Gao Yang, MD, Laser Center, Jinshan Hospital, Fudan University, Shanghai, China; Leihong Flora Xiang, MD, PhD Department of Dermatology, Huashan Hospital, Fudan University, Shanghai, China; Michael H. Gold, MD, Gold Skin Care Center, Tennessee Clinical Research Center, Nashville, Tennesee; Vanderbilt University School of Medicine, Department of Dermatology; Vanderbilt University School of Medicine, School of Nursing, Nashville, Tennesee; Huashan Hospital, Fudan University, Shanghai, China; Number One Hospital, China Medical University, Shenyang, China
Abstract
Objective: To investigate the effects of photodynamic intense pulsed light therapy on skin photoaging in Asian skin. Methods: This was a prospective, single-blinded, controlled, clinical trial with 40 patients enrolled. The enrolled patients applied 5% 5-aminolevulinic acid on the left side of the face while a placebo was applied on the right side of the face. After a one-hour incubation, the patients received intense pulsed light therapy. After four treatment cycles, the pH values, transepidermal water loss of the dermis of the forehead and canthus skin, as well as the moisture capacity of stratum corneum and the global score of photoaging were assessed. Results: The pH value of forehead and canthus skin, moisture capacity of stratum corneum, and the dermis of forehead and canthus skin of the photodynamic intense pulsed light therapy treated sides were significantly higher than those of the control sides in all of the patients. The photoaging score decreased after the therapy on both sides, with the photodynamic intense pulsed light therapy treated sides decreasing more than the control sides (P<0.01). Conclusion: 5-aminolevulinic acid photodynamic intense pulsed light therapy showed better effects in the treatment of skin photoaging compared to intense pulsed light therapy alone. (J Clin Aesthetic Dermatol. 2010;3(3):40–43.)
Photoaging is caused primarily by sun exposure, especially ultraviolet light, UVA and UVB. It usually appears in patients before 30 years of age and may be characterized by pigmentation, deep wrinkles, large pores, telengiectasia, and skin relaxation.[1] Several methods have been reported to have positive effects in treating photoaging, such as intense pulsed light (IPL), surgery, drugs, and cosmetic therapy. In today’s experience, the IPL therapy is recognized as one of the most common methods to treat photoaging, as it is safe and effective.[2] To enhance the efficacy of the IPL, the photodynamic intense pulsed light therapy (IPL-PDT) is now widely performed, with the application of a photosensitizer, such as 5-aminolevulinic acid (ALA). However, data concerning the use of IPL-PDT in Chinese individuals are limited.
In this study, the authors investigated the effects of IPL-PDT in the treatment of skin photoaging compared to IPL alone in Chinese patients.
Materials and Methods
Study design and patient enrollment. This is a prospective, single-blinded, clinical trial from one Chinese laser center. Patient inclusion criteria were healthy women between 40 and 55 years of age with moderate photodamage. Exclusion criteria included the topical use of tretinoin, bleaching creams, or glucocorticoid hormones in the three months prior to study entry; facial plastic surgery, rolling, or injection treatment on the facial skin in the six months prior to the first treatment; IPL treatment or other laser therapies in the past; pregnant or lactating during the trial; history of keloids; history of herpes simplex virus infection; psychosis or neurological abnormalities; or other systemic diseases.
During each treatment, the patients had 5% 5-ALA (ALA, 5-aminolevulinic acid, Fudan Zhangjiang, Shanghai, China) applied by clinical coordinators to the left side of the face and a placebo to the right side of the face. After a one-hour incubation, they received IPL therapy by trained study personnel.
A broadband, filtered, IPL source (IPL Quantum, Lumenis, USA) with a cut-off filter of 560nm was applied to all patients. The standard skin rejuvenation treatment parameters were used, with a first pulse set at 3.8msec and the second pulse set at 5.6msec, with a 20msec delay between pulses. The fluence was 24J/cm2. During the remaining treatments, subjects received the same fluence as in the initial treatment.
The patients were instructed to avoid sun exposure for at least 24 hours after each treatment. Each patient received a total of four full-face treatments with the IPL device at one-month intervals.
The photoaging scores were assessed based on a 0 to 4 scale,2 which was recorded at baseline and at the last treatment visit. The scale is defined as follows: 0 = facial skin is smooth to the touch, without significant fine lines or uneven pigmentation including cheeks, forehead, and the canthus area; 1 = either the cheeks, forehead, or the canthus area shows significant roughness, dyspigmentation (hypopigmentation or hyper-pigmentation), or fine lines; 2 = facial skin shows two areas of significant roughness, dyspigmentation, or fine lines or shows roughness, dyspigmentation, and fine lines in one area; 3 = facial skin shows three areas with significant roughness, dyspigmentation, or fine lines or shows roughness, dyspigmentation, and fine lines in two areas; and 4 = facial skin shows any degree of photodamage greater than 3.
The skin pH value (Skin Analyzer SHP, Courage+Khazaka, Germany), moisture capacity of the skin (moisture Meter-D, moisture Meter-SC, Delfin Technologies Ltd, Finland), and transepidermal water loss (TEWL, Vapo Meter, g/m2h, Delfin Technologies Ltd, Finland) of the forehead and canthus skin, as well as the moisture capacity of stratum corneum and dermis of forehead and canthus skin were evaluated at baseline as well as at the last visit of the study.
Statistical analysis. All data were analyzed with the SPSS software 13.0. Paired t-test was carried out to evaluate the significance of two period differences. Values of p<0.05 were considered to be statistically significant.
Results
Forty patients were enrolled after informed consents were obtained. Two subjects dropped out of the study after the first treatment cycle. In the present study, the authors analyzed data of the 38 patients who had completed the study.
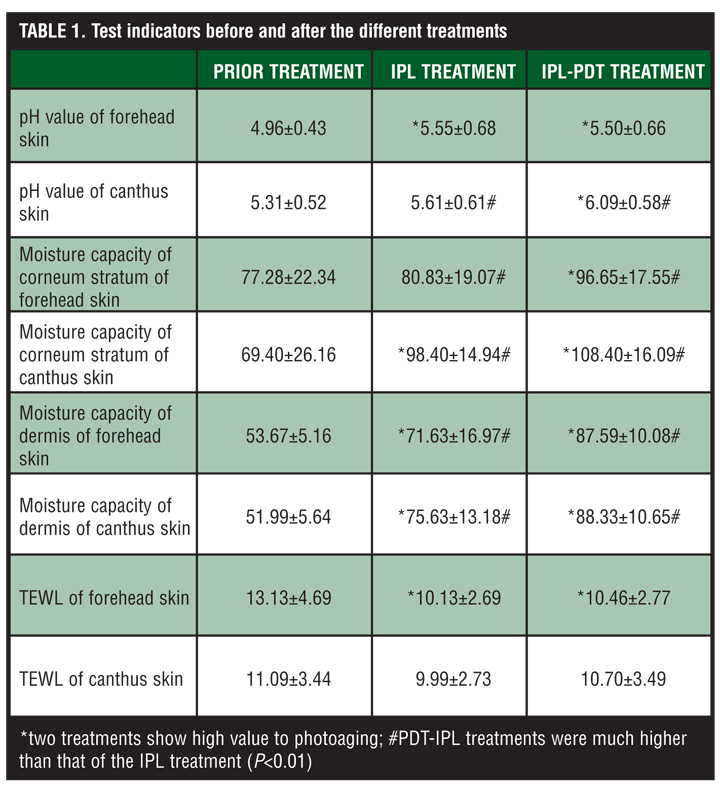
The therapeutic effect of IPL treatment. The pH value of the canthus skin after treatment was significantly increased (p<0.05), but still in the normal range. The pH value of the forehead skin, the moisture capacity of stratum corneum and dermis of canthus skin, and the moisture capacity of dermis of forehead skin were also all increased (p<0.01). The TEWL value of forehead skin was significantly decreased after treatment (Table 1).
{kind=link}
The therapeutic effect of IPL-PDT treatment. The pH value of both the forehead skin and canthus skin, the moisture capacity of corneum stratum, and the dermis of both the forehead skin and canthus skin were significantly increased after treatments (p<0.01). The TEWL value of forehead skin decreased (p<0.01) (Table 1).
Comparison of IPL and PDT-IPL treatment. The pH value of the canthus skin, the moisture capacity of the corneum stratum, and the dermis of forehead and canthus skin of the PDT-IPL treatments were much higher than that of the IPL treatment (P<0.01) (Table 1).
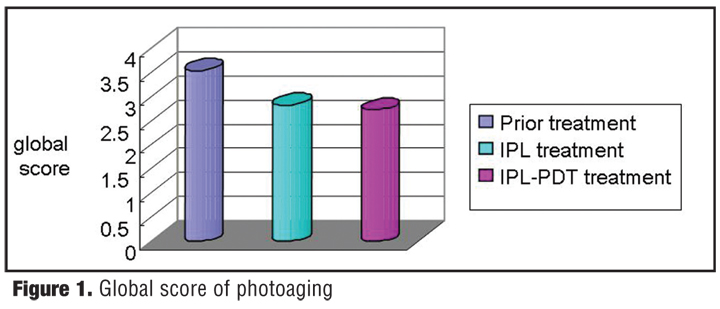
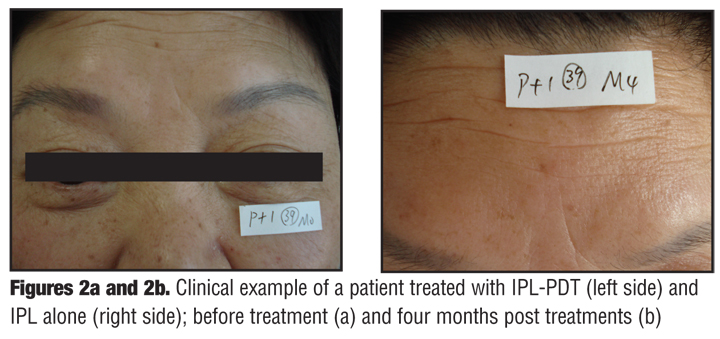
As for the global score for photoaging, both therapies improved photoaging (P<0.01). The improvement of IPL-PDT treatment was more noticeable than the IPL treatment alone (P<0.05), as shown in Table 2 and graphically depicted in Figure 1. Clinical examples are shown in Figures 2a and 2b and Figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The pH value of the skin is related to the skin barrier function. If the pH value of the skin is increased, the activity of stratum corneum chymotryptic enzyme (SCCE) is upregulated to break down the cornedesmosome.[3] TEWL is one of the objective items to investigate the skin barrier function. TEWL levels will change if the skin barrier function is damaged.[4]
Photon therapy, also known as photorejuvenation (PR), works well with IPL to improve a variety of pigmented or vascular lesions, and to promote proliferation and remodeling of collagen fibers to restore skin flexibility.[1] Negishi et al[5] proposed three mechanisms of activation of fibroblasts and collagen synthesis with IPL therapy. First, tissues containing melanin and oxyhemoglobin could selectively absorb IPL energy, which would bring heat to the tissue and lead to thermal damage of collagen fibers. Second, the collagen fibers’ self-absorption of light could induce thermal damage. And third, the nonselective absorption of the heat of the dermis leads to thermal damage of collagen fibers. Based on the mechanism of selective photothermolysis, the 560 to 1200nm spectrum of IPL can be used to treat vascular and pigmented lesions with its effects on mature melanin, hemoglobin, and collagen fibers. It represents a noninvasive, effective cosmetic technology.[6]
Photodynamic therapy (PDT) is an unusual clinical application of a photochemical reaction. It has been used in cancer therapy.[7] In the procedure, a photosensitive medicine (photosensitizer) is applied to the target site before treatment. Visible light can stimulate exogenous photosensitive molecules (porphyrin, chlorin, phthalocyanine green, etc.) generated by target organs, or endogenous photosensitive molecules induced by precursor drugs, such as 5-ALA, which generates a series of photochemical reactions and photobiological reactions that lead to the achievement of desired therapeutic effect.[8]
PDT has recently been introduced in the field of cosmetic laser therapy, especially in regard to photoaging and the treatment of actinic keratoses. The mechanisms may be related to the intracellular heat shock protein (HSP) and matrix metalloproteinase (MMP). Singlet oxygen generated by PDT photosensitizers may be responsible for oxidative stress-induced Hsp70 expression,[9] which could inhibit PDT-mediated apoptosis,[10] so that the cells can deal with the stress, suggesting Hsp70 may play a role in the skin collagen remodeling.[11] MMP1 and 3mRNA expressions of human dermal fibroblast cells could be induced by the sub-lethal dose (LD10) of ALA (75µmol/L) and red light exposure.[12] MMP can decompose photodamaged collagens and accelerate the formation and deposition of new collagens.[13] Moreover, the therapeutic effect can be strengthened when PDT is combined with IPL exposure to enhance the metabolism of stratum corneum and the collagen synthesis of the dermis and to increase moisturizing factors, while the barrier function of skin is not affected.
Wrinkles are one of the main clinical features of photoaging. Our study demonstrated that both IPL and IPL-PDT have good effects on photoaging. Pretreatment with 5-ALA resulted in greater improvement in the photodamage variables compared with IPL alone with respect to the global score for photoaging in the study of Chinese individuals. This is similar to previous accounts of IPL-PDT effects on photoaging reported in Caucasians.[2,14,15] This report on Asian skin broadens the scope of the improvement noted with ALA-IPL and photoaging with darker skin types as seen in many in the Asian population. However, their effect and the mechanism on pH value of the skin should be further investigated. Furthermore, the dosage of photosensitizers should be strictly defined in order to avoid damage to normal tissue cells.
References
1. Li X, Yu J. Clinical application of non-ablative photonic wrinkles Rejuvenation. J Medical Forum. 2007;28(16): 45–46.
2. Dover JS, Bhatia AC, Stewart B, et al. Topical 5-aminolevulinic acid combined with intense pulsed light in the treatment of photoaging. Arch Dermatol. 2005;141(10):1247–1252.
3. Sato J, Yanai M, Hirao T, Denda M. Water content and thickness of the stratum corneum contribute to skin surface morphology. Arch Dermatol Res. 2000;292: 412–417.
4. Zhao X, Xu A. Impact of non-ablative laser rejuvenation on the transepidermal water loss of murine skin. Chinese Journal of Dermatology. 2005;38(11):689–691.
5. Negishi K, Wakamatsu S, Kushikata N, et al. Full-face photorejuvenation of photodamaged skin by intense pulsed light with integrated contact cooling: initial experiences in Asian patients. Lasers Surg Med. 2002;30(4):298–305.
6. Zhang Y, Guo H, Su F, et al. Treatment of face pigmentation and improvement of face skin quality by intense pulsed light. Journal of Chinese Modern Dermatology. 2005;2(5):388–390.
7. Wang Y, Zhang H, Zhu J. Research of ALA combined with HPD-PDT which induced change of P16 gene and P53 gene of G422 glioma of rats. Applied Laser. 2008;28(5):419-429.
8. Sang H. The present situation in the study on application of photodynamic therapy. J Clin Dermatol. 2002;31(5): 332–334.
9. Gomer CJ, Ryter SW, Ferrario A, et al. Photodynamic therapy-mediated oxidative stress can induce expression of heat shock proteins. Cancer Res. 1996;56(10):2355–2360.
10. Nonaka M, Ikeda H, Inokuchi T. Inhibitory effect of heat shock protein 70 on apoptosis induced by photodynamic therapy in vitro. Photochem Photobiol. 2004;79(1):94–98
11. Wang ML, Liu DL, Yuan Q. Effect of intense pulsed light on heat shock protein 70 expression in skin. Di Yi Jun Yi Da Xue Xue Bao. 2005;25(1):109–110.
12. Karrer S, Bossershoff AK, Weiderer P, et al. Influence of 5-aminolevulinic acid and red light on collagen metabolism of human dermal fibroblasts. J Invest Dermatol. 2003;120(2): 325–331.
13. Orringer JS, Kang S, Johnson TM, et al. Connective tissue remodeling induced by carbon dioxide laser resurfacing of photo-damaged human skin. Arch Dermatol. 2004;140(11):1326–1332.
14. Gold MH, Zhou Xi. Topical 5-aminolevulinic acid with intense pulsed light versus intense pulsed light for photodamage in Chinese patients. Dermatol Surg. Submitted for publication.
15. Marmur ES, Phelps R, Goldberg DJ. Ultrastructural changes seen after ALA-IPL photorejuvenation: a pilot study. J Cosmet Laser Ther. 2005;7(1):21–24.