Morgan McCarty, DO; James Q. Del Rosso, DO, FAOCD
Dr. McCarty is Dermatology Resident, St. Joseph Mercy Hospital, Ann Arbor, Michigan. Dr. Del Rosso is Dermatology Residency Director, Valley Hospital Medical Center, Las Vegas, Nevada. Disclosure: Dr. McCarty reports no relevant conflicts of interest. Dr. Del Rosso serves as a consultant, researcher, and/or speaker for Allergan, Coria/Valeant, Galderma, Graceway, Intendis/Bayer, LeoPharma, Medicis, Onset Dermatologics, Ortho Dermatology, Pharmaderm, Promius, Ranbaxy, TriaBeauty, Unilever, and Warner-Chilcott.
The treatment of acne vulgaris (AV) is a constantly evolving subject in dermatology as new data emerges. Conventional therapies, including use of oral antibiotic agents, must be updated regularly due to concerns regarding changes in antibiotic resistance patterns, optimal use in combination with other acne therapies, applicability for patients recalcitrant to other AV treatments, and new information regarding side effects or drug interactions. The availability of efficacious alternative oral antibiotics for AV, such as trimethoprim-sulfamethoxazole (TMP-SMZ), are important for the clinician, allowing for strategic application in specific cases. This article serves as a concise guide for TMP-SMZ use for AV, including a review of possible adverse side effects.
What information is available on the use of oral trimethoprim-
sulfamethoxazole in the treatment of acne vulgaris?
TMP-SMZ is approved by the United States Food and Drug Administration (FDA) for oral treatment of urinary tract infections (UTI), shigellosis, acute otitis media in children, travelers’ diarrhea in adults, acute exacerbations of chronic bronchitis, and treatment and/or prophylaxis of Pneumocystis jirovecii pneumonia (PJP) in the immunocompromised patient.[1,2] Off-label use of TMP-SMZ for AV was first demonstrated in 1971, with a few other reports examining efficacy and safety of TMP-SMZ or TMP alone for AV.[2–5] Studies evaluating oral TMP alone have found it to be effective against inflammatory acne.[2,4,5] TMP-SMZ has been shown to reduce colony counts of Propionibacterium acnes by approximately a 1-log reduction.[6]
Importantly, as with other oral antibiotics used to treat AV, TMP-SMZ is used for treatment of moderate-to-severe inflammatory AV in combination with a topical regimen. A retrospective review examining 22 patients with infantile acne treated for more than 24 months with either erythromycin 250 to 375mg twice daily or TMP 100mg twice daily identified no systemic adverse events. Most infants cleared within 18 months of treatment, while more refractory cases required a duration of 40 months to achieve satisfactory response.[7]
What is the antibacterial mechanism of action of trimethoprim-sulfamethoxazole?
As many bacteria are not capable of incorporating exogenous folate, they are dependent on their own ability to synthesize folate that is needed for their own protein and deoxyribonucleic acid (DNA) production. TMP-SMZ inhibits folate production in bacteria by blocking bacterial dihydrofolic acid reductase, which causes reduced production of purines and subsequently DNA.[4] Studies evaluating oral TMP alone have found it to be effective against inflammatory acne.[2,4,5] TMP is 50,000-fold less effective at suppressing dihydrofolic acid reductase activity as compared to when TMP is combined with the sulfonamide SMZ. The TMP-SMZ combination is bactericidal while TMP alone is bacteriostatic.4,5 As noted above, colony counts of P. acnes are reduced by approximately a 1-log reduction with TMP-SMZ.[6]
As oral antibiotic therapy is used to treat many patients with acne vulgaris that are under 18 years of age, what data are available on chronic administration of trimethoprim-sulfamethoxazole in the pediatric population?
As AV is a chronic disorder necessitating long-term therapy, evaluation of the chronic use of TMP-SMZ in younger patient populations with disease states other than AV may serve to shed some light regarding potential safety concerns. In the first study evaluating use of TMP-SMZ for AV, the treatment length was three months.[3] As mentioned above, the study evaluating long-term use of TMP-SMZ included subjects with infantile acne only.[7]
Other reports have evaluated the use of TMP-SMZ (TMP 2mg/kg and SMZ 10mg/kg) for up to 12 months in children with recurrent UTIs with demonstration of an acceptable adverse-reaction profile.[3,8] Specific reactions noted with long-term use of TMP-SMZ in children with chronic UTI were not described in detail by Craig et al[8]; however, none were documented as life threatening. According to the literature, it is considered appropriate to treat pediatric patients long term with TMP-SMZ for chronic UTIs as no major safety signals have been noted.[8–10]
In 2006 World Health Organization (WHO) guidelines, the United States Public Health Services, and the Infectious Disease Society of America all deemed it advisable to use TMP-SMZ for PJP prophylaxis in pregnancy, in the breastfeeding patient with human immunodeficiency virus (HIV), and in infants at 4 to 6 weeks of age born to mothers with HIV. TMP-SMZ prophylaxis may be initiated after the first trimester or throughout pregnancy along with folic acid supplementation, as the mortality rate for pregnant HIV patients with PJP in the United States is 50 percent, and PJP is the major cause of death in pregnant females with acquired immune deficiency syndrome (AIDS).[11] The use of TMP-SMZ outweighs potential adverse events and sequelae in this population who are known to exhibit a higher risk of TMP-SMZ-associated side effects, including severe cutaneous reactions.[2,11]
Based on publications supporting the chronic use of TMP-SMZ for disorders other than AV, it appears rational that TMP-SMZ be utilized in selected cases of AV refractory to conventional treatment, including oral antibiotics that are commonly used to treat AV (e.g., tetracyclines). Use of TMP-SMZ for durations longer than what is used for treatment of acute bacterial infections, such as more chronic use over several months, appears to be safe overall. However, the well-known potential for TMP-SMZ to cause rare but severe adverse events, especially severe cutaneous reactions, hematological changes, and hyperkalemia, must always be kept in mind when considering use of TMP-SMZ for adults, adolescents, or children with AV.[2,12] Additionally, recommendations on how to determine adequate duration of oral antibiotic treatment for AV in the individual patient are reviewed elsewhere.[12]
When trimethoprim-sulfamethoxazole is used for treatment of acne vulgaris, are there recommendations that it be used in combination with other acne therapies?
Importantly, it is not recommended that oral or topical antibiotics be used as monotherapy for AV due to progressive emergence of P. acnes strains that are less sensitive to antibiotics (“antibiotic-resistant” P. acnes).[5,12–14] As prolonged antibiotic administration is associated with an upward climb in the minimum inhibitory concentration (MICs) against bacteria, it is prudent to reserve TMP-SMZ for selected refractory cases of AV to prevent emergence of less sensitive bacterial strains, including with P. acnes.[1] Regarding MICs against P. acnes and antibiotic use for AV, it is strongly suggested that antibiotic therapy for AV be used concurrently with benzoyl peroxide (BP), the latter demonstrating both potent in-vitro reduction in P. acnes and the ability to decrease the emergence of antibiotic-resistant P. acnes strains.[5,12–14] It is important to note that this effect of BP has not been well studied in AV patients treated specifically with concurrent use of TMP-SMZ and BP.[12,13]
What are potential consequences of exposing patients with acne vulgaris to systemic antibiotic effects that target more than just Propionibacterium acnes?
Antibiotics used to treat AV have effects against bacteria other than P. acnes and, therefore, alter the microbiological profile of the host, at least temporarily. The potential consequences and clinical relevance of these microbiological changes remain a matter of controversy. Additionally, more focus has been placed by government agencies on the importance of modifying antibiotic prescribing patterns in order to reduce the emergence of “antibiotic resistance.”
Margolis et al[14] conducted a retrospective cohort study that examined 118,496 individuals with AV from a large general practice database, 84,977 of whom received a topical antibiotic (erythromycin, clindamycin) and/or oral antibiotic (tetracyclines, erythromycin) for at least six weeks versus 33,519 of whom were not on antibiotic therapy for AV. The data were mined using diagnosis and prescription codes to evaluate whether or not any of these subjects developed an upper respiratory tract infection (URTI) or UTI (control group) over a 12-month period. The results revealed that patients with AV treated with oral and/or topical antibiotics for at least six weeks demonstrated a twofold greater risk for development of a URTI, but not a UTI.
Increased provider seeking behavior was accounted for by examining patients with hypertension who are also routinely seen by a physician. When the two groups were compared, hypertensive patients with URTI versus AV patients with URTI, the antibiotic-treated AV patients were two times as likely to be coded for URTI than the untreated AV patients and the hypertension patients (P<0.001).[15] However, there are several limitations to this study, including retrospective design, use of diagnosis coding to identify diagnosis without direct patient examination by the investigators, variable dose response and URTI occurrence, and lack of determination if the study groups had similar URTI case rates before antibiotic treatment.[16]
A proposed mechanism for the possible correlation between the rate of URTIs and antibiotic use for AV relates to nonantimicrobial and direct anti-inflammatory properties of some antibiotics. For example, tetracycline has the ability to impede neutrophil migration, perhaps allowing for propensity for infection.[16] The research on URTI and antibiotic use may seem trivial initially; however, more than 200 million office visits for URTI (pharyngitis, coryza, rhinitis, and mild temperature) were coded in the United States in 2002 and accounted for a cost of $25 billion in revenue.[15]
Given the economic implications of management of URTIs, Bowe et al[16] assessed the possibility of increasing URTI in household members in contact with AV patients treated with antibiotics. There was no significant association in nearly 100,000 contacts between 15 to 65 years of age.[17] This one study does not definitively prove the presence or lack of causation; however, the patient may wish to be educated regarding the data available. TMP-SMZ use for AV was not directly included in the studies evaluating the possible correlation of antibiotic use in AV and the increased predisposition for URTI. Therefore, it may be premature to assume TMP-SMZ would be associated with the same relative risk that was found with other antibiotic classes based on the retrospective study by Margolis et al.[14] More research is needed in this area before concluding that there is a true causal relationship between antibiotic use in AV and an increased risk for development of URTIs.
What patterns of Propionibacterium acnes antibiotic resistance have been identified with trimethoprim-sulfamethoxazole or trimethoprim as compared to other oral antibiotics used to treat acne vulgaris?
Unfortunately, there is conspicuous absence of recent published data on P. acnes antibiotic-resistance patterns with oral antibiotics used to treat acne vulgaris in the United States. In 1997, Ross et al[17] examined P. acnes antibiotic resistance in Europe, the United States, Japan, and Australia and found that P. acnes isolates from all evaluated countries showed either erythromycin-, clindamycin-, and/or tetracycline-resistance patterns, with P. acnes resistance to minocycline found only in the United States.[18] In the United Kingdom between 1991 and 1999, resistant strains peaked in frequency and treatment practices were altered to switch patients who showed resistance to conventional antibiotics to treatment with oral trimethoprim. Soon thereafter, P. acnes resistance patterns to conventional antibiotics used to treat AV started on a downward trend. Ross et al[17] also observed trimethoprim was active against most erythromycin- and tetracycline-resistant P. acnes strains. It has also been documented that antibiotic-resistant P. acnes is transmitted to AV patients within families, between patients, and through provider contact.[17]
TMP-SMZ is used to treat a wide spectrum of cutaneous infections caused by a variety of pathogens. Therefore, when considering its use for treatment of AV, concern arises with widespread use and prolonged use of TMP-SMZ for a common disorder such as AV will increase the emergence of not only resistant P. acnes strains, but also other TMP-SMZ-resistant bacterial organisms, including pathogens. This is especially of concern in immunocompromised patients. TMP-SMZ is the preferred treatment and prophylactic agent for PJP and is also used to treat methicillin-resistant Staphylococcus aureus (MRSA) infections, especially the community-acquired type (CA-MRSA), and Wegener granulomatosis.[1,11]
In what cases of acne vulgaris might consideration be given to using trimethoprim-sulfamethoxazole?
Tetracycline agents, especially doxycycline and minocycline, are the most common oral antibiotics used by dermatologists in the United States for the treatment of AV.[12,18] When these agents are not considered effective or when adverse reactions occur that result in the need for discontinuation, alternative oral antibiotics have been suggested. These include macrolide agents and TMP-SMZ.[2,5,12] It has been noted that TMP-SMZ is effective in some refractory cases of AV.[2,12] Long-term use is sometimes necessitated as some patients flare when TMP-SMZ is stopped despite use of a topical regimen. In addition, cases of refractory AV, which are actually a result of gram-negative acne/folliculitis, may respond to TMP-SMZ due to its spectrum of antibiotic coverage.
Tan[5] recommends initially using TMP-SMZ 160/800mg twice daily with a later switch to once daily for more prolonged maintenance therapy. Some practitioners use a step-down dosing technique to theoretically prevent recurrent flares of inflammatory lesions; however, there is no definitive evidence supporting a step-down approach. The preferred method utilized by the authors is cessation of oral antibiotic treatment without step down when the number of new active lesions is few to none and persistent erythema or hyperpigmentation has diminished.[12]
What cutaneous adverse events have been associated with the use of trimethoprim-sulfamethoxazole?
TMP-SMZ has been associated with a wide variety of adverse reactions (ARs); however, the more serious cutaneous ARs are at the forefront of concern when prescribing TMP-SMZ. Perhaps the saving grace with use of TMP-SMZ is that many of the associated major cutaneous ARs occur early, that is within the first 2 to 3 months of starting therapy.[2,18] This allows the clinician to feel some sense of comfort when a patient is given TMP-SMZ and he or she does not develop a serious cutaneous AR early during the course of therapy for AV or other disorders. However, the clinician must still remain vigilant as rare exceptions may exist, and other ARs, such as hematological reactions, may take longer to emerge.
The most common cutaneous reaction to TMP-SMZ is a macular or morbilliform pattern and occurs in up to five percent of the general population and 15 percent in HIV patients.[2,18] TMP-SMZ has also been associated with other cutaneous ARs, such as urticaria, fixed drug eruption, exfoliative dermatitis, erythema multiforme including Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug-induced acute febrile neutrophilic dermatosis (Sweet’s syndrome).[2,19–21] Reaction patterns of some cutaneous ARs that can occur with TMP-SMZ are depicted in Table 1.
{kind=link}
Cutaneous reactions without systemic features. Fixed drug eruption due to TMP-SMZ tends to exhibit the quickest onset among the cutaneous reactions associated with TMP-SMZ, usually appearing between 1 to 8 hours of ingestion, but sometimes within a few days.[2] TMP-SMZ-associated Sweet’s syndrome occurs an average of 7.5 days after initiation of therapy.[19,20]
Cutaneous reactions with systemic features. Drug-induced hypersensitivity syndrome (DIHS), also referred to as drug rash with eosinophilia and systemic symptoms (DRESS), is a more severe reaction process that is associated with systemic symptoms and internal organ involvement.[2,21] DIHS occurs most commonly within two weeks to two months after starting TMP-SMZ, most often presenting with fever, fatigue, a generalized exanthem, and systemic involvement of one or more organ systems. The most feared cutaneous reaction patterns that have been associated with the use of TMP-SMZ, due to associated morbidity and the risk of mortality, are TEN and SJS and the observation that approximately 30 percent of TEN cases are related to sulfonamide ingestion.[1,2,19,21,22] TEN and SJS usually manifest within the first 1 to 3 months of TMP-SMZ therapy. Clinical features suggestive of TEN and SJS are outlined in Table 1.[12,18,21] Rarely, cases of aseptic meningitis and fulminant hepatic necrosis have been reported in the literature in association with TMP-SMZ use.[1,22]
Overall, if a cutaneous reaction to TMP-SMZ is suspected, discontinuation of TMP-SMZ is very important, along with appropriate intervention with other therapies based on the type and severity of reaction. Development of autoimmune thyroiditis has been reported in some cases of DIHS. Initially, hyperthyroidism can develop in DIHS, followed by hypothyroidism and positive antimicrosomal antibodies months later.[21]
What explanations have been given regarding the mechanism of drug hypersensitivity syndrome induced by trimethoprim-sulfamethoxazole?
It is estimated that between 1 in 1,000 and 1 in 10,000 drug cases of DIHS hypersensitivity are related to use of sulfonamides and anticonvulsants, respectively. However, the exact number is unknown due to variable reporting. The aromatic amine structural components, which are oxidized to hydroxylamines and then to nitroso derivatives, cycle bidirectionally, creating a stressful oxidative state.[25,26]
Procainamide and dapsone exhibit a similar chemical oxidative cycle to TMP-SMZ, allowing for accumulation of oxidative stress and reactive protein production. This mechanism theoretically explains the potential for increased toxicity of dapsone or procainamide when used in conjunction with TMP-SMZ.[24,25]
What other adverse reactions have been related to the use of trimethoprim-sulamethoxazole? Are some of these reactions correlated with interactions with other drugs?
Hypoglycemia. Hypoglycemia may occur in patients with diabetes mellitus, especially as the sulfonamide component increases the activity of some antidiabetic agents (sulfonylureas).[23–24]
Hyponatremia. TMP alone may increase the risk of hyponatremia when used in combination with diuretics.[25]
Oral contraceptive failure potential. As with oral antibiotics other than rifamycins, reports of oral contraceptive failure due to concurrent use of TMP-SMZ are controversial. Therefore, especially with long-term co-administration for AV patients, TMP-SMZ is best categorized along with other oral antibiotics, wherein appropriate precaution is prudent, despite the negligible or absent likelihood of a drug interaction.
Hematologic reactions. TMP-SMZ has been associated with a variety of hematological reactions (blood dyscrasias).[2,29–32] Swedish population study data reported the occurrence of blood dyscrasias from TMP-SMZ to be 1 in 18,000.[30]
Agranulocytosis was reported to be 0.6 to 1.3 per million. Long-term use studies spanning three months found few instances of adverse hemotological effects.[30,31] It has been noted that patients susceptible to blood abnormalities due to underlying medical conditions, such as alcoholics, patients with malabsorption or malnourishment disorders, and pregnant women, are predisposed to developing cytopenias.[29,32] Interestingly, these same underlying disorders predispose patients to deficiency in folate. Monitoring for blood dyscrasias and megaloblastosis, and/or pre-emptive folic acid co-administration (up to 5mg/day) to avoid hematological side effects is prudent. A complete blood cell count performed every three months is suggested to monitor for folate deficiency in individuals with a known or medical predisposition.[2,19]
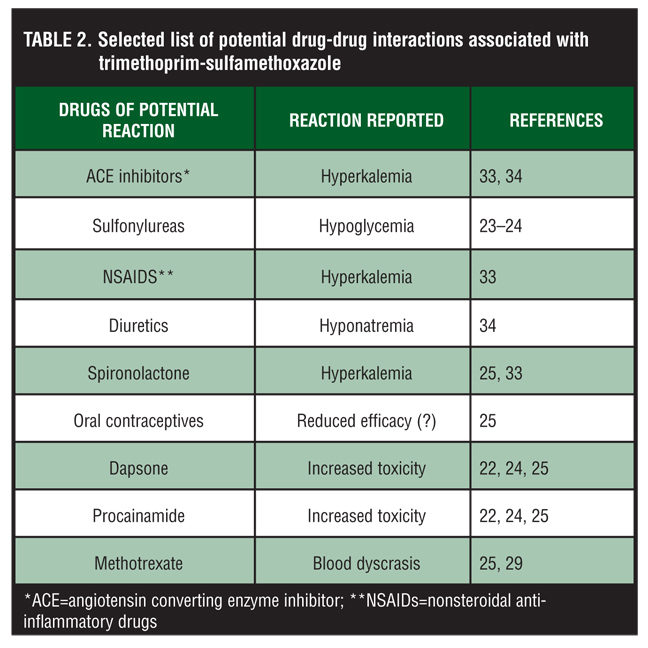
Concurrent use of TMP-SMZ in patients on methotrexate is not recommended due to increased antifolate activity and possible hematological reactions.[2,4,25] Few reports exist that support any significant interaction of TMP-SMZ with warfarin, with dosage adjustments likely to be unnecessary.[25] Table 2 provides a selected list of potential drug interactions associated with use of TMP-SMZ .
{kind=link}
Hyperkalemia. The potential for hyperkalemia has been associated with TMP-SMZ, which prevents loss of potassium by blocking amiloride-sensitive sodium channels in distal nephrons. Several studies have examined increased risk of hyperkalemia with concurrent use of angiotensin converting enzyme (ACE) inhbitors, angiotension II receptor blockers (ARBs), nonsteroidal anti-inflammatory drugs (NSAIDs), spironolactone, and prednisolone.[25,32–36] Cases of severe hyperkalemia were first reported in the 1990s in HIV patients, but also in the elderly, and even in patients with normal renal function and with standard dosages of TMP-SMZ.[25,36,37] The potential for clinically significant hyperkalemia has become more recognized with caution suggested in patients on potassium-sparing agents.[25] The cohort study by Loughlin et al[36] examined patients ages 10 to 59 years and suggested that there appeared to be no greater risk of hyperkalemic events in patients taking drospirenone-containing oral contraceptives (OCs) versus other OCs. Dinger et al[37] examined 58,674 drospirenone-containing OC users in which 99 developed new onset arrhythmias (e.g., Wolff-Parkinson-White syndrome, hyperthyroidism with tachycardia, ventricular and supraventricular extrasystoles, tachycardia absoluta, sick sinus syndrome). No new cases of arrhythmia were found to be related to the potassium-sparing property of drospirenone. The same conclusions were drawn regarding hyperkalemia potentially causing arrhythmia in several other studies.[37,38] However, a limitation of these studies is that they did not address concurrent use of drugs that precipitate hyporeninemia or hypoaldostronism, such as NSAIDs, TMP-SMZ, and spironolactone.[25,34–36] There is plausible existence for development of hyperkalemia especially if there is underlying renal insufficiency, diabetes, or concurrent use of potassium-sparing agents.[39] A study by McAdams et al[39] regarding drospirenone-induced hyperkalemia reported that 17.6 percent of 62,527 women taking a drospirenone-containing product were also taking other potassium-sparing drugs, such as certain diuretics (i.e., amiloride), ACE inhibitors, ARBs, and NSAIDs. From the standpoint of identifying the population subset at higher risk of hyperkalemia, 40 percent of subjects 35 years of age or older were also taking multiple potassium-sparing drugs. McAdams et al[39] stressed the importance of screening patients on OCs containing drospirenone about the use of potential drug therapy combinations that may induce hyperkalemia.[39]
What are the important considerations related to use of trimethoprim-sulfamethoxazole in pregnancy?
TMP is catergory C while sulfonamides are category B in pregnancy, resulting in TMP-SMZ being placed as category C classification.[40] The incidence of kernicterus and the possible teratogenic potential of TMP-SMZ have recently been disputed. The mechanism for hyperbilirubinemia is theorized to be TMP-SMZ binding to albumin and leading to displacement of albumin-bound bilirubin into circulation as free bilirubin.[11,41] Forna et al[11] reviewed the data for the incidence of TMP-SMZ causing kernicterus. Most of the research on this topic is derived from small retrospective studies that examined the entire class of sulfonamides. In several reports, outcome assessment was not differentiated based on whether or not the infant had glucose-6-phosphate dehydrogenase (G6PD) deficiency.[11] In 1956, Silverman et al[42] found evidence of TMP-SMZ causing hyperbilirubinemia, an increased risk of kernicterus, and risk of mortality in postnatal low-birth-weight neonates, a subset associated with greater risk for kernicterus regardless of sulfisoxazole exposure.[42] Forna et al[11] examined all data regarding TMP-SMZ use in pregnancy and breastfeeding and found little substantial evidence that kernicterus is a common sequelae of TMP-SMZ exposure in pregnancy. The identification of insufficient evidence regarding a high potential for kernicterus development with TMP-SMZ use in pregnancy challenged the “recycled dogma” that emphasized this complication and implied that both the risk and its consistency for development were both minimal. As a result, the WHO elected to include TMP-SMZ in the guidelines for PJP prophylaxis in HIV-positive pregnancies after the first trimester and HIV-positive women who were breastfeeding.[11] Due to minimal accumulation in breast milk if an infant is full term, and with no evidence of G6PD deficiency nor hyperbilirubinemia, the American Academy of Pediatrics deems breastfeeding with use of TMP-SMZ acceptable.[40,41] However, this classification for use of TMP-SMZ does not necessarily address or support chronic use of TMP-SMZ, especially for an indication such as AV, as the majority of TMP-SMZ use is for short-term treatment of a systemic infection. The authors suggest avoidance of TMP-SMZ in women who are breastfeeding until more definitive evidence in this specific population is specifically evaluated.
Although available data do not substantiate cleft palate and cardiac malformations associated with TMP-SMZ use in pregnancy, the antifolate potential of TMP-SMZ is considered a theoretical risk for development of these birth defects. Folate supplementation or avoidance of TMP-SMZ use as prophylaxis in the first trimester of pregnancy is deemed reasonable when the benefits of TMP-SMZ use outweigh the risks.[11] However, the authors are not condoning the intentional use of TMP-SMZ for treatment of AV during pregnancy or breastfeeding. Nevertheless, it is advantageous for clinicians to understand the available data if an unintended pregnancy occurs in a female patient who is taking TMP-SMZ for AV. The evidence is indeed scant with regard to direct causation of kernictuis in infants unless the infant is G6PD deficient. However, the teratogenic potential of TMP-SMZ in the first trimester is still considered plausible, though deemed to be low risk.[11,41]
What is known about the risk of allergic reactions to trimethoprim-
sulfamethoxazole, especially as it contains a sulfonamide antibiotic agent?
When considering the allergic hypersensitivity potential of a sulfonamide, or of a combination formulation that contains a sulfonamide agent, it is essential to recognize the two distinct groups of sulfonamide agents: antimicrobial and nonantimicrobial. The antimicrobial drug class structurally contains an arylamine group, which has been correlated with a greater risk of hypersensitivity reactions. Sulfonamides in the nonantimicrobial class do not contain an arylamine moiety. The supporting evidence derived from retrospective cohort studies suggests overall that there is a very low, but not definitively impossible risk, of hypersensitivity reactions in the absence of this structural moiety.[42] One notable exception is the sulfonamide agent, sulfasalazine. Although sulfasalazine has been categorized as a nonantimicrobial sulfonamide, its chemical structure contains similarity to the arylamine group, and reports of severe hypersensitivity reactions associated with sulfasalazine have been published.[43] There is little evidence that some other nonantimicrobial agents that structurally contain a sulfonamide component, such as some diuretics (i.e., furosemide) and sulfonylurea hypoglycemic agents, cross react with the sulfonamide antimicrobial class.
The most common clinical manifestations of hypersensitivity reactions to antimicrobial sulfonamides and their cross-reactive “cousins,” including TMP-SMZ, which contains the antimicrobial sulfonamide sulfamethoxazole, are skin eruption (usually exanthem-like), nausea, vomiting, diarrhea, and photosensitivity.[1,4] As discussed above, severe reactions, such as SJS and TEN, are rare among the general population considering the overall volume of TMP-SMZ use.[2,8] However, the severe nature of SJS and TEN, and their association with high morbidity and mortality risk, demands strong consideration when deciding the use of TMP-SMZ in individual patients, especially for disorders such as AV[.2] In adults, TEN associ[ated with TMP-SMZ use has been estimated to occur in 2.6 per 100,000, and in children the rate has been estimated to be 0.4 to 1 case per million person-years.[2,] Jick et al[44] conducted a 45-day follow-up study in a population of 232,390 people who were prescribed TMP-SMZ, 266,951 who were prescribed trimethoprim alone, and 196,397 who were prescribed cephalexin in the United Kingdom.[44] The overall study also examined adverse drug reactions up to 45 days following drug exposure. The outcomes showed that one patient developed a hematological reaction and four developed erythema multiforme/SJS. None of the patients treated with TMP or TMP-SMZ developed TEN. The study concluded that the overall risk for adverse reactions to TMP-SMZ and TMP are similar to other antibiotics.[44] However, this does not take into account that antimicrobial sulfonamides, including TMP-SMZ, are the most common cause of TEN as compared to other drugs known to cause this specific reaction pattern, possibly due to innate characteristics sulfonamide agents, the TMP-SMZ combination, and/or relative frequency of use.
Another caveat that appears important to address before initiating treatment with TMP-SMZ is to determine whether the patient’s first-degree family members have had DIHS related to use of TMP-SMZ or another sulfonamide agent. Realistically, many patients may not know this information or relate it accurately. However, if there is a confirmed or highly suspected positive family history of DIHS, it is prudent to avoid TMP-SMZ, especially for treatment of AV. Genetically directed inheritance of similar metabolic pathways sets up the background for increased risk of DIHS in a patient with a family history of hypersensitivity to the drug.[2]
What concluding comments can be made about use of trimethoprim-sulfamethoxazole in the treatment of acne vulgaris?
TMP-SMZ might be a reasonable treatment for the refractory AV patient. It appears germane to avoid TMP-SMZ in those patients who have documented allergy directly or a family history of reactions to the drug, G6PD deficiency, or wish to become pregnant. Caution may be appropriate with concomitant use of TMP-SMZ and hyporeninemic hypoaldosteronism-precipitating drugs such as NSAIDs. The art of clinical dermatology is not a dichotomous practice, but a continuum ever ebbing and flowing with nuance.
When faced with a variety of treatment modalities, all aspects of the therapy are examined and custom tailored to the patient’s unique presentation. Hopefully, this article serves to aid clinicians in addressing many of their patient’s questions and supportive evidence for the clinicians’ treatment plan.
References
1. Smilack JD. Trimethoprim-sulfamethoxazole. Mayo Clin Proc. 1999;74(7):730–734.
2. Bhambri S, Del Rosso JQ, Desai A. Oral trimethoprim/sulfamethoxazole in the treatment of acne vulgaris. Cutis. 2007;79(6):430–434.
3. Cotterill JA, Cunliffe WJ, Forster R, et al. A comparison of trimethoprim-sulphamethoxazole with oxytetracycline in acne vulgaris. Br J Dermatol. 1971;84(4):366–369.
4. Katzung B. Basic and Clinical Pharmacology, 10th ed. Toronto, Canada: The McGraw-Hill Companies Inc.; 2007.
5. Tan H. Antibacterial therapy for acne: a guide to selection and use of systemic agents. Am J Clin Dermatol. 2003;4(5):307–314.
6. Del Rosso JQ, Kim G. Optimizing use of oral antibiotics in acne vulgaris. Dermatol Clin. 2009;27(1):33–42.
7. Cunliffe WJ, Baron SE, Coulson IH. A clinical and therapeutic study of 29 patients with infantile acne. Br J Dermatol. 2001;145(3):463–466.
8. Craig J, Simpson J, Williams G, et al. Prevention of Recurrent Urinary Tract Infection in Children with Vesicoureteric Reflux and Normal Renal Tracts (PRIVENT) Investigators. Antibiotic prophylaxis and recurrent urinary tract infection in children. N Engl J Med. 2009;361(18):1748–1759. Erratum in: N Engl J Med. 2010;362(13):1250.
9. Williams GJ, Wei L, Lee A, Craig JC. Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst Rev. 2006;3:CD001534.
10. Karpman E, Kurzrock EA. Adverse reactions of nitrofurantoin, trimethoprim and sulfamethoxazole in children. J Urol. 2004;172(2):448–453.
11. Forna F, McConnell M, Kitabire F, et al. Systematic review of the safety of trimethoprim-sulfamethoxazole for prophylaxis in HIV-infected pregnant women: implications for resource-limited settings. AIDS Rev. 2006;8(1):24–36.
12. Strauss J, Krowchuk D, Leyden J, et al. American Academy of Dermatology/American Academy of Dermatology Association. Guidelines of care for acne vulgaris manage-ment. J Am Acad Dermatol. 2007; 56(4):651–663. Epub 2007 Feb 5.
13. Leyden JJ, Wortzman M, Baldwin EK. Antibiotic-resistant Propionibacterium acnes suppressed by a benzoyl peroxide cleanser 6%. Cutis. 2008;82(6):417–421.
14. Margolis DJ, Bowe WP, Hoffstad O, Berlin JA. Antibiotic treatment of acne may be associated with upper respiratory tract infections. Arch Dermatol. 2005;141(9):1132–1136.
15. Chan AW, Shaw JC. Acne, antibiotics, and upper respiratory tract infections. Arch Dermatol. 2005;141(9):1157–1158.
16. Bowe WP, Hoffstad O, Margolis DJ. Upper respiratory tract infection in household contacts of acne patients. Dermatology. 2007;215(3):213–218.
17. Ross J, Snelling A, Eady E, et al. Phenotypic and genotypic characterization of antibiotic-resistant P. acnes isolated from acne patients attending dermatology clinics in Europe, the USA, Japan, and Australia. Brit J of Derm. 2001:144:339–346.
18. Del Rosso J. Systemic therapy for rosacea: focus on oral antibiotic therapy and safety. Cutis. 2000;66(4S):7–14.
19. Walker DC, Cohen PR. Trimethoprim-sulfamethoxazole-associated acute febrile neutrophilic dermatosis: case report and review of drug-induced Sweet’s syndrome. J Am Acad Dermatol. 1996;34(5 Pt 2):918–923.
20. Wu AJ, Rodgers T, Fullen DR. Drug-associated histiocytoid Sweet’s syndrome: a true neutrophilic maturation arrest variant. J Cutan Pathol. 2008;35(2):220–224.
21. Knowles S, Uetrecht J, Shear N. Idiosyncratic drug reactions: the reactive metabolite syndromes. Lancet. 2000;356(9241):1587–1591.
22. Pashankar D, McArdle M, Robinson A. Co-trimoxazole induced aseptic meningitis. Arch Dis Child. 1995;73(3):257–258.
23. Mathews WA, Manint JE, Kleiss J. Trimethoprim-sulfamethoxazole-induced hypoglycemia as a cause of altered mental status in an elderly patient. J Am Board Fam Pract. 2000;13(3):211–212.
24. McKnight JT, Gaskins SE, Pieroni RE, Machen GM. Severe hypoglycemia associated with trimethoprim-sulfamethoxazole therapy. J Am Board Fam Pract. 1988;1(2):143–145.
25. Masters PA, O’Bryan TA, Zurlo J, Miller DQ, Joshi N. Trimethoprim-sulfamethoxazole revisited. Arch Intern Med. 2003;163(4):402–410.
26. Lavergne SN, Wang H, Callan H, et al. “Danger” conditions increase sulfamethoxazole-protein adduct formation in human antigen-presenting cells. J Pharmacol Exp Ther. 2009;331(2):372–381. Epub 2009 Aug 7.
27. Stockley I. Drug Interactions, 5th ed. London: Pharmaceutical Press; 1999.
28. Whittle SL, Hughes RA. Folate supplementation and methotrexate treatment in rheumatoid arthritis: a review. Rheumatology (Oxford). 2004;43(3):267–271. Epub 2004 Jan 6.
29. Keisu M, Wiholm BE, Palmblad J. Trimethoprim-sulphamethoxazole-associated blood dyscrasias. Ten years’ experience of the Swedish spontaneous reporting system. J Intern Med. 1990;228(4):353–360.
30. Myers MW, Jick H. Hospitalization for serious blood and skin disorders following co-trimoxazole. Br J Clin Pharmacol. 1997;43(6):649–651.
31. Heimpel H, Raghavachar A. Hematological side effects of co-trimoxazole. Infection. 1987;15(Suppl 5):S248–S253.
32. Antoniou T, Gomes T, Juurlink DN, et al. Trimethoprim-sulfamethoxazole-induced hyperkalemia in patients receiving inhibitors of the renin-angiotensin system: a population-based study. Arch Intern Med. 2010;170(12):1045–1049.
33. Perazella MA. Drug-induced hyperkalemia: old culprits and new offenders. Am J Med. 2000;109(4):307–314.
34. Mori H, Kuroda Y, Imamura S, et al. Hyponatremia and/or hyperkalemia in patients treated with the standard dose of trimethoprim-sulfamethoxazole. Intern Med. 2003;42(8):665–669.
35. Putcha N, Allon M. Management of hyperkalemia in dialysis patients. Semin Dial. 2007;20(5):431–439.
36. Loughlin J, Seeger JD, Eng P, et al. Risk of hyperkalemia in women taking ethinylestradiol/drospirenone and other oral contraceptives. Contraception. 2008;78(5):377–383. Epub 2008 Aug 8.
37. Dinger JC, Heinemann LA, Kühl-Habich D. The safety of a drospirenone-containing oral contraceptive: final results from the European Active Surveillance Study on oral contraceptives based on 142,475 women-years of observation. Contraception. 2007; 75(5):344–354. Epub 2007 Feb 23.
38. Koltun W, Lucky AW, Thiboutot D, et al. Efficacy and safety of 3mg drospirenone/20mcg ethinylestradiol oral contraceptive administered in 24/4 regimen in the treatment of acne vulgaris: a randomized, double-blind, placebo-controlled trial. Contraception. 2008;77(4):249–256. Epub 2008 Mar 4.
39. McAdams M, Staffa JA, Dal Pan GJ. The concomitant prescribing of ethinyl estradiol/drospirenone and potentially interacting drugs. Contraception. 2007;76(4): 278–281. Epub 2007 Aug 1.
40. Briggs G, Freeman R, Yaffe S. Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk, 5th ed. Baltimore: Williams and Wilkins; 1998.
41. Silverman W, Anderson D, Blanc W, et al. A difference in the mortality rate and incidence of kernicterus among premature infants allotted to two prophylactic antibacterial regimens. Pediatrics. 1956;18:614–624.
42. Strom BL, Schinnar R, Apter A, et al. Absence of cross-reactivity between sulfonamide antibiotics and sulfonamide nonantibiotics. N Engl J Med. 2003;349(17):1628–1635.
43. Zawodniak A, Lochmatter P, Beeler A, Pichler W. Cross-reactivity in drug hypersensitivity reactions to sulfasalazine and sulfamethoxazole. Int Arch Allergy Immunol. 2010; 153(2):152–156. Epub 2010 Apr 22.
44. Jick H, Derby L. A large population-based follow-up study of trimethoprim-sulfamethoxazole, trimethoprim, and cephalexin for uncommon serious drug toxicity. Pharmacotherapy. 1995;15(4):428–432.