Matthias Imhof, MD; Ulrich Kühne, MD
Ästhetische Dermatologie, Medico Palais Bad Soden, Bad Soden, Germany
Disclosure: Drs. Imhof and Kühne had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. In the last five years, Drs. Imhof and Kühne have attended and presented in workshops and meetings for Merz Pharmaceuticals GmbH, Germany, and have received financial support from Merz Pharmaceuticals GmbH, Germany. This study was supported by Merz Pharmaceuticals GmbH, which was involved in the design and conduct of the study; in the collection, analysis, and interpretation of data; and in the preparation, review, and approval of this manuscript.
Clinical trials registration: Safety and Efficacy of NT 201, Free of Complexing Proteins, in the Treatment of Glabellar Frown Lines,
ID number: NCT00694148. Registry: www.clinicaltrials.gov
Abstract
Objective: To investigate the efficacy and safety of incobotulinumtoxinA (also known as botulinum toxin type A [150 kDa], free from complexing proteins, or previously as NT 201), for the treatment of glabellar frown lines, in a prospective, open-label, multicenter, Phase III trial. Design: The study was a prospective, open-label, multicenter, international, Phase III clinical study. Subjects with moderate-to-severe glabellar frown lines at maximum frown, as assessed by the investigator according to the facial wrinkle scale, were given one intramuscular treatment of 20U incobotulinumtoxinA, administered as 0.1mL to each of five injection sites, and assessed over 84 days. Missing values were imputed using the baseline value or next observation carried backwards. Adverse events were documented for the duration of the study. Settings: Two centers in Russia and one center in Germany. Participants: A total of 105 subjects (18–65 years) with moderate-to-severe glabellar frown lines at maximum frown were enrolled. Measurement: The primary endpoint was the percentage of responders at maximum frown (improvement of ?1 on the facial wrinkle scale when compared with Day 0) on Day 28, as assessed by the investigator. Results: Response to treatment with incobotulinumtoxinA with respect to the facial wrinkle scale at maximum frown on Day 28 and Day 84 was 98.1 and 80.0 percent, respectively (missing values imputed). At rest, 94.3 percent (imputed values) of subjects were responders on Day 28 while 81.9 percent were responders on Day 84 (imputed values). Consistent with assessment by the investigators, subjects also rated treatment success highly. Incidence of treatment-related adverse events was low and no patients developed neutralizing antibodies. Conclusion: IncobotulinumtoxinA is effective in the treatment of glabellar frown lines and is well tolerated. (J Clin Aesthet Dermatol. 2011;4(10):28–34.)
Botulinum type A toxins (BTX-A) have been used therapeutically for more than 25 years for the treatment of conditions associated with excessive muscle contraction and for more than 20 years in the aesthetics arena.[1] The first report in the medical literature on the use of botulinum preparations in glabellar frown lines was published in 1992,[2] and several reports have since followed.[3–9] Glabellar frown lines are caused by contraction of the corrugator muscles above the eyebrows.[10] These frown lines often become more prominent with age and can project negative emotions unintentionally.[6]
IncobotulinumtoxinA (also known as botulinum toxin type A [150 kDa], free from complexing proteins, or NT 201; Xeomin®/Xeomeen®/Bocouture®; Merz Pharmaceuticals GmbH, Germany) is a BTX-A, which, in contrast to other commercially available preparations, is free from complexing proteins and contains only active neurotoxin.[11] IncobotulinumtoxinA has demonstrated noninferiority to a conventional botulinum toxin 900 kDa complex (onabotulinumtoxinA, Botox®/Vistabel®, Allergan Inc., United States) in aesthetic treatment, such as glabellar frown lines in a large, multicenter, head-to-head study involving 381 patients.[9] Noninferiority has also been confirmed in two large head-to-head studies for the treatment of cervical dystonia[12] and blepharospasm.[13] In addition, incobotulinumtoxinA has demonstrated efficacy in post-stroke upper limb spasticity.[14] The product was first launched in 2005 for central nervous system (CNS) indications. Since July 2009, it has also been approved and marketed for the treatment of glabellar frown lines in Germany and has now also been launched in all major European markets as well as Russia, Mexico, and Argentina.
IncobotulinumtoxinA is synthesized by a wild-type strain of Clostridium botulinum, which produces distinct neurotoxins with associated proteins as part of a high molecular weight complex.[15] During the manufacturing process, a number of purification steps are carried out to separate the neurotoxin from the complexing proteins to yield only the active neurotoxin.[16] From a clinical standpoint, the lack of complexing proteins may convey an advantage, as their presence has been associated with eliciting an immune response.[17] This has been corroborated in animal models, where neutralizing antibodies were detected in rabbits following repeated intradermal administration of conventional complexing protein-containing preparations of botulinum toxin (onabotulinumtoxinA; abobotulinumtoxinA/ Dysport®, Ipsen Ltd., United Kingdom), but were not produced after incobotulinumtoxinA was administered.[18] The development of neutralizing antibodies in humans following aesthetic treatment with BTX-A is rare; however, there have been several reports of treatment failure that is suggestive of the presence of neutralizing antibodies to BTX-A.[19,20] Additionally, Dressler et al reported antibody-induced treatment failure in four cases following treatment with onabotulinumtoxinA, abobotulinumtoxinA, or an ona-botulinumtoxinA and abobotulinumtoxinA combination.[21]
The aim of this study was to investigate the efficacy and tolerability of incobotulinumtoxinA in the treatment of glabellar frown lines. Secondary objectives were to further evaluate the treatment effect of incobotulinumtoxinA on glabellar frown lines at maximum frown and at rest, as assessed by the investigators and patients.
Methods
This study was a prospective, open-label, international, Phase III trial performed in two centers in Russia and one center in Germany, all of which were experienced in the treatment of glabellar frown lines. The study was approved by the Independent Ethics Committee and was conducted according to the recommendations of Good Clinical Practice, the 1975 Declaration of Helsinki, and the applicable regulatory requirements. Informed consent was obtained from each patient before any study-related procedures were initiated.
Subjects 18 to 65 years of age with moderate-to-severe glabellar frown lines at maximum frown (severity score of 2 or 3 on the Facial Wrinkle Scale [FWS]), as assessed by the investigator, and who were in a stable medical condition were eligible for the study. The medical condition of subjects was assessed by physical examination, medical history, laboratory evaluation, and vital signs during Visit 1 (Day -7, screening visit). Exclusion criteria included previous treatment with botulinum toxin of any serotype in the upper third of the face within the last six months, treatment with biodegradable fillers or insertion of permanent material in the glabellar area within the last 12 months, any surgery or scars in the glabellar region, and any marked facial asymmetry or ptosis of the eyelid and/or eyebrow. Also excluded were subjects with any infection in the area of the injection sites or any medical condition that put them at increased risk with exposure to incobotulinumtoxinA, including disorders that could interfere with neuromuscular function.
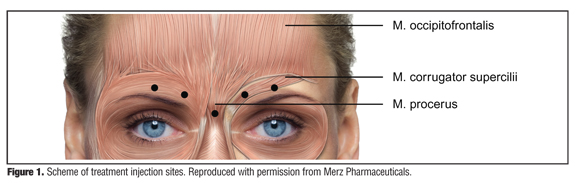
The duration of the study was 84 days with a seven-day screening period to assess subject eligibility. At Visit 2 (Day 0), subjects received a total dose of 20U incobotulinum-toxinA, administered as intramuscular injections at five sites. The total injection volume of 0.5mL was divided equally between injection sites (0.1mL per injection site; equivalent to 4U incobotulinumtoxinA) in the procerus muscle, the central part of both corrugator muscles at least 1cm above the bony orbital rim, and the lateral part of both corrugator muscles at least 1cm above the bony orbital rim (Figure 1). During the observation period of 84 days, subjects attended the study center for Visit 3 (Day 28) and Visit 4 (Day 84). At each visit, efficacy assessments were made by both the investigator and the subject at maximum frown and at rest.
{kind=link}
The primary efficacy endpoint was the proportion of subjects with improvement in physician-rated glabellar frown line severity at maximum frown on Day 28. Glabellar frown line severity was evaluated using the FWS four-point scale: 0=none, 1=mild, 2=moderate, and 3=severe. A responder was defined as a subject achieving an improvement of at least one point on the FWS on Day 28 when compared with Day 0. Secondary endpoints included the proportion of responders at rest on Days 28 and 84 and the proportion of responders at maximum frown on Day 84, as assessed by the investigator according to the FWS.
Glabellar frown line severity was also self-assessed by subjects using the 4-point Patient’s Assessment Scale (PAS; rating at maximum frown: 0=no muscle action at all, 1=some even slight muscle action possible, 2=moderately strong muscle action possible, 3=strong muscle action possible, which may cause local pallor; and rating at rest: 0=no visible vertical line(s) at all, 1=slightly visible vertical line(s), 2=moderate vertical line(s) with depression, 3=deep vertical line(s) and depression, which cannot be effaced by spreading). Subjects rated their PAS values at maximum frown and at rest on Days 28 and 84. A subject was defined as a responder when they had achieved an improvement of at least one point on the four-point scale compared with Day 0. Additionally, subjects performed further self-assessment using the 9-point Patient’s Global Assessment (PGA) in response to the question: “How would you rate the change in the appearance of your glabellar lines compared with the situation immediately before the injection?” The potential PGA rating responses were: +4=complete improvement, +3=marked improvement, +2=moderate improvement, +1=slight improvement, 0=unchanged, -1=slight worsening, -2=moderate worsening, -3=marked worsening, -4=very marked worsening. Subjects also rated PGA values on Days 28 and 84, with a responder defined as a person achieving a score of at least +2 points.
The type, severity, causal relationship and seriousness of adverse events (AEs), and signs and symptoms that could indicate spread of the neurotoxin, were recorded throughout the duration of the study. For AEs and serious AEs, frequencies and proportions of subjects with events are given. In addition, blood samples were taken from subjects at screening and Day 84 for clinical biochemistry and hematology analysis. The blood samples were also used in a fluorescence immunoassay to detect BTX-A antibodies. If positive, the hemidiaphragm assay was performed to test for neutralizing antibodies.[22]
All enrolled and treated subjects with a FWS measurement at maximum frown on Day 0 were included in the Full Analysis Set (FAS). The Per Protocol Set (PPS) included the subset of subjects of the FAS for whom no major protocol violations were reported. A parametric two-sided 95-percent confidence interval was calculated for the primary and secondary efficacy endpoints. The confirmatory analysis of the primary endpoint was performed on the FAS, with missing values imputed for Day 28 using the next observation carried backwards. If the next value for Day 84 was also missing, a worst-case strategy was applied by imputing the FWS value on Day 28 by the respective baseline value, and therefore assuming the subject was a nonresponder. In order to investigate the strength of the findings, sensitivity analyses were conducted on the FAS with observed cases only. All subjects who had received study treatment were part of the Safety Evaluation Set (SES), and safety analyses were based only on the SES.
Results
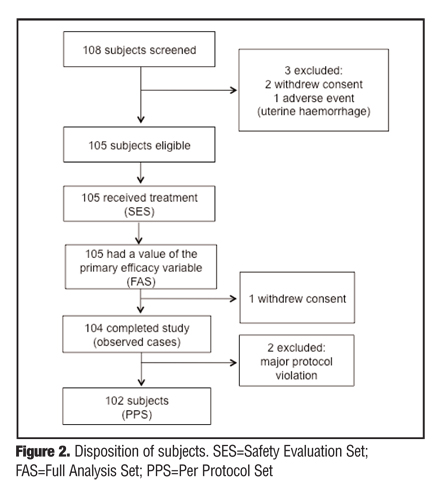
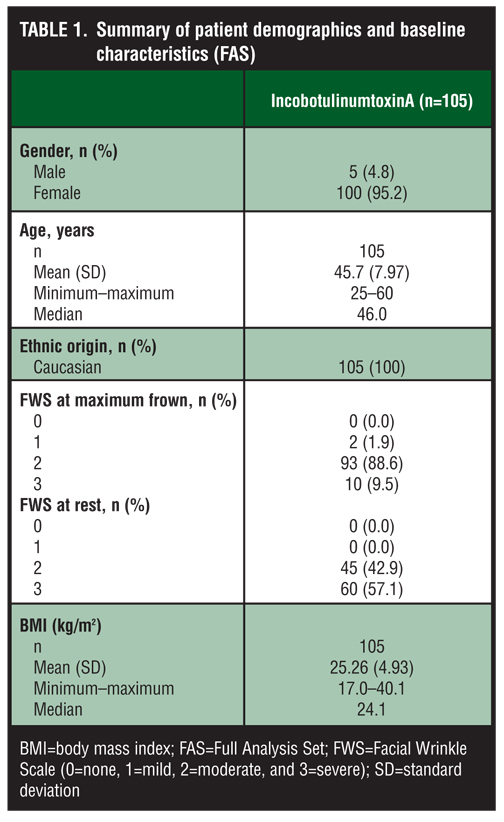
In total, 105 subjects received incobotulinumtoxinA for moderate-to-severe glabellar frown lines (Figure 2). A value for the primary efficacy endpoint was recorded for these participants and therefore all were included in the FAS. A total of three subjects were excluded from the PPS after withdrawing consent (n=1) or showing major deviations from the study protocol (n=2), and therefore the PPS population consisted of 102 subjects. The demographics and baseline characteristics of the FAS are presented in Table 1.
{kind=link}
{kind=link}
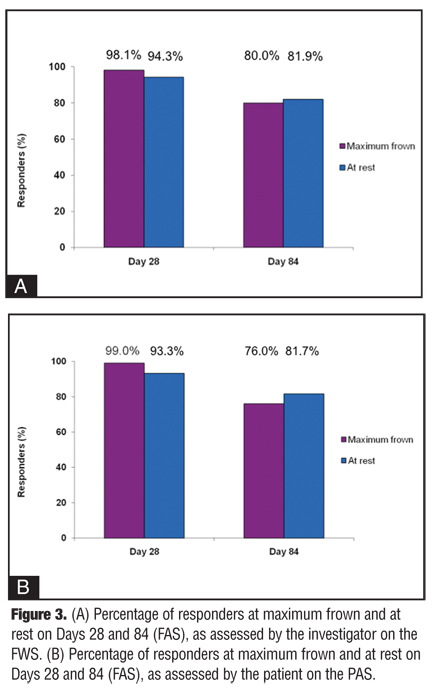
With respect to the primary efficacy endpoint, the response rate to treatment with incobotulinumtoxinA at maximum frown was high. On Day 28, 98.1 percent (n=103; 95% CI: 0.933; 0.995) of subjects in the FAS (missing values imputed) were responders at maximum frown, as assessed by the investigator, and experienced an improvement of at least one point on the FWS on Day 28 when compared with baseline (Figure 3a). In total, at maximum frown, 46 (43.8%) subjects had moderate and 59 (56.2%) had severe glabellar frown lines at Baseline. On Day 28, 22 (21.0%) subjects had no glabellar frown lines, 65 (61.9%) had mild, 17 (16.2%) had moderate, and one (1.0%) subject had severe glabellar frown lines. The overall response rate was slightly higher in the PPS on Day 28 for maximum frown, with 99.0 percent (n=101; 95% CI: 0.947; 0.998) of subjects treated with incobotulinumtoxinA classed as responders.
{kind=link}
The results of the secondary endpoint analysis showed that response rates at rest, as assessed by the investigators using the FWS, were also high on Day 28, but were lower than at maximum frown, as expected (Figure 3a).
Importantly, results from subject and investigator assessments were consistent. On Day 28, 99.0 and 93.3 percent of subjects FAS achieved an improvement of at least one scale point compared with Day 0 using the PAS at maximum frown and at rest, respectively. At Baseline, at maximum frown, 47 (44.8%) subjects assessed the potency of muscle action as “moderately strong muscle action possible” and 58 (55.2%) as “strong muscle action possible, which may cause local pallor.” On Day 28, 26 (24.8%) subjects assessed “no muscle action at all,” 64 (61.0%) assessed “some even slight muscle action possible,” and 14 (13.3%) assessed “moderately strong muscle action possible.” Regarding PAS assessments at rest, at Baseline, four (3.8%) subjects estimated the degree of their glabellar lines as “slightly visible vertical line(s),” 89 (84.8%) as “moderate vertical line(s) with depression,” and 12 (11.4%) as “deep vertical line(s) and depression, which cannot be effaced by spreading.” On Day 28, 33 (31.4%) subjects reported “no visible vertical line(s) at all,” 56 (53.3%) reported “slightly visible vertical line(s),” and 15 (14.3%) reported “moderate vertical line(s) with depression.” The overall response rates, as assessed by the investigators and subjects, were lower on Day 84 than the corresponding rates on Day 28, as shown in Figure 3b.
The PGA of change in appearance of glabellar frown lines compared with their appearance at Baseline was also self-assessed by study participants. In total, 98.1 percent (n=103 out of a total of 104; 95% CI: 0.933; 0.995) and 85.6 percent (n=89 out of 104; 95% CI: 0.776; 0.911) of subjects (FAS) were classed as responders, with respect to PGA (i.e., achieved a score of at least +2 points), on Days 28 and 84, respectively. The change in appearance, as assessed by the subjects themselves on Days 28 and 84, at maximum frown, is shown in Figure 4.
{kind=link}
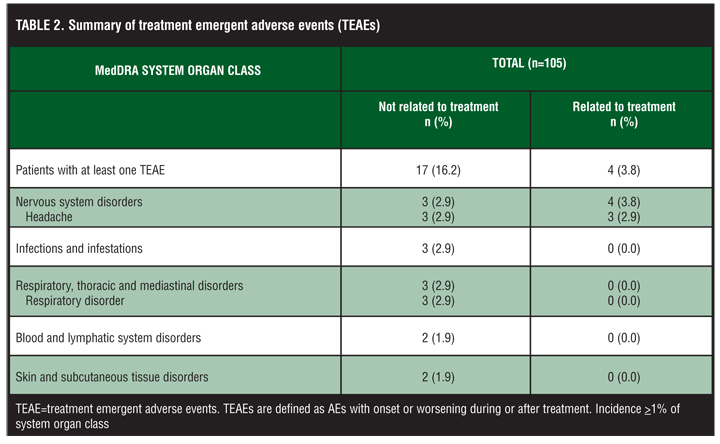
Safety was assessed throughout the study in the 105 subjects who received incobotulinumtoxinA treatment. In total, 21 participants (20.0%) experienced a treatment-emergent AE (TEAE; Table 2). Four subjects (3.8%) experienced TEAEs that were deemed by the investigator to be related to treatment. All were classified as nervous system disorders: headache in three subjects (2.9%) and worsening of pre-existing carotid artery stenosis in one subject (1.0%). One moderate case of a treatment emergent serious AE was reported (fibroadenoma of the breast), but was not considered to be related to treatment. Overall, no safety concerns were raised following analyses of clinical laboratory data and vital signs. No subjects developed neutralizing antibodies against incobotulinum-toxinA and no subject was withdrawn from the study due to AEs.
{kind=link}
Discussion
In this prospective, open-label, Phase III trial, 20U incobotulinumtoxinA demonstrated efficacy and tolerability in the treatment of moderate-to-severe glabellar frown lines, as evaluated by investigators and subjects alike. Overall, 98.1 percent of subjects in the FAS were responders on Day 28 and response rates remained high on Day 84 (80.0%), as assessed by the investigator at maximum frown. The investigator assessment of glabellar frown lines was supported by the subject assessments (99.0% and 76.0% were responders at maximum frown on Day 28 and Day 84, respectively). The response rates for Day 84 were lower than the corresponding values for Day 28, which was to be expected considering the capacity of the body to re-innervate the muscles paralyzed after treatment injection. Similarly, response rates at rest were lower than those reported for maximum frown. This finding is consistent with data from other clinical studies[9] and is not surprising, as wrinkles at rest have a nonmuscle component and may require several treatment cycles to resolve.
The PGA of the appearance of glabellar frown lines also correlated well with the investigator’s assessment, with 98.1 percent of subjects reporting a moderate, marked, or complete improvement in the appearance of their glabellar frown lines on Day 28 as compared to baseline and 85.6 percent reporting at least a moderate improvement on Day 84. Given that client satisfaction is a key treatment goal in facial aesthetics, these results are particularly noteworthy.
The efficacy results presented in this study were not unexpected in light of previous studies with other botulinum toxin A preparations, which demonstrated efficacy in the treatment of glabellar frown lines.[2,3,5–8] Of note, incobotulinumtoxinA has also demonstrated noninferiority to onabotulinumtoxinA in the treatment of glabellar frown lines in a recent, large, head-to-head comparison study, also over 84 days.[9] Another recent study did not detect any differences in therapeutic effect in terms of onset latency, extent, or duration between incobotulinumtoxinA and onabotulinumtoxinA in the treatment of crow’s feet.[23] These findings lend support to the hypothesis that complexing proteins may not have a therapeutic role, but have been implicated in eliciting an immune response.[17,18,24] It is noteworthy that no subjects in this study developed neutralizing antibodies against incobotulinumtoxinA. Cases of antibody-induced therapy failure have been reported in aesthetics following application of complexing protein-containing BTX-A products.[25–27]
As therapy failure associated with long-term use has been increasingly reported, a product lacking complexing proteins, and consequently with less antigenicity, may be preferable.
The incidence of TEAEs in this study was similar to that reported in other studies[28,29] and none of the AEs led to study discontinuation. The AE profile presented in this study is consistent with the known safety profile of incobotulinumtoxinA and is also in line with the profiles of other botulinum toxin preparations.[9,13,30,31]
In summary, incobotulinumtoxinA is an effective therapeutic option for the treatment of glabellar frown lines, according to both investigator and subject assessments, and is well tolerated.
ACKNOWLEDGMENTS
Editorial assistance was provided by Ogilvy 4D, Oxford, United Kingdom. The authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. They gratefully acknowledge the contributions of Vladimir A. Vissarionov and Olga S. Panova.
References
1. Carruthers A, Carruthers J. Botulinum toxin products overview. Skin Therapy Lett. 2008;13:1–4.
2. Carruthers JD, Carruthers JA. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J Dermatol Surg Oncol. 1992;18:17–21.
3. Ascher B, Zakine B, Kestemont P, et al. A multicenter, randomized, double-blind, placebo-controlled study of efficacy and safety of 3 doses of botulinum toxin A in the treatment of glabellar lines. J Am Acad Dermatol. 2004;51: 223–233.
4. Carruthers A, Carruthers J, Lowe NJ, et al. One-year, randomised, multicenter, two-period study of the safety and efficacy of repeated treatments with botulinum toxin type A in patients with glabellar lines. J Clin Res. 2004;7:1–20.
5. Carruthers A, Carruthers J, Said S. Dose-ranging study of botulinum toxin type A in the treatment of glabellar rhytids in females. Dermatol Surg. 2005;31:414–422.
6. Carruthers JA, Lowe NJ, Menter MA, et al. A multicenter, double-blind, randomized, placebo-controlled study of the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J Am Acad Dermatol. 2002;46:840–849.
7. Lowe P, Patnaik R, Lowe N. Comparison of two formulations of botulinum toxin type A for the treatment of glabellar lines: a double-blind, randomized study. J Am Acad Dermatol. 2006;55:975–980.
8. Monheit G, Carruthers A, Brandt F, Rand R. A randomized, double-blind, placebo-controlled study of botulinum toxin type A for the treatment of glabellar lines: determination of optimal dose. Dermatol Surg. 2007;33:S51–S59.
9. Sattler G, Callander M, Grablowitz D, et al. Noninferiority of incobotulinumtoxinA, free from complexing proteins, compared with another botulinum toxin type A in the treatment of glabellar frown lines. Dermatol Surg. 2010;36:2146–2154.
10. Carruthers A, Kiene K, Carruthers J. Botulinum A exotoxin use in clinical dermatology. J Am Acad Dermatol. 1996;34: 788–797.
11. Frevert J. Content of botulinum neurotoxin in Botox®/ Vistabel®, Dysport®/Azzalure®, and Xeomin®/Bocouture®. Drugs R D. 2010;10:67–73.
12. Benecke R, Jost WH, Kanovsky P, et al. A new botulinum toxin type A free of complexing proteins for treatment of cervical dystonia. Neurology. 2005;64:1949–1951.
13. Roggenkämper P, Jost WH, Bihari K, et al. Efficacy and safety of a new Botulinum Toxin Type A free of complexing proteins in the treatment of blepharospasm. J Neural Transm. 2006;113:303–312.
14. Kanovsky P, Slawek J, Denes Z, et al. Efficacy and safety of botulinum neurotoxin NT 201 in poststroke upper limb spasticity. Clin Neuropharmacol. 2009;35:259–265.
15. Inoue K, Fujinaga Y, Watanabe T, et al. Molecular composition of Clostridium botulinum type A progenitor toxins. Infect Immun. 1996;64:1589–1594.
16. Jost WH, Kohl A, Brinkmann S, Comes G. Efficacy and tolerability of a botulinum toxin type A free of complexing proteins (NT 201) compared with commercially available botulinum toxin type A (BOTOX) in healthy volunteers. J Neural Transm. 2005;112:905–913.
17. Lee JC, Yokota K, Arimitsu H, et al. Production of anti-neurotoxin antibody is enhanced by two subcomponents, HA1 and HA3b, of Clostridium botulinum type B 16S toxin-haemagglutinin. Microbiology. 2005;151:3739–3747.
18. Blümel J, Frevert J, Schwaier A. Comparative antigenicity of three preparations on boutlinum neurotoxin A in the rabbit. Neurotox Res. 2006;9:238.
19. Borodic G. Botulinum toxin, immunologic considerations with long-term repeated use, with emphasis on cosmetic applications. Facial Plast Surg Clin North Am. 2007;15(1): 11–16v.
20. Lee SK. Antibody-induced failure of botulinum toxin type A therapy in a patient with masseteric hypertrophy. Dermatol Surg. 2007;33: S105–S110.
21. Dressler D, Wohlfahrt K, Meyer-Rogge E, Wiest L, Bigalke H. Antibody-induced failure of botulinum toxin A therapy in cosmetic indications. Dermatol Surg. 2010;36: 2182–2187.
22. Göschel H, Wohlfarth K, Frevert J, et al. Botulinum A toxin therapy: neutralizing and nonneutralizing antibodies—therapeutic consequences. Exp Neurol. 1997;147:96–102.
23. Prager W, Wissmüller E, Kollhorst B, et al. Comparison of two botulinum toxin type A preparations for treating crow’s feet: a split-face, double-blind, proof-of-concept study. Dermatol Surg. 2010;36:2155–2160.
24. Frevert J, Dressler D. Complexing proteins in botulinum toxin type A drugs: a help or a hindrance? Biologics. 2010;4: 325–332.
25. Borodic G. Immunologic resistance after repeated botulinum toxin type A injections for facial rhytides. Ophthal Plast Reconstr Surg. 2006;22:239–240.
26. Lee S-K. Antibody-induced failure of botulinum toxin type A therapy in a patient with masseteric hypertrophy. Dermatol Surg. 2007;33:S105–110.
27. Dressler D, Wohlfahrt K, Meyer-Rogge E, et al. Antibody-induced failure of botulinum toxin a therapy in cosmetic indications. Dermatol Surg. 2010;36(Suppl 4):2182.
28. Kawashima M, Harii K. An open-label, randomized, 64-week study repeating 10- and 20-U doses of botulinum toxin type A for treatment of glabellar lines in Japanese subjects. Int J Dermatol. 2009;48:768–776.
29. Monheit GD, Cohen JL. Long-term safety of repeated administrations of a new formulation of botulinum toxin type A in the treatment of glabellar lines: interim analysis from an open-label extension study. J Am Acad Dermatol. 2009;61: 421–425.
30. Benecke R, Grafe S, Comes G. Clinical safety of NT201 (Xeomin): A meta analysis. Toxicon. 2008;51:23–24.
31. Dressler D. Comparing Botox and Xeomin for axillar hyperhidrosis. J Neural Transm. 2010;117:317–319.