Michael H. Gold, MD
Dr. Gold is the founder and medical director of Gold Skin Care Center, Advanced Aesthetics Medical Spa, The Laser and Rejuvenation Center, and Tennessee Clinical Research Center located in Nashville, Tennessee. He is also Clinical Assistant Professor at Vanderbilt University School of Medicine and School of Nursing in Nashville, Tennessee; Visiting Professor of Dermatology, Huashan Hospital, Fudan University, Shanghai, China; and Visiting Professor of Dermatology, No. 1 Hospital of China Medical University, Shenyang, China.
Introduction
Since the introduction of the first fractional thermolysis (FT) device in 2004, dermatologists have seen numerous FT technologies introduced into the marketplace, which has increased the armamentarium we have available for our patients to treat a variety of skin concerns. With so many devices now available with numerous claims of clinical success, deciding which FT device to use can be confusing. The author reviewed FT in 2007,[1] and it is his hope that this update brings further clarification to this ever-exciting world of FT.
It is crucial to state at the onset that all FT devices are not the same, and even though almost every laser company produces an FT device, research endeavors, presentations at major medical meetings, and, most importantly, scientific publications in peer-reviewed medical journals are needed for the legitimacy of FT devices. As clinicians, we should demand the science behind medical devices and not rely on the so-called “white” papers laser companies are eager to make available. Although the majority of laser company papers are sponsored clinical studies, those that have credence will have an institutional review board (IRB) approval for safety concerns and a peer-reviewed manuscript, which helps provide the legitimacy laser companies are so eager to achieve.
During the late 1990s and early 2000s, the gold standard for the treatment of facial lines and wrinkles as well as acne and traumatic scars was, at least from a laser point of view, the carbon dioxide (CO2) laser system. This laser was used, by most, in a continuous beam mode and removed all of the epidermis and a portion of the dermis. In the resultant wound-healing cascade, fibroplasia and neocollagensesis were evident in the treated areas. Downtime with the CO2 laser typically lasted about one week or more, and depending on the device and the aggressiveness of the clinician utilizing the device, potential adverse effects became more widespread. These potential adverse effects included pain, edema, persistent erythema, infections, postinflammatory hyperpigmentation, and the most problematic of all, hypopigmentation following the ablative procedure, seen in some patients two years following the laser surgery. Incidence rates for this postlaser hypopigmentation have varied from single digits to as high as 20 percent.[2] To counter these potential adverse events, the erbium:yttrium-aluminum-garnet (Er:YAG) laser was introduced. It has a higher absorption coefficient for water and theoretically should not produce the same adverse events as the “more powerful” CO2 lasers. In truth, postlaser hypopigmentation with the Er:YAG lasers still can occur as well as other problems similar to those of the CO2 laser. Downtime still may be from 5 to 7 days depending on the power utilized.[1]
Due to these “problems,” ablative laser resurfacing fell out of favor among many laser surgeons. Patients then began receiving rejuvenation treatments with near-infrared nonablative lasers, but with only minimal effects (as most would argue), and intense pulsed light (IPL) devices, which worked well for the treatment of pigment and vascular changes found on the skin, but had only minimal effects on collagen and elastin, thereby not providing the same results as ablative laser resurfacing in treating wrinkles and scars. The near-infrared lasers included various 1319 to 1320nm lasers as well as laser systems in the 1450 and 1540nm range. The 532nm potassium titanyl phosphate (KTP) laser and the 585 to 595nm pulsed dye lasers (PDL) also received attention in the rejuvenation arena, although they are much better at vascular treatments than rejuvenation.
Thus, laser surgeons were in a difficult period and were using devices that had only minimal clinical effects, but did not have the same downtime concerns of the ablative CO2 and Er:YAG laser systems. Then came along FT, and since its emergence five years ago, laser surgeons have been in a laser “resurfacing” renaissance.
History and Concepts Behind Fractional Thermolysis
The concept of FT was first described by Huzaira et al in 2003.[3] It was further elucidated by Manstein et al4 a year later with the first fraxelated laser system. FT was developed as a way for laser surgeons to get closer to ablative laser resurfacing clinical outcomes with less patient downtime and fewer overall adverse events. Simply stated, FT is the production of an injury pattern to the skin with skip areas repeated over and over again, which, as they heal, promote an improvement in the tone and texture of the skin, in lines and wrinkles, in pigmentary concerns including melasma, and in scars, especially acne and traumatic scars. Recently, studies have looked at the use of FT in the treatment of hypertrophic scars, keloids, and burn hypertrophic scars. Currently available devices vary in the way in which they produce their injury patterns, their wavelength, and their intensity.
In more technical terms, all of these devices produce small columns of thermal injury to the skin, which are known as microthermal zones (MTZs). These MTZs vary from device to device. Some are nonablative dermal injuries only; whereas, others are associated with ablative changes in the skin, causing both epidermal and dermal injury patterns. MTZs also vary greatly in their diameter of affect and in the degree of depth they achieve to create the injury. Once injured, the skin begins a very rapid process of repair. Through studies performed by Manstein et al, as well as others, we know that the repair mechanisms seen in FT occur through the transepidermal delivery of treated necrotic skin into the stratum corneum, in which it is exfoliated away in a very short time period. This process, in which the degenerated dermal material is incorporated into columns of debris to be sent to the epidermis, is known as microscopic epidermal necrotic debris (MENDs). MENDs is another term routinely associated with FT and appears unique to FT. The rapid healing process is made possible through the help of the surrounding “normal” or untreated skin—another process unique to FT.[4]
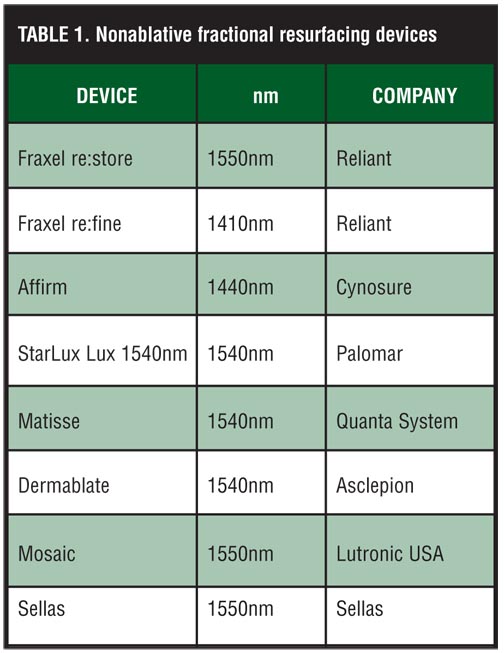
As noted, FT can be divided into several classifications. The easiest has been to classify FT devices into nonablative and ablative FT laser systems. This classification was “easy” at the beginning when only several devices were available. It is now a little more complex, especially among the ablative laser systems, thus new terminology seems prudent at this time. Ablative FT laser systems originally were divided into classifications based on laser type: CO2, Er:YAG, or yttrium-scandium-gallium-garnet (YSGG, 2790nm). What has changed is that different ablative FT laser systems emit light differently, with penetration depths that may be considered “superficial” and others that may be considered “deep.” Thus a new classification system seems prudent at this point. It has been suggested by Geronemus5 and others to classify ablative FT lasers into “micro-ablative FT laser systems,” which would include those lasers that produce epidermal and dermal damage to a depth less than 750 microns, and “deep dermal ablative FT laser systems,” which would include those lasers that produce damage beyond 750 microns in the skin. The classification systems, old and new, are shown in Table 1, Table 2, Table 3, Table 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Additionally, a new technology has recently been introduced and is known as sublative rejuvenation. It uses bipolar radiofrequency (RF) that has been fractionated and has been shown to deliver deep energy into the skin. This new technology is covered later in this article.
Current FT Devices—Nonablative
Numerous FT devices are available and all differ somewhat in energy delivery, injury patterns created, and intensity. They also differ in their clinical work as not all of the devices have peer-reviewed papers to support their treatment claims and successes, and rely on clinicians to “speak” on their devices or to be part of company-promoted “white papers,” which many laser surgeons do not endorse. The companies, as noted, need to perform IRB-approved clinical research and have the results published in peer-reviewed medical journals.
The first commercial FT device was a nonablative fractional laser known as Fraxel (Solta Medical, Inc., Hayward, California). In its original form, it utilized a blue optical guide material that allowed it to sense when the machine was in precise contact with the skin surface, then would allow the laser to fire. The Fraxel device set in motion FT as we know it today. The company behind the device sponsored very impressive clinical trials with skilled laser surgeons. Through the company’s efforts, along with a very smart public relations campaign and direct-to-consumer (DTC) advertising, FT emerged with a bang.
The original US Food and Drug Administration (FDA) clearance for the nonablative Fraxel device included its use for the coagulation of soft tissue, the treatment of periorbital rhytids, pigmented lesions, melasma, skin resurfacing, acne scars, and surgical scars. The literature has many examples of how well the nonablative Fraxel device performed for these indications and has recently been summarized in a review of FT technology by Tierney et al.[6]
The nonablative Fraxel device produces minimal patient discomfort. Some patients may require a topical anesthetic prior to the procedure and/or forced cool air cooling during the procedure. As a nonablative, 1550nm laser, the MTZs and MENDs produced were demonstrated first with this device. From a clinical point of view, most patients notice erythema and some edema, which can last for up to 48 hours following the treatment, followed by skin desquamation for several more days. With the Fraxel device and all nonablative fractional devices, there is usually a need for multiple treatments to achieve the final result. Most contend that 4 to 6 treatments are required to attain the given desired outcome for the majority of clinical indications.[6]
The blue dye became a “problem” with the original Fraxel device. The manufacturer made several modifications improving upon the original design, and blue dye is no longer required, making the procedure “cleaner.” The current device, known as the Fraxel Re:Store, is a market leader due to the amount of science behind the product. Many reports in the literature show the effectiveness of this and other FT devices, stating that these devices have been able to treat numerous modalities; however, case reports on various devices do not necessarily demonstrate total efficacy for a given disease or cosmetic defect. Therefore, larger scaled studies need to be performed and verified.
Clinical studies with regard to the nonablative fractional device include those of Manstein et al[4] in which significant improvements were found in periorbital lines and wrinkles with 54-percent improvement being seen by the end of one month in rhytids and in skin texture. At three months, they found 34-percent improvement in wrinkles and 47-percent improvement in skin texture. Geronemus[7] reported Fraxel improved fine-to-moderate rhytids as well as improvement in vertical lip lines. He concluded that deeper wrinkles were not as amenable to the Fraxel laser and that clinically his results for the full face were not as good as ablative regular Fraxel Re:Store. Jih et al[8] were the first to look at utilizing the Fraxel device on the hands in 10 patients. Improvements in pigmentation were noted to be between 51 and 75 percent in all of the patients at three months; and a 25- to 50-percent improvement rate was seen in skin roughness and skin wrinkling. Wanner et al[9] compared facial to nonfacial skin with the use of the Fraxel device. They found a mean clinical improvement of 2.23 at three months for the face and a mean of 1.85 off the face utilizing a 0 to 4 quartile grading scale. This trend continued for 6 and 9 months as well. Rahman et al10 also reported on the Fraxel device showing qualitative improvements in the treatment of photodamage, melasma, and rhytids. Mezzana et al[11] combined the Fraxel nonablative laser with the intense pulsed light (IPL) and found that the combination worked better than the Fraxel device alone in the 29 patients studied. The Fraxel device, as would be expected, stimulated dermal collagen and remodeling leading to improvements in rhytids and skin texture; whereas, the IPL helped with the dyschromia and telangiectasias associated with photodamage. Several authors have also published clinical studies on the treatment of melasma,[12–14] acne scars,[15,16] and other scars (i.e., hypopigmented scars,[17,18] surgical scars after Mohs surgery,[19] and striae distensae[20]), all of which support the use of nonablative FT.
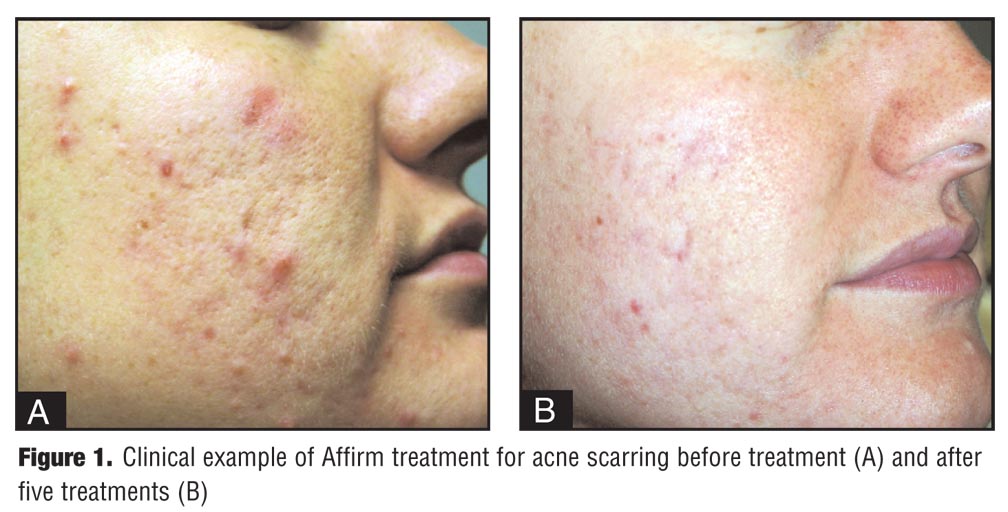
The next nonablative FT device to enter the market was known as the Affirm (Cynosure, Westford, Massachusetts). Its original design was that of a 1440nm FT laser in which the energy delivered was through a micro-array of lenses that yielded the desired FT results on the skin. This delivery of light through the array of lenses is known as combined apex pulse (CAP) technology. Through original work by Weiss et al[21] and other investigators, the Affirm was shown to be effective in the treatment of various skin concerns, including wrinkles, scars, and pigmentary concerns, such as melasma and Nevus of Ota.[22,23] The Affirm has received FDA approval for the treatment of periorbital and perioral wrinkles and pigmented lesions. Most patients require 3 to 6 treatments with the Affirm. Adverse events include post-treatment erythema and edema, which usually resolve within 24 hours, and most patients have very little, if any, downtime associated with the Affirm procedure. Advances to the Affirm device include the addition of a second wavelength of light, that being 1320nm, which is useful for skin tightening, to the 1440nm in what is known as a “multiplexed” event—both wavelengths firing during the same pulse of light making the procedure even more efficacious for the treatment of wrinkles and scars.[21] Clinical examples of the Affirm device are shown in Figure 1 and Figure 2.
{kind=link}
{kind=link}
Many other FT nonablative devices are available as well. However, peer-reviewed clinical papers regarding most of these lasers are lacking in the literature. They all work similarly to the previous lasers described, distributing nonablative laser energy into the dermis through pixilated columns or through an array of lenses, creating MTZs and MENDs, which lead to the desired clinical endpoints. These devices work over time, with multiple treatments usually required for the effect to be seen. The number of treatment sessions varies with nonablative FT devices, but most seem to achieve efficacy within 4 to 6 treatments, with treatment intervals usually spaced about four weeks apart. Downtime with nonablative FT devices does exist, with most patients experiencing erythema and edema for 24 to 48 hours postprocedure. Other adverse events to these devices appear to be negligible, except for the potential for postinflammatory hyperpigmentation (PIH), which is seen more commonly in darker skinned individuals. Proper pretreatment and post-treatment care should minimize the risk of PIH in susceptible individuals. The incidence of other serious adverse events, including scars, is not yet reported with the nonablative FT devices.
Current FT Devices—Ablative
At first, the ablative FT devices were nothing more than “regular” CO2 or Er:YAG devices with modified computer software programs, reduced spot sizes, and scanning devices that were tuned to provide skip areas.
The first of these introduced was the Active FX (Lumenis Aesthetic), which utilizes the UltraPulse platform, considered by some to be the gold standard for ablative resurfacing. The ActiveFX UltraPulse has a reduced spot size of 1.2mm and a superficial or microablative fractional laser energy distribution. The Active FX utilizes the original computer pattern generator (CPG) handpiece with updated technology, which spreads the injury patterns randomly as opposed to next to each other, as is the case with regular ablative resurfacing. Thus, the Active FX assures that the thermal relaxation time of the skin is not compromised as the fractionated holes are delivered.
The FDA approval for the Active FX includes disorders of the skin including wrinkles, rhytids, furrows (e.g., fine lines and texture irregularities), reduction/removal of uneven pigmentation/dyschromia, and acne scars. The majority of patients treated with the Active FX receive one to several treatments depending on what is being treated and have approximately 3 to 4 days of downtime. Work by Clementoni[24] has shown the effectiveness of the Active FX in the clinical world. Tan et al,[25] looking at a darker skinned population, found that the incidence of PIH as a result of the Active FX is very low. Weiss et al[26] also looked at the Active FX in a split-face comparison clinical trial with 10 patients receiving one Active FX treatment versus six FT treatments with the Fraxel ReStore. More than a 75-percent improvement was seen on the Active FX side at the conclusion of the study.[26]
A second computer-generated spot size for the UltraPulse utilizing a 0.12mm diameter spot and different software created what is known as the Deep FX. Berlin et al[27] evaluated this technology and has shown its safety and efficacy in delivering deep dermal ablative FT. The Deep FX can easily create “holes” up to 1mm deep. The contrasting spot sizes and dermal damage attainable with these devices is shown in Figure 3. Downtime with the Deep FX is reported to be 3 to 5 days, and once again, severe adverse events are minimal, with no reported cases of post-laser hypopigmentation.[28]
{kind=link}
In order to achieve the best results with the Active FX and the Deep FX, many are now combining the two modalities, with the first pass being the Deep FX and the second pass the Active FX. Collectively, this has been termed “Total FX” and, although it has the potential “best” benefits, it does have the most associated patient downtime (between 5–7 days) and potential for serious events, although nothing substantial has yet to be reported with the two settings together. A clinical example of the Active FX is shown in Figure 4 and Total FX is shown in Figure 5.
{kind=link}
{kind=link}
Other microablative fractional devices with clinical studies reported in the literature include the Pixel 2940nm FT laser (Gold Star Medical Photoelectric Technology Co., Ltd., Beijing, China), the SmartXide DOT CO2 laser (Deka Medical, Inc.), and the SmartSkin CO2 laser (CynoSure). Lapidoth et al[29] reported their experience with the Pixel 2940nm Er:YAG FT device. The Pixel has two energy modes, one that creates 81 pixels or dots and one that produces 49 dots for deeper penetration. In the work by Lapidoth et al, 28 patients with mild-to-moderate photodamage were treated with the Pixel device. At two months after the treatment, 75 percent of the patients rated the treatment as excellent and 25 percent rated it as good. This persisted for 6 to 9 months, showing the efficacy of the device. The FDA clearance for the Pixel 2940nm device includes skin resurfacing, wrinkle treatment, and scar revision (e.g., acne scars).
Recently, Gotkin et al[30] reported their experiences with a new microablative CO2 laser for FT, known commercially as the SmartXide DOT. Thirty-two patients were evaluated. Six months after one laser treatment, almost all of the patients reported a greater than 50-percent improvement in their wrinkles, epidermal pigment, and solar elastosis. In a report of another microablative CO2 laser (SmartSkin), Gold et al[31] treated 12 individuals with photodamage and acne scars. Two treatment sessions were given and improvement was noted in all patients in the 51 to 75-percent range.
Another deep dermal FT device with clinical trial experience includes the Fraxel RePair, which has had quite a number of investigations supporting its claims. The original work on this device by Hantash et al[32] demonstrated the deep dermal affects possible. Immunochemical staining demonstrated wound healing occurring for up to three months, leading the authors to believe that this deep dermal approach might have better clinical outcomes than nonablative FT. Several other published studies have confirmed this concept.[33,34]
With the Fraxel RePair, most patients require some sort of sedation for the procedure to be performed. This seems to be in deference to the majority of other ablative fractionated laser systems, which usually only require topical anesthesia in the majority of cases. Because this is a deep dermal FT system and produces some of the highest energies of all the ablative systems, several reports of adverse events (i.e., scarring) have recently been documented. We will likely continue to see an increase in adverse events with these machines, as more of them enter the market and are utilized by those who are not skilled laser surgeons.[35]
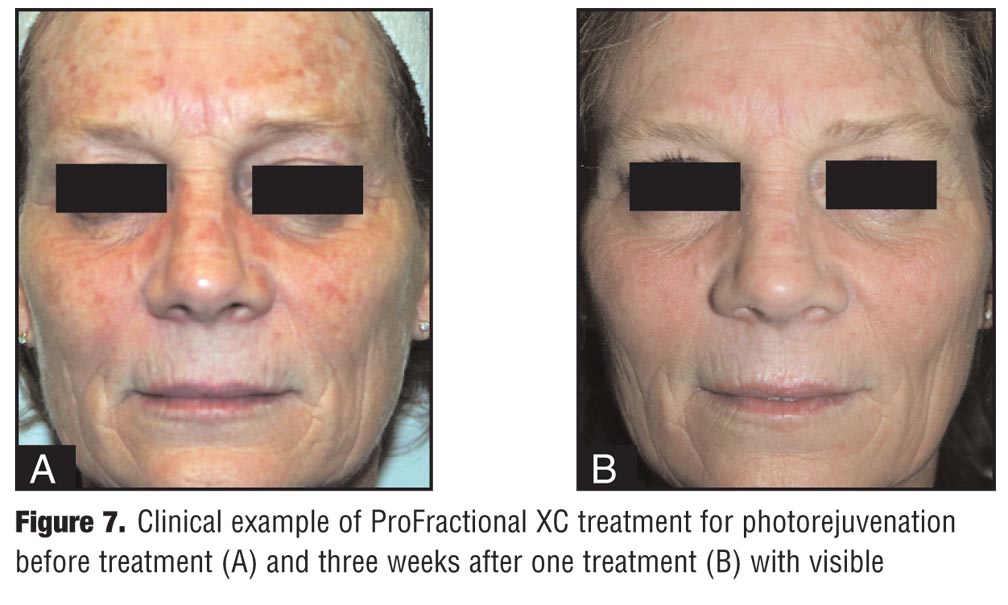
The final laser device to be discussed is the ProFractional (Sciton) Er:YAG FT system. It is also a deep dermal device that has the ability to have coagulation added to the fractional column, creating a deep dermal defect, which, histologically, mimics many of the CO2 FT devices. This is shown histologically in Figure 6.; a clinical example is shown in Figure 7.
{kind=link}
{kind=link}
Sublative Rejuvenation
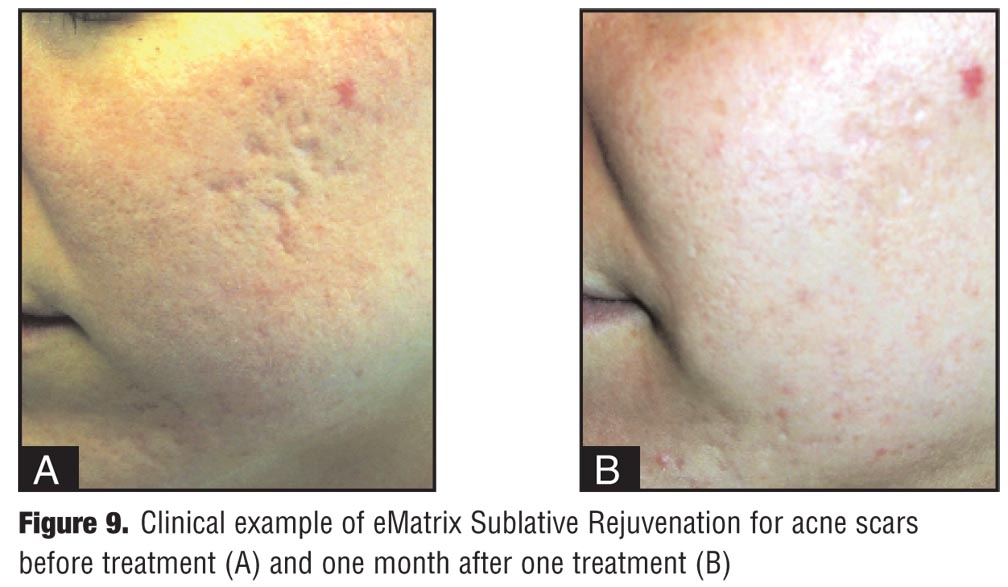
Sublative rejuvenation is the use of fractionated bipolar radiofrequency to produce a deep dermal heat,[36] as demonstrated in Figure 8. Clinical experience with this technology is progressing. Clinical examples for acne scars are shown in Figure 8 and Figure 9.
{kind=link}
{kind=link}
Conclusion
FT medical devices have been a revolution in the field of lasers. Many currently available FT devices work to improve photodamage, skin texture, and scars. Some are nonablative with minimal downtime and others are ablative with various degrees of downtime. Adverse events, such as PIH, may be kept to a minimum if proper pre- and post-skin care is given to the patients. Other adverse events, including scar formation, will be seen with more frequency unless proper training and education are given to those utilizing these machines.
Additional Tables
Table 5.
Table 6.
{kind=link}
{kind=link}
References
1. Gold MH. Fractional technology: a review and clinical approaches. J Drugs Dermatol. 2007;6(8):849–852.
2. Manuskiatti W, Fitzpatrick R, Goldman MP. Long-term effectiveness and side effects of carbon dioxide laser resurfacing for photoaged facial skin. J Am Acad Dermatol. 1999;40(3):401–411.
3. Huzaira M, Lodhi A, Khatri KA. Erbium:YAG laser skin resurfacing: a Pakistani experience. J Cosmet Laser Ther. 2003;5(1):43–49.
4. Manstein D, Herron GS, Sink RKH, et al. Fractional photothermolysis: a new concept for cutaneous remodeling using microscopic patterns of thermal injury. Lasers Surg Med. 2004;34(5):426–438.
5. Geronemus R. Personal communication, 2009.
6. Tierney EP, Kouba DJ, Hanke CW. Review of fractional photothermolysis: treatment indications and efficacy. Dermatol Surg. 2009;35(10):1445–1461.
7. Geronemus R. Fractional photothermolysis: current and future applications. Lasers Surg Med. 2006;38:169–176.
8. Jih MH, Goldberg LH, Kimyai-Asadi A. Fractional photothermolysis for photoaging of hands. Dermatol Surg. 2008;34(1):73–78.
9. Wanner M, Tanzi EL, Alster TS. Fractional photothermolysis: treatment of facial and nonfacial cutaneous photodamage with a 1550nm erbium-doped fiber laser. Dermatol Surg. 2007;33(1):23–28.
10. Rahman Z, Alam M, Dover JS. Fractional Laser treatment for pigmentation and texture improvement. Skin Therapy Lett. 2006;11(9):7–11.
11. Mezzana P, Valeriani M. Rejuvenation of the aging face using fractional photothermolysis and intense pulsed light: a new technique. Acta Chir Plast. 2007;49(2):47–50.
12. Rokhsar CK, Fitzpatrick RE. The treatment of melasma with fractional photothermolysis: a pilot study. Dermatol Surg. 2005;31(12):1645–1650.
13. Goldberg DJ, Berlin AL, Phelps R. Histologic and ultrastructural analysis of melasma after fractional resurfacing. Lasers Surg Med. 2008;40(2):134–138.
14. Naito SK. Fractional photothermolysis treatment for resistant melasma in Chinese females. J Cosmet Laser Ther. 2007;9(3):161–163.
15. Alster TS, Tanzi EL, Lazarus M. The use of fractional laser photothermolysis for the treatment of atrophic scars. Dermatol Surg. 2007;33(3):295–299.
16. Lee HS, Lee JH, Ahn GY, et al. Fractional photothermolysis for the treatment of acne scars: a report of 27 Korean patients. J Dermatol Treat. 2008;19:45–49.
17. Behroozan DS, Goldberg LH, Glaich AS, Dai T, Friedman PM. Fractional photothermolysis for treatment of poikiloderma of civatte. Dermatol Surg. 2006;32(2):298–301.
18. Glaich AS, Rahman Z, Goldberg LH, Friedman PM. Fractional resurfacing for the treatment of hypopigmented scars: a pilot study. Dermatol Surg. 2007;33:289–294.
19. Tierney E, Mahmoud BH, Srivastava D, Ozog D, Kouba DJ. Treatment of surgical scars with nonablative fractional laser versus pulsed dye laser: a randomized controlled trial. Dermatol Surg. 2009;35(8):1172–1180.
20. Kim BJ, Lee DH, Kim MN, et al. Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol. 2008;9(1):33–37.
21. Weiss RA, Gold MH, Bene N, et al. Prospective clinical evaluation of 1440nm laser delivered by microarray for treatment of photoaging and scars. J Drugs Dermatol. 2006;5(8):740–744.
22. Lloyd JR. Effect of fluence on efficacy using the 1440nm laser with CAP technology for the treatment of rhytids. Lasers Surg Med. 2008;40(6):387–389.
23. Kouba DJ, Fincher EF, May RL. Nevus of Ota successfully treated by fractional photothermolysis using a fractionated 1440nm Nd:YAG laser. Arch Dermatol. 2008;144(2):156–158.
24. Clementoni MT, Gilardino P, Muti GF, Beretta D, Schianchi R. Non-sequential fractional ultrapulsed CO2 resurfacing of photoaged facial skin: preliminary clinical report. J Cosmet Laser Ther. 2007;9(4):218–225.
25. Tan KL, Gold MH, Kurniawati C. Low risk of postinflammatory hyperpigmentation in skin types IV and V after treatment with fractional CO2 laser device. J Drugs Dermatol. 2008;7(8):774–777.
26. Weiss, RA, Weiss MA, Beasley KL. Prospective split-face trial of a fixed spacing array computer scanned fractional CO2 laser vs. hand scanned 1550nm fractional for rhytids. Lasers Surg Med. 2008;40(S20):31.
27. Berlin AL, Hussain M, Phelps R, Goldberg DJ. A prospective study of fractional scanned nonsequential carbon dioxide laser resurfacing: a clinical and histopathologic evaluation. Dermatol Surg. 2009;35(2):222–228.
28. Personal communication, Goldman MP, 2009.
29. Lapidoth M, Yagima Odo ME, Odo LM. Novel use of erbium:YAG (2940nm) laser for fractional ablative photothermolysis in the treatment of photodamaged facial skin: a pilot study. Dermatol Surg. 2008;34(8):1048–1053.
30. Gotkin RH, Sarnoff DS, Cannarozzo G, Sadick NS, Alexiades-Armenakas M. Ablative skin resurfacing with a novel microablative CO2 laser. J Drugs Dermatol. 2009;8(2):138–144.
31. Gold MH. Clinical Evaluation of the SmartSkin Fractional Laser for the Treatment of Photodamage and Acne Scars. Accepted for publication; J Drugs Dermatol. 2009;8(11):S4–S8.
32. Hantash BM, Bedi VP, Kapadia B, et al. In-vivo histological evaluation of a novel ablative fractional resurfacing device. Lasers Surg Med. 2007;39(2):96–107.
33. Walgrave SE, Ortiz AE, MacFalls HT, et al. Evaluation of a novel fractional resurfacing device for treatment of acne scarring. Lasers Surg Med. 2009;41(2):122–127.
34. Chapas AM, Brightman L, Sukal S, et al. Successful treatment of acneiform scarring with CO2 ablative fractional resurfacing. Lasers Surg Med. 2008;40(6):381–386.
35. Fife DJ, Fitzpatrick RE, Zachary CB. Complications of fractional CO2 laser resurfacing: four cases. Lasers Surg Med. 2009;41(3):179–184.
36. Hruza G, Taub AF, Collier SL, et al. Skin rejuvenation and wrinkle reduction using a fractional radiofrequency system. J Drugs Dermatol. 2009;8(3):259–265.