aShino Bay Aguilera, DO, FAOCD; bLiza Brown, DO; cViviana Andrea Perico, MD
aVolunteer Professor, Nova Southeastern University College of Osteopathic Medicine, Department of Dermatology, Fort Lauderdale, Florida
bDermatology Resident—PGY3, Larkin Community Hospital, Miami, Florida
cThird Year Aesthetic Medicine Resident, Rosario University, Bogota, Colombia
Disclosure: The authors report no relevant conflicts of interest.
Abstract
Bruxism is a diurnal or nocturnal parafunctional activity that includes unconscious clenching, grinding, or bracing of the teeth. An extensive medical history should be taken in these patients so proper diagnosis can be made. Habits such as biting the tongue, cheeks or lips, chewing gum or eating seeds for many hours per day, biting nails, and/or biting hard objects, will cause and/or exacerbate pre-existing bruxism. The etiology of bruxism is uncertain, but it is hypothesized to be associated with genetic, structural, and psychosocial factors. Over time, chronic clenching of the jaw leads to hypertrophy of masseters and temporalis musculature causing the face to take on a masculine and square appearance. Patients commonly present to dermatology cosmetic practices wishing to have a more slim, softer appearing face. This review is the first paper to discuss aesthetic treatment options for complications of bruxism including masseter and temporalis hypertrophy and the associated accelerated aging of the lower face. J Clin Aesthet Dermatol. 2017;10(5):49–55.
Bruxism was defined in 2008 by the American Academy of Orofacial Pain as a “diurnal or nocturnal parafunctional activity that includes unconscious clenching, grinding, or bracing of the teeth.”[1] Bruxism is different from the term temporomandibular disorder, which is used to describe diseases that affect the structures and functions related to the temporomandibular joint. In the case of bruxism, muscle contraction for long periods of time causes the characteristic symptoms of this disease. Therefore, it is important to note the muscles responsible for closing the jaw, which include the temporalis, masseter, and medial pterygoid. Proper knowledge of temporomandibular anatomy will facilitate diagnosis and treatment.[1],[2]
Patients with bruxism should be questioned regarding extensive medical history to include any bad oral habits that may exacerbate symptoms to help the examiner make an accurate diagnosis. During history-taking, the examiner should ask questions regarding nonfunctional jaw movements; biting the tongue, cheeks, or lips; chewing gum or eating seeds for many hours per day; biting nails; and/or biting hard objects.[3],[4] Many studies have shown that these habits reduce stress and anxiety temporarily, but can cause harmful effects on muscles and joints involved.[3],[5],[6]
Several studies report variable prevalence of bruxism, which is reported in roughly 8 to 31.4 percent of clinical cases in a 2013 systematic review.[7] Diurnal bruxism is more common in women while the nocturnal bruxism was found equally between genders, and interestingly was found to decrease with increasing age.[8]
Etiology
The etiology of bruxism is uncertain, but it is hypothesized to have multiple causes. These causes include the following:
• Genetic factors; 21 to 50 percent of people with sleep bruxism have a direct family member that had this disease during childhood.
• Occlusal interference; this refers to positional or structural abnormalities that can alter the bite.
• Psychosocial factors; of these, emotional stress is considered the main triggering factor.
• Anxiety, insomnia, and depression are important diagnoses, which will also perpetuate the disease state.
• Other causes include macrotrauma, smoking, systemic diseases, alcohol consumption, gastroesophageal reflux, and certain medications.[9–12]
Clinical Findings
The most common reported symptoms in association with bruxism include teeth grinding or clenching, abnormal tooth wear, sounds due to clenching and grinding associated with bruxism, jaw muscle discomfort, gingival inflammation, headache, temporomandibular joint pain, and destruction.[3],[10],[13] Over time, chronic bruxism will lead to hypertrophy of musculature, in particular the masseters and temporalis muscles.[2] With the clinical experience of the authors, the main aesthetic concern patients with bruxism have, is what they physically see; hypertrophy of masseters and temporalis. In other words, patients present wanting to change their facial structure because they either look too masculine or too square.
In addition to the signs and symptoms mentioned above, it is important to mention other symptoms that are not as common or that patients tend not to associate with bruxism, such as:
• Headache: May occur in the temporal and frontal region, usually when the patient wakes up in the morning. This can often be mistaken for migraine or sinusitis. Helping in the differential diagnosis, the patient may experience pain on palpation of these areas.[7],[14]
• Ocular pain, erythema, and photosensitivity may occur.[15]
• Decreased hearing, pruritus of the ear, otalgia, tinnitus and vertigo, and ear plugging sensation.[15–17]
• Oral discomfort; limited opening of mouth; lock jaw, whether shut or open; and reduction of salivary flow may be noted.[10]
• Jaw clicking, popping jaw points, jaw deviating to one side when opening of mouth, pain in muscles of cheeks and temporomandibular joint, uncontrollable jaw movements.7
• Throat: swallowing difficulties and sore throat without infection, laryngitis, voice irregularities or changes, frequent coughing or constant clearing of throat, feeling of foreign object in throat.[7],[17]
• Neck: lack of mobility, stiffness, pain, achy shoulders, and backache.[18]
Therefore, bruxism is a disease with a variable clinical presentation, making it difficult to diagnose. Diagnosis of other diseases in the differential may be made without expected improvement after treatment.
Aesthetic considerations
As mentioned earlier, patients usually present for secondary aesthetic consequences of bruxism, the most common being masseter hypertrophy. Although not often recognized, the premature or accelerated aging of the lower face can also be produced by this disease. While, aging is a physiological process that depends on inevitable intrinsic factors and modifiable extrinsic factors, the authors include bruxism and bad oral habits in the latter. In patients with bruxism, parafunctional habit and muscle hyperkinesis causes facial aging changes to occur at a younger age.[19],[20]
With advancing years, people suffer craniofacial changes, such as skin atrophy, ligamentous laxity, bone remodeling, and disturbance in superficial and deep fat compartments.[20–22] It is common that people will present for cosmetic concerns as bony support shrinks, nasal tip drops, columella-labial angle narrows, upper lip lengthens, lip vermilion thins and lines appear, loss of cupids bow is visualized, corners of the mouth turn down, and development of jowls occurs.[23] Clinically, authors note a person with bone loss characteristically has a more haggard and aged appearance, while facial fat loss makes people look more tired. The above becomes important when choosing the ideal treatment for the patient.
Treatment
The patient should be offered a comprehensive management plan while the condition being treated, identifying symptoms, and exacerbating factors is clearly explained.[2] In addition, patients may consider receiving joint/pain management via oral rehabilitation and psychology consults if stress-induced factors are causative factors for the bruxism.[5] In the authors’ clinical practice, they include self-care steps, botulinum toxin, and perioral rejuvenation as part of the comprehensive care plan in patients diagnosed with bruxism.
Self-care steps. One of the mainstays of bruxism treatment is that the patient is aware of the disease, and based on literature reports, follows these self-care measures:
• Applies ice or wet heat to sore jaw muscles.
• Avoids eating hard foods like nuts, candies, and steak.
• Avoids chewing gum.
• Averts jaw play and other bad oral habits. This refers to nonfunctional jaw movements without tooth physical touching.
• Drinks plenty of water every day.
• Gets plenty of sleep.
• Learns physical therapy stretching exercises to help restore the action of the muscles and joints on each side of the head to get back to normal.
• Massages the muscles of the neck, shoulders, and face. Looks for small, painful nodules called trigger points that can cause pain throughout the head and face.
• Relaxes the face and jaw muscles throughout the day. The goal is to make facial relaxation a habit.
• Tries to reduce daily stress and learn relaxation techniques. • Wears a properly fitted mouth guard at night while sleeping. • Recommend taking L-theanine 100 to 200mg orally daily to help cope with stress
• Recommend magnesium-containing teas or tablets for nocturnal muscle relaxation.
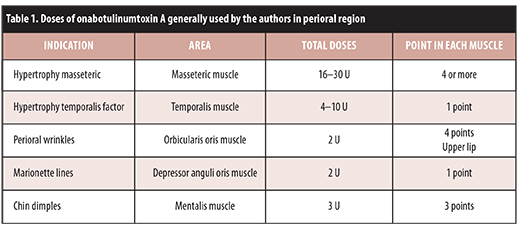
Botulinum toxin. In addition to self-care techniques, treating masseteric hypertrophy with botulinum toxin will relax the muscle and help improve the symptoms of pain, fatigue, and spasm.[12],[24] The authors use a 1mL 5/16” 31g insulin syringe and typically inject a total of 16 to 30 units of onabotulinumtoxin A into each masseter muscle (depending on the degree of hypertrophy), and 4 to 10 units in each temple area approximately 1.5cm superior to the zygomatic arch for muscle relaxation.[2] Needle length may be adjusted according to physician preference and degree of muscle hypertrophy (Figure 1 and Table 1 ). Interestingly, during follow-up, several patients reported remission of other symptoms that they had not associated with the disease. Resolution of vertigo, has attracted the most attention.
{kind=link}
{kind=link}
Perioral rejuvenation. In the management of the perioral area, the authors find it important to identify areas of concern for the patient and focus on the anatomical changes that are causing these changes. It is important to preserve bone structure to give adequate support to the lower third of the face. Facial aging is a multifactorial process. Ptosis, loss of elasticity, repetitive facial expressions (as seen with bruxism), gravity, and extrinsic factors of aging all contribute to the negative appearance of facial aging. This negative appearance is associated with the look of concern and sadness at an older age. Understanding facial anatomy and underlying musculature is of utmost importance when considering rejuvenation procedures. The aging face is more difficult to treat with botulin toxin alone when it is due to volume loss. In this case, fillers and lasers become options for correction of the aging face.[25],[26] To provide the best results, a full face combined treatment modality approach should be considered to include lateral face and temples; tear toughs and periorbital complex; midface; and lower face, including chin, marionette, and jaw line.
Combining botulinum toxin, fillers, and laser resurfacing has been shown to provide better, longer-lasting results when used in combination. Combination therapy provides superior results because botulinum toxin decreases perioral muscle contraction and increases the longevity and durability of the filler. This concept is true regarding botulinum toxin increasing longevity of hyaluronic acid fillers in all areas of the face including cheek volumization.
The use of botulinum toxin is a valuable resource and important tool for decreasing expression causing perioral wrinkles. For example, when the patient tends to pucker lips, vertical marionette lines become visible, labial commissures are depressed, and chin dimples ensue.[27],[28] Generally, authors use doses (Table 1) that are within the lower ranks of those reported in the literature so complications are avoided and there are greater safety margins.
There are many fillers available for facial rejuvenation procedures. Hyaluronic acid (HA) dermal fillers are versatile agents for volume loss of the face. HA is a naturally occurring glycosaminoglycan essential for tissue growth and wound healing and its ability to absorb water makes it a great choice for a filler that is instantaneously pleasing. There are several HA fillers available that differ in particle size, chain length, degree of HA concentration, crosslinking, gel consistency, gel hardness, viscosity, and degree of solubility in water. Enzymatic breakdown of product occurs over six months in most fillers and up to two years in products that have the highest G’ (most stiff particle).[29]
Calcium hydroxyapatite fillers stimulate endogenous collagen and exhibit greater duration of action than the HA group. Supraperiosteal injection of these fillers with post-injection massage is crucial.[30] Authors like to use this product for volume loss of the cheeks, prejowl sulcus, and jaw recontouring in combination with other biostimulatory agents.[31]
Poly-L lactic acid is a biostimulatory agent that gradually replaces and corrects bony and soft tissue deformities of the aging face, greatly correcting volume loss. First approved in 2009 for aesthetic cosmetic use, poly-L lactic acid has become a very important tool in the cosmetic dermatologist’s armamentarium. As with all cosmetic procedures, counseling is a very important part of patient care. Patients should understand that rejuvenation will have delayed gratification as results do not appear until a few months after the first injections, consistent with our bodies’ natural neocollagenesis.[32] The authors of this article believe combination therapy is crucial to improvement in volume loss, with poly-L lactic acid being a mainstay in treatment management.
In advanced cases of bone resorption of the aging face and/or with dental health issues, increasing facial volume may lead to an overdone appearance. In these cases, dental restoration and plastic surgery implants may be necessary.[26]
Botulinum toxin has shown to also reduce facial rhytids when used following laser resurfacing. The mechanism is believed to improve resurfacing and rejuvenation outcomes by reducing wound tension, allowing for re-epithelialization and collagen remodeling.[27] This proves that a triple combination of botulinum toxin, fillers, and lasers will provide greatest results for rejuvenation of the aging face.
Carbon dioxide and erbium-YAG ablative lasers have been the mainstay for full facial resurfacing for improving wrinkles and producing a skin-tightening effect. These results are achieved by denudation of the epidermis via thermal injury. Despite great clinical improvement, downtime may last up to several weeks and potential complications include scarring, edema, erythema, hypo/ hyperpigmentation, milia, and infection, to name a few.[32] With the advent of fractional thermolysis (fractionated columns of ablation, sparing much of the epidermis), many patients opt for this minimally invasive procedure with less downtime and its favorable benefit-to-risk ratio, when compared to full facial resurfacing.[33]
Nonablative resurfacing is another modality using a variety of wavelengths. Treatments have been shown to improve mild-to-moderate wrinkles, skin laxity, and overall skin condition. Multiple treatments are necessary, but downtime is minimal and treatment is well-tolerated. Non-ablative Nd:YAG lasers work via cooling the epidermis, while causing injury to the dermis, sparing epidermal injury, and boosting collagen production. As this type of laser does not cause injury to melanin, it is an excellent choice for rejuvenation of the face in darker skinned patients as well.[32]
Ablative and non-ablative lasers may be used concurrently in addition to other treatment modalities, such as intense pulsed light (IPL) treatments and other newer therapies including ultrasound and radiofrequency skin tightening procedures. These treatment options are non to minimally invasive options for reduction of photodamage via IPL and treating skin laxity and tightening with ultrasound and radiofrequency. A case report by Friedmann et al [34] used IPL therapy in combination with poly-L lactic acid and microfocused ultrasound tightening with excellent results for improvement of the aging face. This combined approach was performed in one single treatment day.[34]
Conclusion
In conclusion, bruxism is a disease that includes unconscious clenching, grinding, or bracing of the teeth. While the etiology of bruxism is uncertain, it is hypothesized to be associated with genetic, structural, and psychosocial factors.9–11 Clinical presentation of bruxism is variable and treatment may be delayed by misdiagnoses due to misleading symptoms, such as headache, vertigo, ocular pain, otalgia, and pain in mouth/throat.[3],[10],[16–18] Chronic clenching of the jaw will lead to masseter and temporalis hypertrophy, premature bone loss and problems with dentition. Patient’s with undiagnosed bruxism will commonly present to dermatology offices with the complaint of appearing too masculine or having a squared appearance to the face. Although not often recognized, bruxism will also lead to a premature aging face and facial volume loss.[19] Patients should be treated with a comprehensive management plan, while clearly understanding the condition being treated, identifying symptoms, and avoiding exacerbating factors. These factors mentioned previously include biting the tongue, cheeks, or lips; chewing gum or eating seeds for many hours per day; biting nails; and/or biting hard objects.[3],[4] Psychosocial factors including anxiety and depression, smoking, systemic diseases, alcohol consumption, gastroesophageal reflux, and certain medications will complicate bruxism. A genetic cause is noted in 21 to 50 percent of patients.[9–11]
Self-care tips are important primary treatment approaches for the management of bruxism. Aesthetic treatments aim to improve masseter and temporalis hypertrophy as well as restore facial volume loss to allow the aging face to do so gracefully. There are many tools in a physician’s armamentarium to aid in this process from botulinum toxin to numerous fillers and various laser and light therapies. It is now known that the aging face is best treated with a full face comprehensive approach using multiple treatment modalities.
References
1. Quadri MFA, Mahnashi A, Al Almutahhir A, et al. Association of awake bruxism with khat, coffee, tobacco, and stress among Jazan University students. Int J Dent. 2015;2015. Article ID 842096.
2. Schwartz M, Freund B. Treatment of temporomandibular disorders with botulinum toxin. Clin J Pain [Internet]. 2002;18(6 Suppl):S198–203. http://www.ncbi.nlm.nih.gov/ pubmed/12569969.
3. Winocur E, Gavish a, Finkelshtein T, et al. Oral habits among adolescent girls and their association with symptoms of temporomandibular disorders. J Oral Rehabil. 2001;28(7):624–629.
4. Lavigne GJ, Khoury S, Abe S, et al. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;35(7):476–494.
5. Weijenberg RAF, Lobbezoo F. Chew the pain away: oral habits to cope with pain and stress and to stimulate cognition. Biomed Res Int [Internet]. 2015;2015:1–7. http://www.hindawi.com/ journals/bmri/2015/149431/.
6. Tabrizi R, Karagah T, Aliabadi E, Hoseini SA. Does gum chewing increase the prevalence of temporomandibular disorders in individuals with gum chewing habits? J Craniofac Surg [Internet]. 2014;25(5):1818–1821. http://content. wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00001665-201409000-00055.
7. Murali RV, Rangarajan P, Mounissamy A. Bruxism: conceptual discussion and review. J Pharm Bioallied Sci [Internet]. 2015;7(Suppl 1):S265–S270. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=4439689&tool=pmcentrez&rendertype=abstract.
8. Shetty S, Pitti V, Babu CLS, et al. Bruxism: a literature review. J Indian Prosthodont Soc. 2010;10(3):141–148.
9. Carra MC, Huynh N, Lavigne G. Sleep bruxism: a comprehensive overview for the dental clinician interested in sleep medicine. Dent Clin North Am. 2012;56(2):387–413.
10. Ohayon MM, Li KK, Guilleminault C. Risk factors for sleep bruxism in the general population. Chest. 2001;53–61.
11. Chisnoiu AM, Picos AM, Popa S, et al. Factors involved in the etiology of temporomandibular disorders—a literature review. Clujul Med. [Internet]. 2015;88(4):473. http://www.clujulmedical.umfcluj.ro/ index.php/cjmed/article/view/485.
12. Article R. Bruxism?: a literature review. 2014;6(August):105–109.
13. Kesikburun S, Alaca R, Aras B, et al. Botulinum toxin injection for bruxism associated with brain injury: case report. J Rehabil Res Dev. 2014;51(4):661–664.
14. Glaros AG, Urban D, Locke J. Headache and temporomandibular disorders: evidence for diagnostic and behavioural overlap. Cephalalgia. 2007;27(6):542–549.
15. Michalak M, Wysoki?ska-Miszczuk J, Wilczak M, et al. Correlation between eye and ear symptoms and lack of teeth, bruxism and other parafunctions in a population of 1006 patients in 2003–2008. Arch Med Sci. 2012;8(1):104–110.
16. Ramírez LM, Ballesteros LE, Sandoval GP. Síntomas óticos referidos en desórdenes temporomandibulares. Relación con músculos masticatorios. Rev Med Chil. 2007;135(12):1582–1590.
17. Ferendiuk E, Zajdel K, Pihut M. Incidence of otolaryngological symptoms in patients with temporomandibular joint dysfunctions. Biomed Res Int. 2014;2014. Article ID 824684.
18. Santamato A, Panza F, Di Venere D, et al. Effectiveness of botulinum toxin type A treatment of neck pain related to nocturnal bruxism: A case report. J Chiropr Med [Internet]. 2010;9(3):132–137. http://dx.doi.org/ 10.1016/j.jcm.2010.04.004.
19. Steed PA. The longevity of temporomandibular disorder improvements after active treatment modalities. Cranio. 2004;22(2):110–114.
20. Khavkin J, Ellis DAF. Aging skin: histology, physiology, and pathology. Facial Plast Surg Clin North Am. [Internet]. 2011;19(2):229–234. http://dx.doi.org/10.1016/j.fsc.2011.04.003
21. Wong CH, Mendelson B. Newer understanding of specific anatomic targets in the aging face as applied to injectables: aging changes in the craniofacial skeleton and facial ligaments. Plast Reconstr Surg. [Internet]. 2015;136(5 Suppl):44S–48S. http://www.ncbi.nlm.nih.gov/pubmed/26441110.
22. Fitzgerald R, Rubin AG. Filler placement and the fat compartments. Dermatol Clin [Internet]. 2014;32(1):37–50. http://dx.doi.org/ 10.1016/j.det.2013.09.007
23. Sadick NS, Manhas-Bhutani S, Krueger N. A Novel approach to structural facial volume replacement. Aesthetic Plast Surg. 2013;37(2):266–276.
24. Azam A, Manchanda S, Thotapalli S, Kotha SB. Botox therapy in dentistry?: a review. J Int Oral Health. 2015;7(Suppl 2):103–105.
25. Goldman A, Wollina U. Elevation of the corner of the mouth using botulinum toxin type a. J Cutan Aesthet Surg. [Internet]. 2010;3(3):145–150. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3047731&tool=pmcentrez&rendertype=abstract.
26. Wollina U, Payne CR. Aging well—the role of minimally invasive aesthetic dermatological procedures in women over 65. J Cosmet Dermatol. 2010;9(1):50–58.
27. Danhof RS, Cohen JL. A combination approach to perioral rejuvenation. J Drugs Dermatol. 2016;15(1):111–112.
28. Carruthers J, Fournier N, Kerscher M, et al. The convergence of medicine and neurotoxins: A focus on botulinum toxin type A and its application in aesthetic medicine—a global, evidence-based botulinum toxin consensus education initiative: Part II: incorporating botulinum toxin into aesthetic clini. Dermatol Surg. 2013;39(3 PART 2):510–525.
29. Yasaman Mansouri, Gary Goldenberg. Update on hyaluronic acid fillers for facial rejuvenation. Cutis. 2015;96(2):85–88.
30. Sadick NS, Dorizas AS, Krueger N, Nassar AH. The facial adipose system. Dermatol Surg [Internet]. 2015;41:S333–S339. http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00042728-201512001-00009.
31. Dallara JM, Baspeyras M, Bui P, et al. Calcium hydroxylapatite for jawline rejuvenation: consensus recommendations. J Cosmet Dermatol. 2014;13(1):3–14.
32. Dayan SH, Vartanian a J, Menaker G, et al. Nonablative laser resurfacing using the long-pulse (1064nm) Nd:YAG laser. Arch Facial Plast Surg [Internet]. 2014;5(4):310–315. http://www.ncbi.nlm.nih.gov/pubmed/12873868.
33. Kohl E, Meierhöfer J, Koller M, et al. Fractional carbon dioxide laser resurfacing of rhytides and photoaged skin—a prospective clinical study on patient expectation and satisfaction. Lasers Surg Med. 2015;47(2):111–119.
34. Friedmann DP, Fabi SG, Goldman MP. Combination of intense pulsed light, Sculptra, and Ultherapy for treatment of the aging face. J Cosmet Dermatol. 2014;13(2):109–118.