by James J. Leyden, MD, Department of Dermatology, University of Pennsylvania, Philadelphia, and the Skin Study Center, KGL, Inc., Broomall, Pennsylvania; Norman Preston, PhD; Galderma Laboratories, L.P., Fort Worth, Texas; Cris Osborn, PhD; Galderma Laboratories, L.P.; Ronald W. Gottschalk, MD, Galderma Laboratories, L.P.
Disclosure: Dr. Leyden is a consultant for Galderma Laboratories, L.P. Drs. Preston, Osborn, and Gottschalk are employees of Galderma Laboratories, L.P. This study was funded by Galderma Laboratories, L.P.
Abstract
Background: A gel combination treatment containing a retinoid (adapalene 0.1%) and an antimicrobial (benzoyl peroxide 2.5%) has been shown to be an effective treatment for acne vulgaris, addressing three of the four pathogenic factors (hyperkeratinization, Propionibacterium acnes proliferation, inflammation) without contributing to the incidence of Propionibacterium acnes antibiotic resistance as neither the retinoid nor benzoyl peroxide creates selective pressure for resistance. Objective: To evaluate the effectiveness of an adapalene-benzoyl peroxide gel combination in reducing antibiotic-sensitive and resistant strains of Propionibacterium acnes on the facial skin of volunteers. Methods: This four-week, open-label, single-center study included 30 healthy adults with high facial Propionibacterium acnes populations [>104 colony-forming units per square centimeter of skin (CFU/cm2)] and presence of subpopulations resistant to erythromycin, tetracycline, and clindamycin. The gel was applied once daily to the forehead. Cultures for total and antibiotic-resistant Propionibacterium acnes were obtained from the forehead area at screening, Baseline, Week 2, and Week 4. Results: Total Propionibacterium acnes counts decreased by 1.1 log10 CFU/cm2 after two weeks of treatment, and by 1.6 log10 CFU/cm2 after four weeks. All subjects had strains resistant to each of the five antibiotics at baseline. Mean counts of erythromycin and clindamycin resistant Propionibacterium acnes were high at baseline (5.37 and 5.28 log10 CFU/cm2, respectively) and decreased by ?2.1 log10 by Week 4 (P<0.001). Mean counts of strains resistant to tetracyclines were lower at baseline (3.8 to 4.2 CFU/cm2) and decreased by 1.9 (tetracycline), 2.4 (minocycline), and 1.3 (doxycycline) log10 CFU/cm2 by Week 4 (P<0.001). Limitations: Although limited in scope, the results of the present study demonstrate that the fixed-dose combination gel containing adapalene 0.1% and benzoyl peroxide 2.5% effectively inhibited both antibiotic-susceptible and antibiotic-resistant Propionibacterium acnes. In addition to reducing population densities, therapy with adapalene-benzoyl peroxide eradicated some resistant strains entirely in some individual subjects. Conclusion: Topical adapalene-benzoyl peroxide gel effectively reduced skin colonization by antibiotic-sensitive and antibiotic-resistant Propionibacterium acnes after four weeks. This trial was registered with ClinicalTrials.gov (http://clinicaltrials.gov/), registry number NCT00907101.
(J Clin Aesthet Dermatol. 2011;4(5):22–26.)
The pathogenesis of acne is multifactorial and includes sebaceous follicle obstruction, excessive sebum production due to hormonal stimulation of sebaceous glands, proliferation of Propionibacterium acnes, which produces chemotactic factors and proinflammatory mediators that, in turn, generate an inflammatory response, followed by follicular rupture and extension of inflammation into the dermis, resulting in the formation of inflammatory lesions.[1,2]
As P. acnes proliferation in sebaceous follicles plays a central role in the pathophysiology of inflammation in acne, a primary mode of action for benzoyl peroxides (BPOs) and topical antibiotics is through inhibition of P. acnes in vivo as demonstrated by a 1.0 to 2.0 logarithmic (base 10) reduction.[3–7] Strains of P. acnes that are insensitive or resistant to antibiotics commonly used in the treatment of acne can also be found on the skin of acne patients worldwide.[8–16] In these studies, higher minimum inhibitory concentration (MICs) were found for erythromycin followed by clindamycin, and most erythromycin-resistant strains also showed varying levels of insensitivity to clindamycin.[8] Resistance to tetracycline hydrochloride is also common, and resistance to doxycycline and minocycline is increasing.[4]
Although the clinical significance of P. acnes resistance to antibiotics still remains to be fully elucidated, it is generally believed that the antibacterial activity of antibiotics plays an important role in their efficacy in acne, and that the high prevalence of antibiotic-resistant P. acnes on the skin of acne patients may compromise the efficacy of oral or topical antimicrobial treatment for acne.[4,8,9,11,17]
Based on the trend of decreased sensitivity to the antibiotics typically used in acne, as well as the trend in decreased efficacy and even nonresponse to these agents, new research has focused on 1) the development of optimum methods of use of antibiotics in acne management to preserve the utility of these drugs (i.e., in combination with BPO to help minimize the development of resistance), and 2) the development of nonantibiotic therapies to potentially minimize the risk of community antibiotic resistance.[18,19]
In 2003 and 2009, the Global Alliance to Improve Outcomes in Acne issued recommendations stressing that, in order to effectively address as many acne pathogenic factors as possible while minimizing side effects, a rational approach to acne management was to use multiple agents at the same time during treatment (concomitant therapy).[20,21] Some of the treatment recommendations include lower concentrations of BPO (2.5%, 5%) and topical retinoids (adaplene 0.1%, tretinoin microsphere 0.04%, tazarotene 0.05%).
One such commercially available, antibiotic-free, therapeutic option for the treatment of acne is a fixed-dose, once-daily gel combining adapalene 0.1%, a well-tolerated and efficacious topical retinoid, and BPO 2.5%, a well-established nonantibiotic antimicrobial agent (Epiduo® Gel, Galderma Laboratories, L.P., Fort Worth, Texas). Three randomized, double-blind, vehicle- and placebo-controlled clinical trials have established the safety and efficacy of adapalene-BPO gel in the treatment of acne and have shown that this fixed-dose combination gel is significantly more effective than the corresponding monotherapies of BPO alone or adapalene alone.[22–24] Retinoids such as adapalene help normalize the abnormal desquamation of follicular keratinocytes (comedogenesis) and have some anti-inflammatory properties.[25] Adapalene itself possesses anticomedogenic and anti-inflammatory properties.[26–29] The antimicrobial BPO, an oxidizing agent with antibacterial and keratolytic effects, is widely used in acne treatment for its activities in decreasing the bacterial population of P. acnes.[30–33] Thus far, no microbial resistance to BPO has been described. In addition, the nonclinical and clinical safety profile of BPO has been well established.[34]
Because neither the retinoids nor BPO create selective pressure for resistance, this combination may also be expected to decrease the incidence of epidermal bacterial resistance relative to antibiotics. This study was conducted to assess the ability of adapalene 0.1%/benzoyl peroxide 2.5% gel (adapalene-BPO gel) to reduce the numbers of sensitive and resistant strains of P. acnes in subjects who are colonized with these bacteria.
Methods
This study was conducted in June and July 2009 in the United States in accordance with the ethical principles originating from the Declaration of Helsinki and Good Clinical Practices and in compliance with all regulatory requirements. The protocol was reviewed and approved by an institutional review board. Prior to the performance of any study procedures, written informed consent was obtained from all participants.
Subjects. The volunteers selected for the study were healthy adult men and women 18 years of age and older who showed a high degree of fluorescence of the facial skin under a Wood’s lamp indicating the presence of high levels of P. acnes. Because the objective of this study was to evaluate pattern of P. acnes sensitivity and resistance to antibiotics, the primary inclusion criteria focused on the presence of insensitive or resistant bacteria on the skin of the panel volunteers, rather than whether or not they displayed active acne. Subjects were further screened to ensure that none of them had used any form of topical or systemic antibiotics within four weeks prior to enrollment. They were instructed not to use any antimicrobial topical products (e.g., soaps, medicated shampoos, acne preparations) or systemic antibiotics for the duration of the study. Baseline samples taken from the facial skin (forehead) were to confirm P. acnes counts of >104 CFU/cm2. In addition, subjects presented with P. acnes with high MICs to erythromycin (>512µg/mL), varying high MICs to clindamycin (8 to >512µg/mL), and MICs greater than 2µg/mL for tetracycline.
Adapalene-BPO gel application. Adapalene-BPO gel was applied topically once a day to the entire forehead area for 28 days. Once-daily treatment was applied by each subject under supervision by a technician at the study center in a standardized manner (Monday–Friday); application on weekends was unsupervised. Prior to each daily application, the subjects washed their face, patted dry, and allowed to dry thoroughly. They were instructed to use enough test material to cover the forehead from temple to temple. After the application was complete, they were instructed to wash their hands.
Collection and processing of bacterial samples. Quantitative cultures were collected from the surface of the forehead at screening, baseline, Week 2, and Week 4 using a modification of the detergent scrub method of Williamson and Kligman.[35,36] The forehead was cleansed of surface aerobic bacteria by thoroughly wiping the area for 30 seconds with sterile gauze soaked with 0.1% Triton-X-100 (Sigma-Aldrich, Inc., St. Louis, Missouri) to remove surface debris and bacteria. The surface area to be cultured (3.8cm2) was then delineated by a sterile plastic template held firmly to the skin. A cotton-tipped swab was first moistened in 2mL of wash solution (Bacto Letheen Broth, Difco, Sparks, Maryland) and used to swab the forehead area for 30 seconds. The swab tip was then placed into 2mL of wash solution, and the bacteria were released by wringing the swab on the side of the tube. The procedure was repeated on the same skin area with the same swab. The swab was then broken into the 2mL of wash solution. The sample was serially diluted using 0.05% Tween-80 (Sigma-Aldrich, Inc.) (buffered with 0.075M phosphate buffer, pH 7.9) in four 10-fold dilutions. Using a micropipettor, 0.05mL aliquots of each dilution were placed onto plates of Brucella agar (Neogen, Lansing, Michigan) supplemented with yeast extract, dextrose, and cysteine, with and without antibiotics, each on duplicate plates. Serial antibiotic incorporation plates with 1, 2, 4, 8, 16, 32, 64, 128, and 512µg/mL were made fresh the day before subjects were to be cultured. Cultures were placed in an anaerobic jar with BBL Gas Pak Plus anaerobic system envelope and were incubated anaerobically at 35 to 37°C for seven days. Representative colonies on each medium were counted at the dilution that contained between 10 and 100 CFUs, and the number of viable P. acnes colonies was expressed as the average (of both plates) of the log10 CFU/cm2 skin.
In the study screening phase, culture samples were plated in Brucella agar with incorporation of erythromycin 8µg/mL and tetracycline hydrochloride 2µg/mL. All antibiotic incorporation plates were prepared the day prior to use to ensure that the antibiotic had not degraded (tetracyclines degrade after 2–4 days). Another check on the stability of the incorporated antibiotics was the plating of strains known to be sensitive to tetracyclines.
Statistical analysis. The primary analysis was conducted on P. acnes log10 CFU/cm2 testing the null hypothesis that the change from Baseline at Week 2 and Week 4 was zero versus the alternative hypothesis that the change from Baseline was less than zero. The Shapiro-Wilk normality test was performed on the difference between quantitative bacteriology measurements at Baseline and each post-baseline visit. If the difference between quantitative bacteriology measurements at the two time points was normally distributed, a t-test on the difference was performed. If the difference was not normally distributed, then the Wilcoxon signed rank test on the difference was used. Additionally, the percent change from baseline in P. acnes log10 CFU/cm2 was calculated using the formula (10x-10y)/10y x 100, where 10x was the log10 CFU/cm2 at Week 2 or Week 4, and 10y was the log10 CFU/cm2 at Baseline.
Results
A total of 44 suitable subjects were microbiologically screened. Of these, 30 met the microbiological entry criteria of >104 CFU/cm2 skin with prospectively defined levels of resistance and all were included in this analysis. The 30 subjects entered into the study (22 male and 8 female) were all Caucasian except for one subject who was African American. Age ranged from 19 to 61 years (average 36 years). All 30 subjects completed the 28-day treatment to the forehead with 100-percent adherence, and all attended the Week 2 and Week 4 visits. None of the subjects had used topical or oral antibiotics within four weeks prior to the screening visit.
MICs of P. acnes strains at Baseline. This panel of 30 subjects had strains of P. acnes both sensitive and insensitive to all five antibiotics tested (Table 1). All subjects had strains with high MICs to erythromycin (?512µg/mL) and varying sensitivity to clindamycin (ranging from 8 to 1,024µg/mL), similar to those seen in published series.2 In the tetracycline family, all subjects had strains of P. acnes with low MICs ranging from 2 to 16µg/mL. Thus, all 30 subjects had populations of multiple antibiotic-resistant P. acnes.
{kind=link}
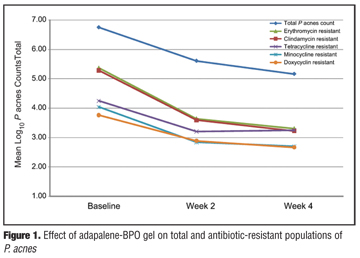
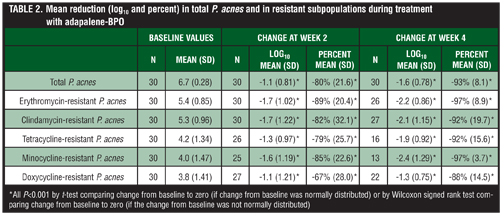
Population density of total and antibiotic-resistant P. acnes. Daily application of adapalene-BPO gel resulted in significant reductions in total P. acnes counts and in counts of all antibiotic-resistant strains after two weeks and four weeks of treatment (Figure 1 and Table 2). The results of the quantitative bacteria cultures demonstrated a significant decline in the mean total P. acnes counts present at Week 2 and Week 4 with a reduction of 1.1 log10 CFU/cm2 (80% reduction) at Week 2 (P<0.001) and 1.6 log10 CFU/cm2 (93% reduction) at Week 4 (P<0.001).
{kind=link}
{kind=link}
Baseline mean counts of resistant P. acnes were highest for erythromycin and clindamycin (5.37 and 5.28 log10 CFU m2, respectively) and these counts decreased by 2.2 (97% reduction) and 2.1 log10 (92% reduction), respectively, after four weeks of treatment with adapalene-BPO gel (P<0.001). Baseline mean counts of strains resistant to tetracycline, minocycline, or doxycycline were lower (3.8–4.2 CFU/cm2) and were reduced by 1.9 (92% reduction; tetracycline), 2.4 (97% reduction; minocycline), and 1.3 (88% reduction; doxycycline) log10 CFU/cm2 by Week 4 (P<0.001). Thus the number of erythromycin- and clindamycin-resistant bacteria was reduced by several orders of magnitude reduction, while the bacteria resistant to one or more of the tetracyclines decreased to levels close to total eradication.
Conclusion
Although limited in scope, the results of the present study demonstrate that the fixed-dose combination gel containing adapalene 0.1% and BPO 2.5% effectively inhibited both antibiotic-susceptible and antibiotic-resistant P. acnes, reducing the bacterial populations by 97 percent after four weeks of application. In addition to reducing population densities, therapy with adapalene-BPO eradicated some resistant strains entirely in some individual subjects.
With the growing incidence of antibiotic-resistant P. acnes on the skin of patients with acne, adapalene-BPO gel provides clinicians and patients with a combination product that is effective against acne, is well tolerated, and is also effective against antibiotic-resistant P. acnes. This makes adapalene-BPO gel a therapeutic option for treating acne in patients with resistant P. acnes while minimizing the development of further antibiotic resistance.
Acknowledgment
The authors would like to acknowledge the role of Christiane Baud, PhD, in preparation of the manuscript.
References
1. Strauss JS, Thiboutot DM. Diseases of the sebaceous glands. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Fitzpatrick’s Dermatology in General Medicine. Vol 1. New York (NY): McGraw-Hill; 1999:769–784.
2. Pawin H, Beylot C, Chivot M, et al. Physiopathology of acne vulgaris: recent data, new understanding of the treatments. Eur J Dermatol. 2004;14:4–12.
3. Gans EH, Kligman AM. Comparative efficacy of clindamycin and benzoyl peroxide: in-vivo suppression of Propioni-bacterium acnes. J Dermatol Treat. 2002;13:107–10.
4. Leyden JJ, Wortzman M, Baldwin EK. Antibiotic-resistant Propionibacterium acnes suppressed by a benzoyl peroxide cleanser 6%. Cutis. 2008;82(6):417–421.
5. Del Rosso J. Benzoyl peroxide cleansers for the treatment of acne vulgaris: status report on available data. Cutis. 2008;82:336–342.
6. Cunliffe WJ, Holland KT, Bojar R, Levy SF. A randomized, double-blind comparison of a clindamycin phosphate/benzoyl peroxide gel formulation and a matching clindamycin gel with respect to microbiologic activity and clinical efficacy in the topical treatment of acne vulgaris. Clin Ther. 2002;24(7): 1117–1133.
7. Leyden J, Kaidbey K, Levy SF. The combination formulation of clindamycin 1% plus benzoyl peroxide 5% versus 3 different formulations of topical clindamycin alone in the reduction of Propionibacterium acnes. An in-vivo comparative study. Am J Clin Dermatol. 2001;2(4):263–266.
8. Leyden JJ, McGinley KJ, Cavalieri S, Webster GF, et al. Propionibacterium acnes resistance to antibiotics in acne patients. J Am Acad Dermatol. 1983;8:41–45.
9. Eady EA, Cove JH, Holland KT, Cunliffe WJ. Erythromycin resistant propionibacteria in antibiotic treated acne patients: association with therapeutic failure. Br J Dermatol. 1989;121:51–57.
10. Cooper AJ. Systematic review of Propionibacterium acnes resistance to systemic antibiotics. Med J Aust. 1998;169:259–261.
11. Dreno B, Reynaud A, Moyse D, et al. Erythromycin resistance of cutaneous bacterial flora in acne. Eur J Dermatol. 2001;11:549–553.
12. Tan HH, Goh CL, Yeo MG, Tan ML. Antibiotic sensitivity of Propionibacterium acnes isolates from patients with acne vulgaris in a tertiary dermatological referral centre in Singapore. Ann Acad Med Singapore. 2001;30:22–25.
13. Ross JI, Snelling AM, Eady EA, et al. Phenotypic and genotypic characterization of antibiotic-resistant Propioni-bacterium acnes isolated from acne patients attending dermatology clinics in Europe, the USA, Japan and Australia. Br J Dermatol. 2001;144:339–346.
14. Coates P, Vyakrnam S, Eady EA, et al. Prevalence of antibiotic-resistant propionibacteria on the skin of acne patients: 10-year surveillance data and snapshot distribution study. Br J Dermatol. 2002;146:840–848.
15. Ross JI, Snelling AM, Carnegie E, et al. Antibiotic-resistant acne: lessons from Europe. Br J Dermatol. 2003;148: 467–478.
16. Ozolins M, Eady EA, Avery AJ, et al. Comparison of five antimicrobial regimens for treatment of mild to moderate inflammatory facial acne vulgaris in the community: randomised controlled trial. Lancet. 2004;364:2188–2195.
17. Webster GF. Acne vulgaris. BMJ. 2002;325:475–478.
18. Tanghetti E. The impact and importance of resistance. Cutis. 2007;80(1 Suppl):5–9.
19. Leyden JJ, Del Rosso JQ, Webster JF. Clinical considerations in the treatment of acne vulgaris and other inflammatory skin disorders: a status report. Dermatol Clin. 2007:27;1–15
20 Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49(Suppl):S1–37.
21. Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne Group. J Am Acad Dermatol. 2009;60(5 Suppl):S1–50.
22. Thiboutot DM, Weiss J, Bucko A, et al. Adapalene-benzoyl peroxide, a fixed-dose combination for the treatment of acne vulgaris: results of a multicenter, randomized double-blind, controlled study. J Am Acad Dermatol. 2007;57:791–799.
23. Gollnick HP, Draelos Z, Glenn MJ, et al Adapalene-benzoyl peroxide, a unique fixed-dose combination topical gel for the treatment of acne vulgaris: a transatlantic, randomized, double-blind, controlled study in 1670 patients. Br J Dermatol. 2009;161(5):1180–1189.
24. Gold LS, Tan J, Cruz-Santana A, et al. A North American study of adapalene-benzoyl peroxide combination gel in the treatment of acne. Cutis. 2009;84(2):110–116.
25. Wolf JE Jr. Potential anti-inflammatory effects of topical retinoids and retinoid analogues. Adv Ther. 2002;19(3): 109–118.
26. Gollnick H, Schramm M. Topical drug treatment in acne. Dermatology. 1998;196(1):119–125.
27. Brogden RN, Goa KE. Adapalene. A review of its pharmacological properties and clinical potential in the management of mild to moderate acne. Drugs. 1997;53(3):511–519.
28. Michel S, Jomard A, Démarchez M. Pharmacology of adapalene. Br J Dermatol. 1998;139 Suppl 52:3–7.
29. Shroot B, Michel S. Pharmacology and chemistry of adapalene. J Am Acad Dermatol. 1997;36(6 Pt 2):S96–S103.
30. Tanghetti EA, Popp KF. A current review of topical benzoyl peroxide: new perspectives on formulation and utilization. Dermatol Clin. 2009;27(1):17–24.
31. Waller JM, Dreher F, Behnam S, et al. ‘Keratolytic’ properties of benzoyl peroxide and retinoic acid resemble salicylic acid in man. Skin Pharmacol Physiol. 2006;19(5):283–289.
32. Fanta D, Bardach H, Poitscheck C. Investigations on the bacteriostatic effect of benzoyl peroxide. Arch Dermatol Res. 1979;264(3):369–371.
33. Fulton JE Jr, Farzad-Bakshandeh A, Bradley S. Studies on the mechanism of action to topical benzoyl peroxide and vitamin a acid in acne vulgaris. J Cutan Pathol. 1974;1(5):191–200.
34. Fakhouri T, Yentzer BA, Feldman SR. Advancement in benzoyl peroxide-based acne treatment: Methods to increase both efficacy and tolerability. J Drugs Dermatol. 2009;8(7):657–661.
35. Williamson P, Kligman AM. A new method for the quantitative investigation of cutaneous bacteria. J Invest Dermatol. 1965;45:498–503.
36. Keyworth N, Millar MR, Holland, KT. Swab-wash method for quantitation of cutaneous microflora. J Clin Microbiology. 1990;28:941–943.
37. Pagnoni A, Kligman AM, Kolias N, et al. Digital fluorescence photography can assess the suppressive effect of benzoyl peroxide on Propionibacterium acnes. J Am Acad Dermatol. 1999;41:710–716.
38. Bojar RA, Cunliffe WJ, Holland KT. The short-term treatment of acne vulgaris with benzoyl peroxide: effects on the surface and follicular cutaneous microflora. Br J Dermatol. 1995;132:204–208.
39. Nacht S, Gans EH, McGinley KJ, Kligman AM. Comparative activity of benzoyl peroxide and hexachlorophene. In-vivo studies against Propionibacterium acnes in humans. Arch Dermatol. 1983;119:577–579.
40. Burkhart CN, Burkhart CG. Microbiology’s principle of biofilms as a major factor in the pathogenesis of acne vulgaris. Int J Dermatol. 2003;42(12):925–927.
41. Coenye T, Honraet K, Rossel B, Nelis HJ. Biofilms in skin infections: Propionibacterium acnes and acne vulgaris. Infect Disord Drug Targets. 2008;8(3):156–159.