was a reduction in these lesions with the blue light LED treatment; however, the reduction was not large enough to demonstrate a statistically significant difference.
With self treatment using TC for daily applications, optimal treatment is provided, as demonstrated by the study results. Subjects expressed that the instructions given for how to use the device were clear, and that they had positive expectations regarding the effect of the blue light self treatment for their condition. Subjects also expressed that they trusted the device and believed that it was safe (Table 5 ).
Subjects found the use of the blue light device to be easy, even with daily applications. They did not experience any difficulties when using self treatment with TC, even without supervision of a doctor. Motivation of subjects to improve their acne is high, which may explain excellent concordance with the treatment reported during the study.
TC is indicated for the treatment of mild-to-moderate acne. In this study, most of the reduction of signs of acne were achieved for the number of open and closed comedones and papules. It is suggested that the reduction of comedones and papules may support the reduction of early signs of acne and, therefore, may support the prevention of new outbreaks.
Conclusion
Subjects evaluated self administration of the blue light treatment according to the device’s labeling as being safe and effective. The study showed that daily self treatment using the device for mild-to-moderate inflammatory acne reduced the number of acne lesions significantly. Moreover, the study demonstrated a significant improvement of the subjects’ skin conditions. Subjects included in the study were able to safely and effectively administer self treatment with the device and felt confident doing so.
References
1. Cunliffe WJ, et al. Comedogenesis: some new aetiological, clinical, and therapeutic strategies. Br J Dermatol. 2000:142(6):84–91.
2. Coates P, Vyakrnam S, Eady EA, et al. Prevalence of antibiotic-resistant Propionibacteria on the skin of acne patients: 10-year surveillance data and snapshot distribution study. Br J Dermatol. 2002;146(5):840–848.
3. Hanna S, Sharma J, Klotz J. Acne vulgaris: more than skin deep. Dermatology Online Journal. 2003:9(3):8.
4. Cunliffe WJ, Goulden V. Phototherapy and acne vulgaris. Br J Dermatol. 2000;142(5):855–856.
5. Krowchuk DP. Managing acne in adolescents. Pediatric Clinics of North America. 2000;47(4):841–857.
6. James WD. Clinical practice. Acne. N Engl J Med. 2005;352(14):1463–1472.
7. Strauss JS, Krowchuk DP, Leyden JJ, et al. American Academy of Dermatology/American Academy of Dermatology Association. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651–663.
8. Lee WL, Shalita AR, Poh-Fitzpatrick MB. Comparative studies of porphyrin production in Propionibacterium acnes and Propionibacterium granulosum. J Bacteriol. 1978;133(2):811–815.
9. Arakane K, Ryu A, Hayashi C, et al. Singlet oxygen (1 delta g) generation from coproporphyrin in Propionibacterium acnes on irradiation. Biochem Biophys Res Commun. 1996;223(3):578–582.
10. Kawada A, Aragane Y, Kameyama H, et al. Acne phototherapy with a high intensity, enhanced, narrowband, blue light source: an open study and in-vitro investigation. J Dermatol Sci. 2002;30 (2):129–135.
11. Griffin JP. A review of the literature on benign intracranial hypertension associated with medication. Adverse Drug React Toxicol Rev. 1992;11(1):41–57.
12. Sigurdsson V, Knulst AC, van Weelden H. Phototherapy of acne vulgaris with visible light correlates with localized protoporphyrin IX fluorescence. Am J Pathol. 1990;136: 891–897.
13. Burton JL, Cunlitfe WJ, Stafford, et al. The prevalence of acne vulgaris in adolescence. Br J Dermatol. 1971;85:119–126.
14. Morton CA, Scholefield RD, Whitehurst C, Birch J. An open study to determine the efficacy of blue light in the treatment of mild-to-moderate acne. J Dermatolog Treat. 2005;16:219–223.
15. Kjeldstad B. Photoinactivation of Propionibacterium acnes by near-ultraviolet light. Z Naturforsch [C]. 1984;39(3-4):300–302.
16. Ashkenazi H, Malik Z, Harth Y, Nitzan Y. Eradication of Propionibacterium acnes by its endogenic porphyrins after illumination with high intensity blue light. FEMS Immunol Med Microbiol. 2003;35(1):17–24.
17. New Light Therapy for Acne. US Food and Drug Administration. FDA Consumer Magazine. November– December 2002 Notice.