
Lawrence F. Eichenfield, MD, Rady Children’s Hospital, San Diego, and University of California San Diego, San Diego, California; Diane Thiboutot, MD, Penn State University College of Medicine, Hershey, Pennsylvania; Alan Shalita, MD, SUNY Downstate Medical Center, Brooklyn, New York; Leonard Swinyer, MD, Dermatology Research Center, Salt Lake City, Utah; Emil Tanghetti, MD, Center for Dermatology and Laser Surgery, Sacramento, California; Eduardo Tschen, MD, Academic Dermatology Associates, Albuquerque, New Mexico; Lisa Parr, PharmD, Clinical Affairs Department, OMP, Inc., Long Beach, California
Disclosure: Dr. Eichenfield has served as an investigator and past consultant for Obagi, Stiefel, and Galderma. Dr. Thiboutot has served as a clinical investigator and consultant for Obagi. Dr. Shalita is a consultant for Galderma, Medicis, and Stiefel. Drs. Swinyer and Tschen report no relevant conflicts of interest. Dr. Tanghetti is an investigator, speaker, and consultant for Allergan, Stiefel, and Obagi and is an investigator and speaker for Galderma. Dr. Parr, at the time of the study, was employed by and owned stock options in Obagi Medical Products, Inc. Financial support for this study was provided by OMP, Inc.
Objective. To evaluate the clinical benefit in adolescents of a three-step acne system containing solubilized benzoyl peroxide. Design. Patients in this multicenter, investigator-blind trial were randomly assigned to receive 10 weeks of treatment with either the three-step acne system for normal-to-oily skin (proprietary 2% salicylic acid cleanser twice daily + proprietary 2% salicylic acid toner once daily + solubilized 5% benzoyl peroxide gel twice daily) or with control cleanser + 5% benzoyl peroxide/1% clindamycin gel twice daily. Setting. Patients seeking acne treatment from a dermatologist. Pediatric subgroup analysis from a larger trial. Participants. Eighty-two adolescents with mild-to-moderate facial acne vulgaris. Measurements. Noninflammatory and inflammatory lesion counts, erythema, dryness, peeling, burning/stinging, and itching. Results. The three-step acne system was significantly more effective than benzoyl peroxide/clindamycin in reducing the noninflammatory lesion count at Weeks 2 and 4. The antibiotic-free acne system was also comparably effective to benzoyl peroxide/clindamycin in reducing the inflammatory lesion count at all timepoints. Both regimens were generally well tolerated with mean levels of erythema, dryness, peeling, burning/stinging, and itching less than mild in both groups at all timepoints. Conclusions. The three-step acne system is an effective antibiotic-free acne treatment. Relative to benzoyl peroxide/clindamycin, its ability to achieve comparable reductions in inflammatory lesions, and significantly greater reductions in noninflammatory lesions in the early weeks of treatment is likely attributable to the solubilization of the benzoyl peroxide enhancing the bioavailability and intrafollicular penetration of the benzoyl peroxide. (J Clin Aesthetic Dermatol. 2009;2(11):21–26.)
Abstract
Benzoyl peroxide (BPO) is a rational first-line treatment for acne vulgaris because it offers good efficacy against both inflammatory and noninflammatory acne lesions.[1] It is also a useful maintenance treatment because, unlike antibiotics, it is not associated with the development of resistance in Propionibacterium acnes or other bacteria.[2–4] However, BPO is challenging to formulate—it is only poorly soluble in aqueous vehicles and can aggregate into crystalline clusters that may be too large for intrafollicular penetration. It also tends to be unstable in other solvents.[5]
As a result of these physicochemical issues, the bioavailability, follicular penetration, and clinical efficacy of BPO may be suboptimal. To overcome these limitations, a solubilized formulation of BPO has been developed. This formulation consists of a homogeneous solution of BPO molecules whose diameters are ~0.0001µm. Follicles on the forehead have been reported to have a mean diameter of 66µm[6]; therefore, the solubilized BPO molecules are easily small enough for unhindered follicular penetration. In contrast, some commercially available BPO formulations have BPO cluster diameters up to 100µm, which would hinder follicular penetration.[7]
The solubilized 5% BPO gel formulation has been reported to achieve relatively greater bactericidal activity on the surface of the cheeks and in follicles, and a significantly greater reduction in noninflammatory lesion count, than a BPO/antibiotic combination product.[8,9] Both products resulted in comparable reductions in the inflammatory lesion count despite the absence of antibiotic in the solubilized BPO regimen.[9]
The solubilized 5% BPO formulation is available as part of a three-step acne system for either normal-to-oily skin (used in conjunction with a proprietary 2% salicylic acid cleanser and a proprietary 2% salicylic acid toner) or normal-to-dry skin (used in conjunction with a nonsoap cream cleanser and a noncomedogenic moisturizer containing glycerin and dimethicone).[10]
The results from a clinical study evaluating the three-step acne system for normal-to-oily skin showed that the system was at least as effective as BPO/clindamycin (the formulation packaged in a pump) in reducing the noninflammatory lesion count and may enhance the speed at which these lesions are reduced in the early weeks of treatment. Both products resulted in comparable efficacy against inflammatory lesions and comparable tolerability.[11] We present a subgroup analysis of the pediatric patients in this study to demonstrate the clinical benefit of this three-step acne system, specifically in adolescents.
Materials and Methods
Patients. Patients eligible for enrollment had mild-to-moderate facial acne vulgaris (10–100 noninflammatory lesions, 17–60 inflammatory lesions, and <2 nodulocystic lesions) and were willing to refrain from excessive exposure to ultraviolet (UV) light and the use of any nonstudy acne medications, moisturizers, sunscreens, fragrances, or aftershaves. Only patients aged 11 to 17 years old were included in the subgroup analysis presented here.
Patients were ineligible if they were using other medicated products on their face or had used a medicated facial cleanser in the preceding week; a topical alpha-hydroxy acid or anti-acne medication in the preceding two weeks; a topical retinoid, topical or systemic antibiotic, or topical or systemic steroid in the preceding four weeks; estrogen/birth control pills for less than three months immediately before the baseline visit; or systemic retinoids in the preceding six months.
The study (protocol NOA010) was approved by the relevant institutional review boards and conducted in accordance with the Declaration of Helsinki. All minors signed an assent for the study and informed consents were signed by a parent or legal guardian.
Treatment regimen. In the parent study, patients were randomly assigned (1:1) to 10 weeks of facial treatment with either the three-step acne system for normal-to-oily skin or BPO/clindamycin. The patients assigned to the three-step acne system were instructed to apply a dime-sized amount of the proprietary 2% salicylic acid cleanser twice daily, one pump of the solubilized 5% BPO gel twice daily, and the proprietary 2% salicylic acid toner once daily. The patients in the BPO/clindamycin group were instructed to use a dime-sized amount of the control cleanser twice daily and one pump of the 5% BPO/1% clindamycin gel (pump formulation used, repackaged into study-specific pumps to maintain blinding) twice daily.
All patients were provided with a moisturizer (CLENZIdermTM Therapeutic Moisturizer, OMP, Inc.) and sunscreen (Obagi Nu-Derm® Healthy Skin Protection SPF 35, OMP, Inc.) for use as needed.
Randomization and masking. An independent company prepared a randomization schedule and sealed envelopes containing treatment assignments for each subject number. Each enrolled subject was allocated a number and, after randomization, the unblinded dispensing coordinator opened the relevant sealed envelope and dispensed the assigned treatment. At each site, subject numbers were allocated in order of enrollment and the envelopes were kept locked away with only the dispensing coordinator having access. Subjects were given boxes to transport their study products to and from the clinic.
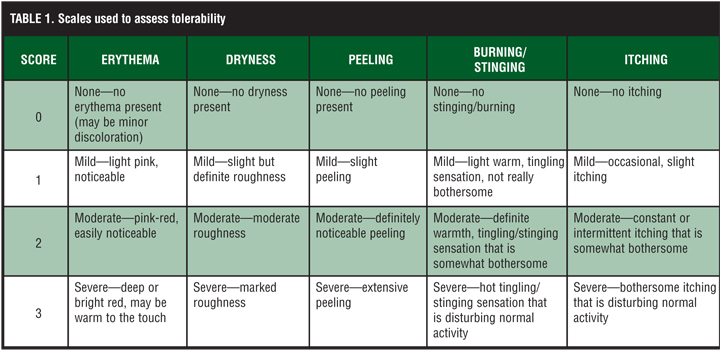
Outcome measures. Efficacy was assessed in terms of reductions in noninflammatory lesion count (open plus closed comedones) and inflammatory lesion count (papules plus pustules plus nodules/cysts). Tolerability was assessed in terms of erythema, dryness, peeling, burning/stinging, and itching using a four-point scale (Table 1).
{kind=link}
Statistical analyses. The sample size of the parent study was not determined using a power analysis approach, but was expected to be large enough to show a clinical difference between groups. Between-group differences were analyzed using a two-sided chi-square test or Fisher’s exact test for gender and race; a two-sided t-test or Wilcoxon rank-sum test for age and baseline lesion counts; Wilcoxon rank-sum test for Fitzpatrick skin type and mean tolerability scores; and analysis of covariance or rank analysis of covariance or Student’s t-test or Wilcoxon rank-sum test for percent change from baseline in lesion count (depending on the importance of the baseline value in analysis of covariance models, and the normality of the residuals and the variable). All statistical evaluations were performed by an independent statistical group and a P value of <0.05 on two-tailed tests was considered statistically significant.
Results
Patients. A total of 82 pediatric patients were evaluated and included in this subgroup analysis (49 were treated with the three-step acne system and 33 with BPO/clindamycin). Among these, six (7%) discontinued prematurely—three due to lack of efficacy (2 with acne system, 1 with BPO/clindamycin), two due to lack of adherence (1 in each group), and one due to treatment-related adverse effects (facial erythema and burning sensation in 1 patient in the acne system group).
The majority of patients were Caucasian (84%), female (57%), and with a Fitzpatrick skin type of II, III, or IV (29%, 34%, and 26%, respectively). Their mean age was 15 years and they had a mean of 58 noninflammatory acne lesions and 29 inflammatory acne lesions at baseline. There were no significant between-group differences in any of these parameters at baseline. The study was conducted between July 2007 and January 2008.
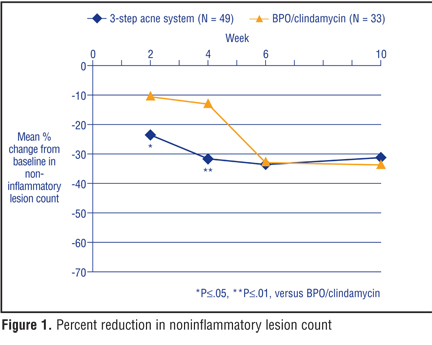
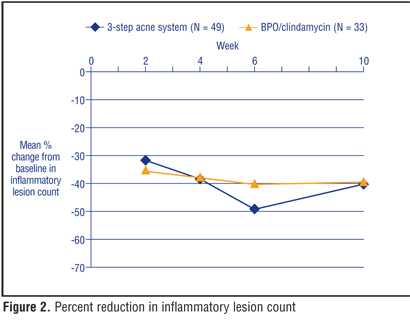
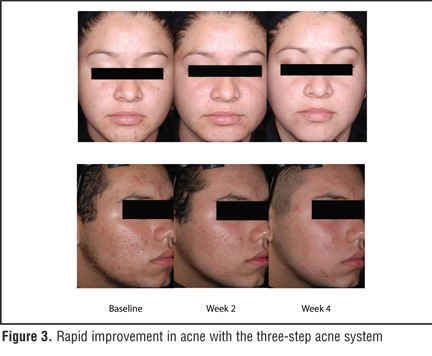
Efficacy. The three-step acne system was associated with a significantly greater mean reduction in noninflammatory lesion count than BPO/clindamycin at Week 2 [23% (±32%) versus 11% (±35%), P<0.05] and Week 4 [32% (±27%) versus 12% (±36%), P<0.01], and comparable reductions thereafter (Figure 1). Both regimens were associated with comparable reductions in inflammatory lesion count at all timepoints (Figure 2). At Week 10, the mean reductions in noninflammatory lesion count and inflammatory lesion count with the three-step acne system and with BPO/clindamycin were 31 percent (±36%) versus 33 percent (±42%), and 40 percent (±35%) versus 40 percent (±32%), respectively. The early clinical improvement in acne with the three-step acne system is demonstrated in Figure 3.
{kind=link}
{kind=link}
{kind=link}
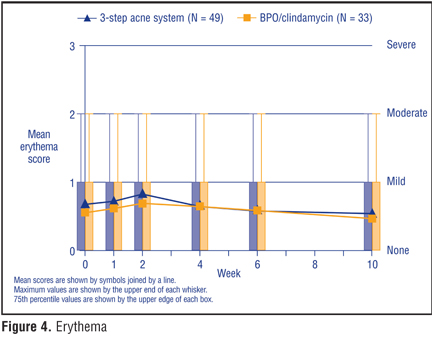
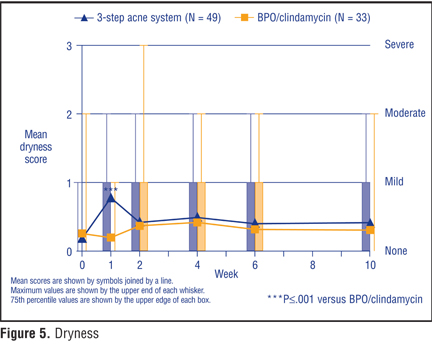
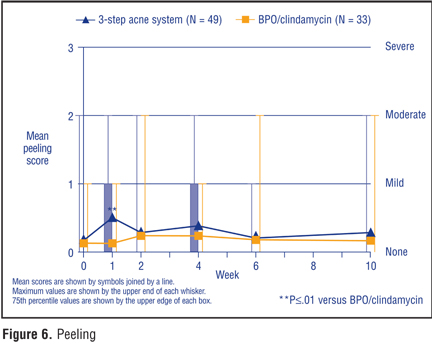
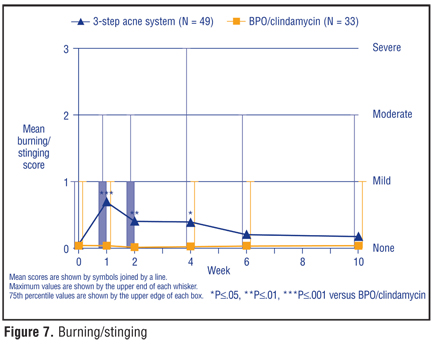
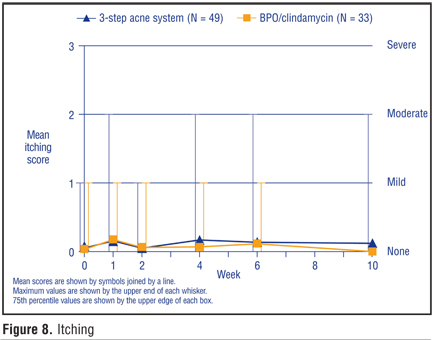
Tolerability. Both treatments were generally well tolerated with mean levels of erythema, dryness, peeling, burning/stinging, and itching less than mild in both groups at all timepoints (Figure 4, Figure 5, Figure 6, Figure 7, Figure 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
There were no significant between-group differences in mean scores for erythema (Figure 4) and itching (Figure 8). Mean scores for dryness and peeling were comparable between groups at all timepoints except at Week 1 when mean levels were transiently significantly higher with the acne system than with BPO/clindamycin (Figure 5 and Figure 6). Mean scores for burning/stinging were significantly higher in the acne system group than in the BPO/clindamycin group at Weeks 1 through 4 (Figure 7). The 75th percentile scores were comparable between groups except for being one point higher in the acne system group than the BPO/clindamycin group for dryness at Weeks 1 and 10 (Figure 5), peeling at Weeks 1 and 4 (Figure 6), and burning/stinging at Weeks 1 and 2 (Figure 7).
Three patients reported treatment-related adverse events on their face (dryness with BPO/clindamycin, erythema and burning sensation, and burning/stinging sensation with the acne system).
Discussion
The results from the pediatric subgroup presented here are similar to those from the overall study population presented previously[11]—that is, compared with BPO/clindamycin, the three-step acne system for normal-to-oily skin resulted in numerically greater reductions in noninflammatory lesion count in the early weeks of treatment, enhanced the speed at which these lesions were reduced, and resulted in comparable reductions in inflammatory lesion count. In the pediatric subgroup, the mean reductions in noninflammatory lesion count were significantly greater with the acne system than with BPO/clindamycin at Week 2 (23% versus 11%) and Week 4 (32% versus 12%). In contrast, although the equivalent between-group differences in the whole study population were considered clinically significant at Week 2 (27% versus 13%) and Week 4 (39% versus 25%), they were not statistically significant. The early attainment of statistical significance in the pediatric subgroup despite the smaller sample size suggests that the three-step acne system is particularly effective in achieving rapid improvements in noninflammatory lesions in adolescents—which is potentially of great clinical benefit given that adolescents are often especially anxious for their acne to resolve quickly. (No conclusions can be drawn about the lack of statistical significance in the entire study population as the study had not been powered to detect statistically significant differences.)
The comparable reductions in inflammatory lesion count with both treatments and across both data sets are notable because they are achieved in the absence of any antibiotic in the three-step acne system group. Although both data sets showed that the three-step acne system was associated with a smaller percent reduction in inflammatory lesion count from baseline at Week 10 than at Week 6, this is likely a transient anomaly in the data with no clinical significance because a longer trial evaluating solubilized BPO alone also showed such a lessening (albeit smaller and between Weeks 4 and 8 and this was transient and had disappeared by Week 12.[9] Consistent with the results from the full study population, both treatments were generally well tolerated in the pediatric subgroup.
The results presented here are derived from the limited number of adolescents (82) who were enrolled in a larger study of 139 patients. While it would be desirable to confirm these results in a larger population of adolescents so as to reduce the effects of interpatient variability and enhance the reliability of the findings, the results are nevertheless similar to those from earlier research in 88 other patients, aged 11 to 45 years.[12] These earlier results showed that the three-step acne system (some patients used only the solubilized 5% BPO gel and 2% salicylic acid toner without the 2% salicylic acid cleanser that is also part of the three-part acne system) was associated with a numerically greater reduction in noninflammatory lesion count than BPO/clindamycin (mean of 37% versus 16%, respectively, at Week 2, and 47% versus 28% at Week 4), comparable reductions in the inflammatory lesion count, and similar tolerability profiles.[12] Furthermore, comparisons of solubilized BPO alone (i.e., without the salicylic acid cleanser and toner) versus BPO/clindamycin showed reductions in noninflammatory lesion count with solubilized BPO that were not dissimilar to those reported elsewhere with the three-step acne system (29–30% at Week 2 and 42–45% at Week 4) in 23 or 65 patients.[9,12,13] These data suggest that the solubilized BPO is the integral component in the three-step acne system that is responsible for the anticomedonal efficacy achieved (and that the between-group differences in anticomedonal efficacy are not attributable to the salicylic acid cleanser and/or toner). Salicylic acid is widely used as a keratolytic in cleansers and toners and in other over-the-counter acne medications and is often used in combination with other agents in order to offer greater overall efficacy. The apparently superior anticomedonal efficacy of the solubilized BPO may be at least partly attributable to the BPO having been solubilized as this may have enhanced the bioavailability and intrafollicular penetration of the BPO.
The ability of the three-step acne system to consistently achieve comparable inflammatory lesion count reductions to BPO/clindamycin affords the opportunity to treat many patients with inflammatory acne without the need for antibiotic exposure. This provides an immediate advantage for patients who prefer to avoid antibiotics and a longer-term advantage for the wider community in terms of reducing the risk of P. acnes and other bacteria developing resistance. Although the use of BPO concomitantly with an antibiotic reduces the risk of antibiotic-resistant bacterial strains developing, it does not eliminate the risk completely.[14] This remains a significant concern not only because it could endanger the effectiveness of antibiotics that are used in treating more severe cases of inflammatory acne, but also because resistance mechanisms can transfer to bacteria that are not closely related genetically.[15] In addition, adverse effects have been reported to be associated with antibiotic use in patients with acne—for example, colonization of the oropharynx with Streptococcus pyogenes[16] and an increased incidence of upper respiratory tract infections.[17]
Acne systems may enhance patient adherence[18] and many patients choose them over single medications—possibly because of the convenience of the system in defining a daily routine providing for both overall skin care and acne treatment. Guidelines recommend switching from antibiotics once clinical improvement has become apparent.[3] Using an antibiotic-free treatment, such as the three-step acne system, from the outset would avoid the inconvenience of discontinuing an initial antibiotic-containing regimen and switching to a maintenance treatment.
The reductions in noninflammatory lesion count with the three-step acne system and solubilized BPO alone are comparable with some reported with topical retinoids.[19–21] However, only the results of direct comparative trials can confirm this suggestion that the three-step acne system may achieve similar anticomedonal efficacy to some topical retinoids.
Acknowledgment
We gratefully acknowledge the contributions of James Q. Del Rosso, DO (Las Vegas Skin & Cancer Clinics, Las Vegas, NV), and the late Robert Loss, MD (Dermatology Associates of Rochester, Rochester, NY), as investigators in this study. We also thank JoAnne Watson, DPM, for managing the clinical operations of this study.
References
1. Belknap BS. Treatment of acne with 5% benzoyl peroxide gel or 0.05% retinoic acid cream. Cutis. 1979;23:856–859.
2. Parry EJ, Griffiths CEM. Bacteria and antimicrobial agents in the treatment of acne. Int J Derm. 1996;35:249–251.
3. Gollnick H, Cunliffe W, Berson D, et al. Management of acne: a report from a Global Alliance to Improve Outcomes in Acne. J Am Acad Dermatol. 2003;49(1 Suppl):S1–S37.
4. Leyden JJ, Del Rosso JQ, Webster GF. Clinical considerations in the treatment of acne vulgaris and other inflammatory skin disorders: focus on antibiotic resistance. Cutis. 2007;79(6 Suppl):9–25.
5. Chellquist EM, Gorman WG. Benzoyl peroxide solubility and stability in hydric solvents. Pharm Res. 1992;9:1341–1346.
6. Otberg N, Richter H, Schaefer H, et al. Variations of hair follicle size and distribution in different body sites. J Invest Dermatol. 2004;122:14–19.
7. Data on file. Long Beach, CA: Obagi Medical Products, Inc.; 2006.
8. Erianne J, Prince DL, Ramirez J, et al. The pharmacologic science of a novel benzoyl peroxide formulation and the implications for clinical effects. Poster presented at: 25th Anniversary Fall Clinical Dermatology® Conference; October 6-9, 2006; Las Vegas, NV. Obagi Medical Products, Inc. website. http://obagi.avisan.com/documents/BPO_
Poster_100206_v2%20(%20Overview).pdf. Accessed on August 21, 2009.
9. Kircik L, Green L, Thiboutot D, et al. Comparing a novel solubilized benzoyl peroxide gel with benzoyl peroxide/clindamycin: final data from a multicenter, investigator-blind, randomized study. J Drugs Dermatol. 2009;8:812–818.
10. CLENZIderm M.D.TM Product Overview. Obagi Medical Products, Inc. http://www.obagi.com/article/forphysicians/ ourproducts/obagiclenzidermmd/products/products.html. Accessed on August 21, 2009.
11. Thiboutot D, Eichenfield L, Shalita A, et al. A 3-step acne system containing solubilized benzoyl peroxide versus clindamycin-benzoyl peroxide. Cutis. 2009;84:48–55.
12. Del Rosso JQ. Evaluation of a solubilized benzoyl peroxide gel: a pooled analysis from 3 randomized investigator-blinded trials. Cos Derm. 2008;21:201–206.
13. Tanghetti E, Kircik L, Wilson D, Dhawan S. Solubilized benzoyl peroxide versus benzoyl peroxide/clindamycin in the treatment of moderate acne. J Drugs Dermatol. 2008;7:534–538.
14. Eady EA, Bojar RA, Jones CE, et al. The effects of acne treatment with a combination of benzoyl peroxide and erythromycin on skin carriage of erythromycin-resistant Propionibacteria. Br J Dermatol. 1996;134:107–113.
15. Mills O Jr, Thornsberry C, Cardin CW, et al. Bacterial resistance and therapeutic outcome following three months of topical acne therapy with 2% erythromycin gel versus its vehicle. Acta Derm Venereol. 2002;82:260–265.
16. Levy RM, Huang EY, Roling D, et al. Effect of antibiotics on the oropharyngeal flora in patients with acne. Arch Dermatol. 2003;139:467–471.
17. Margolis DJ, Bowe WP, Hoffstad O, Berlin JA. Antibiotic treatment of acne may be associated with upper respiratory tract infections. Arch Dermatol. 2005;141:1132–1136.
18. Bowe WP, Shalita AR. Effective over-the-counter acne treatments. Semin Cutan Med Surg. 2008;27:170-176.
19. Webster GF. Topical tretinoin in acne therapy. J Am Acad Dermatol. 1998;39:S38–S44.
20. Differin® (adapalene) cream, 0.1% [package insert]. Fort Worth, Texas: Galderma Laboratories, LP; 2009.
21. Shalita A, Weiss JS, Chalker DK, et al. A comparison of the efficacy and safety of adapalene gel 0.1% and tretinoin gel 0.025% in the treatment of acne vulgaris: a multicenter trial. J Am Acad Dermatol. 1996;34:482–485.